Localized swellings (masses)
Diffuse swellings (Macroglossia)
A. Cystic swellings
Vascular malformations
Retention mucous cyst (ranula)
Multiple neurofibromatosis
Sublingual dermoid cyst
Congenital causes:
Thyroglossal cyst (at foramen cecum)
1. Cretinism (muscle hypertrophy)
Hemangioma
2. Mongolism
Chronic abscess
Glycogen storage disease
Degenerated solid tumor (sarcoma)
Amyloidosis (amyloid infiltration)
Softened gumma or tuberculous (TB) nodule
Diffuse carcinoma
Hydatid cyst
Glossitis
B. Solid swellings
1. Acute glossitis
Stone in Wharton’s duct
2. Chronic diffuse syphilitic glossitis
Neurofibroma
Allergy
Papilloma
Lingual thyroid
Carcinoma (usually an ulcer)
Sarcoma
5.2.1 Ranula
A ranula is a large mucous retention cyst in the floor of the mouth (in Latin, ranula means a small frog) probably due to an unnoticed trauma of the duct system.
It usually occurs in children and young adults, affecting both genders equally. The main complaint is a swelling in the floor of the mouth that usually ruptures and refills. Physical examination reveals a small spherical cyst (only the top 1/2 is seen), about 1–5 cm in size, in the floor of the mouth, between the symphysis menti and the tongue, just to one side of the midline. Ranulae occasionally extend into the submandibular triangle of the neck (plunging ranula or deep cervical ranula). The cyst is characteristically translucent and has a bluish tinge. It is smooth and covered by tortuous veins, and the submandibular duct is displaced and stretched over it. The edge is difficult to feel and the cyst cannot be compressed or reduced.
Treatment options include marsupialisation (deroofing of the cyst and suturing the edges to the floor of the mouth) and total or partial excision of the sublingual gland through an intraoral approach [3].
5.2.2 Sublingual Dermoid Cyst
When the face and neck are formed by the fusion of the facial processes, a piece of skin may get trapped deep in the midline just behind the jaw and later forms a “sublingual dermoid cyst.” Such cysts usually lie in the midline or may be slightly lateral. They may lie above or below the mylohyoid muscle (supra- or infrahyoid, respectively).
It usually occurs between 10 and 25 years, affecting both genders equally. The patient usually complains of a swelling under the tongue, which becomes painful and tender if it gets infected. Physical examination reveals a smooth, clearly defined, spherical swelling, about 2–5 cm in size, occupying the midline between the tongue and the inner surface of the chin. It may bulge into the submental triangle of the neck below the chin. The mucous membrane appears normal. It can be felt bimanually (with one finger in the mouth and the other beneath the chin). It is characteristically opaque and fluctuant.
Treatment is by surgical excision through the oral route rather than the cervical route because of the hidden scar.
5.2.3 Stone in Wharton’s Duct
Stones and infection of the submandibular gland and duct are common. When such a stone migrates to the mouth of the submandibular duct (Wharton’s duct), it forms a tender lump in the floor of the mouth. The lump bulges slightly into the mouth and, through the surrounding edema, feels hard. Occasionally, the surface of the stone can be seen through the open end of the duct. The submandibular gland is usually swollen and tender. The majority of stones (60 %) reside in the proximal duct or hilum of the submandibular gland.
Small mobile stones (<4 mm) could be retrieved (as per parotid) by baskets (via endoscopes and radiologically guided). The extracorporeal lithotripter is relatively inefficient in eliminating submandibular stones (30 % clearance). These stones are dealt with by an intraoral surgical technique either under local anesthetic or day-case general anesthesia. Based on a review of the treatment of 4600 salivary stones, submandibulectomy should be recognized as an uncommon event representing a minority of cases in the modern surgical practice (<3 %) [4].
5.2.4 Vascular Malformations
About 50 % of all vascular anomalies occur in the head and neck regions [5]. Although such lesions are usually of aesthetic concern, a lesion located in the tongue or closely related to the oropharyngeal airway may lead to more serious problems such as spontaneous bleeding or even hematemesis [6]. Though uncommon, progressive asymmetric growth of the tongue (macroglossia) can be also observed. In contrast to hemangiomas, malformations are not neoplasms and thus do not exhibit mitosis or increased endothelial cell turnover. Instead, vascular malformations are defined as structural abnormalities of the capillary, venous, lymphatic, and arterial system that grow in proportion to the child [7].
5.2.4.1 Classification
According to the classification of the International Society for the Study of Vascular Anomalies (ISSVA) approved in April 2014 [8], the vascular malformations were classified according to the origin mainly into four main categories:
1.
Simple (capillary, venous, lymphatic, arteriovenous fistula, arteriovenous malformation)
2.
Combined (lymphatic venous, capillary-lymphatic venous, etc.)
3.
Malformations of major named vessels
4.
Associated with other anomalies
Vascular malformations could be further classified according to the flow pattern into high- and low-flow malformations. The capillary, venous, and lymphatic variants belong to the low-flow pattern group and those with an arterial component belong to the high-flow one. Common vascular malformations in the tongue and oral cavity include venous malformations, arteriovenous fistulae, and lymphatic malformations.
5.2.4.2 Venous Malformations
Pathology
Congenital venous malformations consist of either localized or diffuse ectatic veins with abnormal collections of irregular venous channels. Although mostly in the skin, venous malformations are also commonly found in the cheek, tongue, lip, and mandible. They may be present in deep tissue, bone, muscle, or brain. Recently a loss-of-function mutation was discovered on the angiopoietin receptor gene TIE2/TEK in many solitary and multiple sporadic venous malformations [9]. In addition, upregulation of several factors including tissue growth factor beta (TGF-beta) and basic fibroblast growth factor (beta-FGF) has been also discovered in patients with venous malformations [10].
Clinical Presentation
A venous malformation is always present at birth but is not always evident. They may first become noticeable in childhood or even adulthood and they do not spontaneously involute. Small lesions are usually asymptomatic or the patients may complain only of disfigurement. Intravascular coagulation due to trauma or venous stasis may sometimes cause pain. For large lesions with significant thrombosis, distal embolization may subsequently occur. When malformations are extensive, a blood coagulation profile should be performed. These patients are particularly at risk for a pulmonary embolus following surgery; they require anti-thromboembolic prophylactic treatment [11]. Trauma, infection, and hormone changes of puberty and pregnancy can be associated with growth of the lesions, probably because the progesterone receptors that have been discovered in these malformations [12, 13].
Superficial venous malformations have a bluish compressible mass with no palpable thrill or audible bruit. These lesions often enlarge in a dependent position or with Valsalva maneuver. Phleboliths are commonly seen on radiographs. Doppler echocardiography, MRI or MRA, and direct-puncture phlebography may be required to confirm the diagnosis and assess the extent of the lesion.
Treatment
Treatment depends on the location and extent of the venous malformation. When a lesion is symptomatic, localized, and accessible, surgical excision remains one of the most superior treatment options and may offer a cure for localized lesions. Excision of complex lesions remains difficult due to intraoperative bleeding. Preoperative sclerotherapy (or sometimes multiple sessions of sclerotherapy) can be used prior to excision (24–48 h) to decrease surgical risk. Complete cure is not to be expected in patients with extensive disease but combined modality therapy may offer a long-term control of the disease. Superficial lesions or the superficial component of deep lesions can be treated with the Nd:YAG laser [14].
5.2.4.3 Arteriovenous Fistulae
Pathology
Arteriovenous fistulae or malformations (AVMs) are congenital vascular lesions associated with a variable degree of arteriovenous shunting. They are clinically evident in childhood or during puberty. Rapid expansion has been also reported following pregnancy and trauma, including inadequate surgical intervention. A defect in vascular stabilization is thought to cause AVM, but it remains unclear whether these lesions are primarily congenital in origin. An acquired AV fistula can also occur due to direct trauma to vessels; however, this is uncommon in the oral cavity.
Clinical Presentation
The presentation of AVMs is commonly by a warm swelling with a palpable thrill and an audible bruit. Oral lesions can present early due to gingival involvement, disruption of deciduous teeth, and profuse periodontal bleeding. Traditional angiography or MRA to demonstrate their vascular anatomy is essential for confirming the diagnosis and developing a treatment plan. Moreover, CTA allows evaluation of local effects on surrounding tissues and bones and can define individual arterial feeders as well [15].
Treatment
Treatment of AVMs could be problematic especially with large and diffuse lesions due to complete replacement of normal tissues by the diseased vessels. Such lesions require reconstruction after excision. Recurrence is also common after embolization or even after surgical excision due to recruitment of new vessels [16]. When a lesion is small and asymptomatic, a period of observation is often the most convenient initial strategy. Large and diffuse lesions are usually symptomatic and a delayed treatment may lead to cardiac decompensation. Intra–arterial embolization combined with surgical excision currently offers the best chance for cure. Excision is preformed 24–48 h after embolization. This helps control blood loss and defines the surgical margins of the lesion. Complete excision is sometimes impossible because of the location and extent of the malformation. Long-term follow-up with a dedicated multidisciplinary team is thus crucial for AVM management.
5.2.4.4 Lymphatic Malformations
Pathology
Lymphatic malformations, previously known as “cystic hygroma” or “lymphangioma,” are composed of dilated lymphatic vessels with inappropriate communication, lined by endothelial cells, and filled with lymphatic fluid. Their incidence is approximated to be 1 in 2000–4000 live births [17]. Lymphatic malformations are classically classified into macro-cystic, micro-cystic, or mixed according to the cyst size (2 cm3) [7]. What usually affect the oral cavity are the micro-cystic or mixed variants. These small non-compressible vesicles can weep and at times cause pain or minor bleeding. Micro-cystic disease usually carries a worse prognosis and could be more aggressive, invasive, and difficult to control [18].
Clinical Presentation
Symptoms are usually related to the extent of the disease, which can be defined by MRI. The patient usually suffers from pain, dysphagia, and odynophagia.
Treatment
As spontaneous resolution is usually not anticipated, management of symptomatic disease is usually mandatory. Treatment is usually easier and carries a more favorable prognosis with the macro-cystic type. Treatment modalities include sclerotherapy [19], carbon dioxide laser [20], and surgical excision (with/without reconstruction). Multiple combined treatment modalities are sometimes necessary for the disease control.
5.3 Ulcers of the Oral Cavity
5.3.1 Etiological Classification
The most common varieties of oral cavity ulcers are summarized in Table 5.2.
Table 5.2
List of the most common varieties of oral cavity ulcers
Traumatic ulcers | Inflammatory ulcers | Dyspeptic ulcers | Malignant ulcers |
|---|---|---|---|
Dental ulcers | Herpetic ulcers | Aphthous (metabolic or dyspeptic) ulcers | Epithelioma |
Frenular ulcers | Tuberculous ulcers | Lymphoepithelioma | |
Syphilitic ulcers | Adenocarcinoma | ||
Chronic superficial (nonspecific) glossitis | Basal cell carcinoma | ||
Malignant melanoma |
5.3.2 Traumatic Ulcers
5.3.2.1 Dental Ulcers
Dental ulcers are caused by trauma from a broken tooth or ill-fitting dentures. The ulcer occurs mostly at the side of the tongue. It is painful, with sloping serrated edges, elongated shallow floor covered with granulation tissue, and soft or mildly indurated base. It heals in few days when the cause is removed; otherwise it should be biopsied, particularly if malignancy is suspected. Treatment is by extraction of the ragged tooth plus good oral hygiene. Antibiotics are used if superadded infection occurs.
5.3.2.2 Frenular (Pertussis) Ulcer
A frenular ulcer results from trauma of the frenulum of the tongue by the teeth during coughing in children with whooping cough, between 6 and 8 months of age (due to eruption of lower teeth). Treatment of the cause results in healing of the ulcer.
5.3.3 Inflammatory Ulcers
5.3.3.1 Herpetic Ulcers
Herpetic ulcers are caused by herpes simplex (HS) virus in patients with low resistance (e.g., following pneumonia). They appear in the tongue and angles of the mouth as multiple, small, painful ulcers, preceded by vesicles.
5.3.3.2 Tuberculous (TB) Ulcers
Tuberculous ulcers result from active pulmonary TB or infected milk (causing ulcers, or diffuse fibrosis – woody tongue). They usually appear at the tip and sides of the tongue as multiple, painful, shallow ulcers with undermined edges, yellowish floor, and soft base. Treatment is by antituberculous drugs and sanitorial management.
5.3.3.3 Syphilitic Ulcers
During the first stage of syphilis, a chancre may occur at the tip of the tongue together with enlarged submental and submandibular LNs. During the second stage, mucous patches and snail track ulcers are present in the tongue (multiple and yellowish-white) associated with Hutchinson’s warts or condylomata. Gummatous ulcer develops during the third stage of syphilis, at the midline of the dorsum of the tongue. It is painless, single, with clear-cut edges and washleather floor. Leukoplakia of diffuse fibrosis may also be present.
5.3.3.4 Chronic Superficial Glossitis
Chronic superficial glossitis may be associated with chronic repeated nonspecific ulcers, usually on the dorsum of the tongue. Ulcers are superficial, small, and painful. They are associated with fissures or vesicles and have a unilateral distribution. Untreated chronic superficial glossitis may lead to leukoplakia, erythroplakia, or overt squamous cell carcinoma (SCC). Treatment includes avoiding the predisposing factors, mouth gargles, close follow-up, and biopsy of any developing lesions.
5.3.4 Dyspeptic (Aphthous) Ulcers
Dyspeptic or aphthous ulcers represent the commonest type of ulcers of the oral cavity. They occur in patients with dyspepsia and are characterized by their short history and the painful erosions at the tip (Fig. 5.1) and sides of the tongue and inner sides of lips (Fig. 5.2) and cheeks (Fig. 5.3). Ulcers are small, multiple, with whitish floor, hyperemic margins, sloping edge, and soft base. The regional LNs are not enlarged.



Fig. 5.1
Aphthous ulcer at the tip of the tongue
Fig. 5.2
Multiple aphthous ulcers at the inner side of the lower lip
Fig. 5.3
Aphthous ulcer at the inner aspect of the left cheek
5.3.5 Malignant Ulcers
Malignant ulcers of the oral cavity are most commonly SCCs (epitheliomas) but may be lymphoepithelioma (in the posterior 1/3 of the tongue), salivary adenocarcinoma (from minor salivary glands), or, rarely, basal cell carcinoma (BCC) or melanoma. The epitheliomatous ulcer usually affects the tongue (Fig. 5.4) and lips (Fig. 5.5). It is characterized by a raised nodular everted edge, necrotic floor that bleeds easily on touch, and a hard indurated base. The commonest site is the anterior two thirds of the tongue. Regional LNs are usually enlarged and hard and either mobile or fixed according to stage of the disease. There may be also infiltration of deeper tissues including the bone in neglected cases.
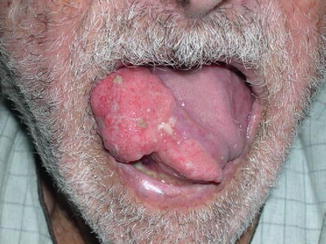

Fig. 5.4
A neglected epitheliomatous ulcer at the side of the anterior two thirds of the tongue in a 73-year-old gentleman. Note the large size and everted edge of the ulcer
Fig. 5.5
A neglected epitheliomatous ulcer at the side of the lower lip (reaching the corner of the mouth) in a 62-year-old gentleman. Note the large size, everted edge, and necrotic floor of the ulcer
For details, see under “Neoplastic Lesions of the Oral Cavity.” Differential diagnosis of tongue ulcers is summarized in Table 5.3.
Table 5.3
Differential diagnosis of ulcers of the tongue
Malignant ulcer | Dyspeptic (aphthous) | Frenular (pertussis) | Dental (traumatic) | TB | Syphilitic | |
|---|---|---|---|---|---|---|
Site | Side of the tongue | Dorsal and undersurface | Undersurface and frenulum | Side of the anterior two thirds | Tip or back of the tongue | Midline of dorsum |
Number | Single | Multiple | Single | Single | Single or multiple | Single |
Pain | ++ | +++ | + | ++ | + | − |
Teeth | Sepsis | ± | ± | Ragged | ± | |
Edges | Everted | Sloping | Sloping | Sloping | Undermined | Punched out |
Base | Indurated | Soft | Firm, granulation tissue | Soft | ± Fibrotic | |
Floor | Tumor | Whitish | Yellowish | Washleather | ||
Enlarged LNs | + | − | − | − | + | + |
5.4 Neoplastic Lesions of the Oral Cavity
5.4.1 Classification
Neoplastic lesions affecting the oral cavity are summarized according to their tissue of origin in Table 5.4.
Table 5.4
Classification of the tongue and floor of mouth neoplasms according to origin
Origin < div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|