Level
Area
Sublevels
Areas drained
I
Submental LNs
Submandibular LNs
IA
IB
Floor of mouth, anterior oral tongue, anterior mandibular alveolar ridge, and lower lip
Oral cavity, anterior nasal cavity, midface soft tissue structures, submandibular gland
II
Upper internal jugular nodes; lying between the skull base and the hyoid bone
IIA, IIB
Oral cavity, nasal cavity, nasopharynx, oropharynx, hypopharynx, larynx, and parotid gland
III
Middle internal jugular nodes; lying between the hyoid bone and cricoid cartilage
Oral cavity, nasopharynx, oropharynx, hypopharynx, and larynx
IV
Lower internal jugular nodes; extending between cricoid cartilage and the clavicle
The hypopharynx, cervical esophagus, and larynx
V
Posterior triangle (spinal accessory chain) LNs
VA
VB
VA: nasopharynx and oropharynx
VB: thyroid gland
VI
Pretracheal + prelaryngeal + paratracheal LNs
Thyroid gland, glottic and subglottic larynx, apex of piriform sinus, cervical esophagus
VII
Upper mediastinal LNs
Fig. 8.1
Regional nomenclature of cervical nodes
Fig. 8.2
Head and neck regions draining into each nodal level
8.1.1 Delineation of the Levels of Cervical Lymph Nodes [3] (Fig. 8.1)
Level IA: Submental Region
These LNs lie within the triangle bounded by the anterior belly of the digastric muscles (both sides) and the hyoid bone inferiorly.
Level IB: Submandibular Region
These LNs lie within the triangle bounded by the anterior and posterior bellies of digastric muscle inferiorly and the body of the mandible superiorly. It should be noted that the submandibular gland should be included in the removed specimen if the LNs within this level are excised.
Level IIA and IIB: Upper Jugular Group
Those are the LNs surrounding the upper third of the internal jugular vein (IJV). They extend from the skull base superiorly to the level of the inferior border of the hyoid bone inferiorly. Anteriorly, it is bounded by the lateral border of the sternohyoid muscle and the stylohyoid muscle. Posteriorly, it is bounded by the posterior border of the sternocleidomastoid (SCM) muscle. Level IIA LNs lie anterior to the vertical plane of the spinal accessory nerve, while IIB LNs lie posterior to this plane. Radiologically, level IB and level IIA LNs are separated by the vertical plane at the posterior aspect of the submandibular gland.
Level III: Middle Jugular Group
This level extends from the inferior border of the hyoid bone superiorly to the inferior border of the cricoid cartilage inferiorly and is located around the middle third of the IJV. Again, the anterior boundary is represented by the lateral border of sternohyoid muscle, and the posterior boundary is the posterior border of the SCM. The jugulo-omohyoid LN belongs to this group.
Level IV: Lower Jugular Group
These LNs extend from the lower border of the cricoid cartilage to the clavicle, and they are located around the lower third of the IJV. Anteriorly, this group is bounded by the lateral border of sternohyoid muscle and posteriorly bounded by the posterior border of SCM. It should be noted that the “Virchow” LN belongs to this group.
Levels VA and VB: Posterior Triangle Group
The upper limit of this group is the convergence of the trapezius and SCM muscles, while the lower boundary is formed by the clavicle. Anteriorly, it is bounded by the posterior border of SCM, and the posterior boundary is formed by the anterior border of the trapezius muscle. Level VA LNs and VB LNs are separated by an imaginary horizontal plane marking the lower border of the cricoid cartilage. Level VA LNs include the spinal accessory LNs, while VB includes LNs located around the transverse cervical vessels and the supraclavicular LNs.
Level VI: Central Compartment Group
This level includes pretracheal, paratracheal, pre-cricoid (Delphian), and peri-thyroidal LNs (including LNs located along the recurrent laryngeal nerves [RLN]). This region extends from the hyoid bone superiorly to the suprasternal notch inferiorly. Laterally, it is bounded by the common carotid arteries (CCAs).
8.1.2 Neck Dissection
8.1.2.1 Historical Overview
The term neck dissection refers to the removal of the fibrofatty tissue of the neck with the intention of treating lymphatic metastasis in the neck region. This surgical procedure was first described by George Crile in 1906 although reports of similar procedures of en bloc resections go back to 1888 when Franciszek Jawdynski – a Polish surgeon – reported four cases. The work of Crile was further popularized by several surgeons including the famous American surgeon, Hayes Martin. However, the morbidity accompanying the radical approach of the original procedure stimulated the development of a more conservative approach. Based on anatomical understanding of the lymphatic anatomy of the neck, Suarez introduced the principles of functional neck dissection in 1963. Later, Ettore Bocca published a description of an operative technique in the English literature aiming at the preservation of the non-lymphatic structures of the neck resulting in a better functional outcome and less morbidity, at the same time obtaining equivalent oncologic results [4, 5].
The ongoing experimentation and clinical studies resulted in a more precise understanding of the metastatic nodal patterns in head and neck malignancies [2, 6]. The resulting data allowed for a more conservative approach depending on the negligible risk of involvement of certain nodal regions in various oncologic scenarios ending in a wide range of surgical procedures. This variation called for an updated classification and nomenclature of operations involving surgical excision of the cervical lymphatics. In order to achieve this, AAO-HNS sponsored the work of the Committee of Head and Neck Surgery and Oncology to develop a unified classification of neck dissection operations. The first classification was established in 1991; this was later modified in 2002 and 2008 to become the currently accepted classification [7–11].
8.1.2.2 Classification of Neck Dissection (AAO-HNS and American Head and Neck Society) [3]
Radical Neck Dissection (RND)
This is the original standard operation of cervical lymphadenectomy to which all the other modifications have been applied. It entails removal of ipsilateral nodal groups extending from the lower border of the mandible superiorly to the clavicle inferiorly and from the lateral border of sternohyoid muscle, hyoid bone, and contralateral anterior belly of digastric muscle medially to the anterior border of trapezius muscle laterally. Thus, nodal groups of level I–V are removed, while the anterior compartment (central, level VI), suboccipital, peri-parotid (except for the infra-parotid LNs lying in the submandibular triangle), retropharyngeal, and buccinators LNs are not. It also includes the removal of spinal accessory nerve (SAN), IJV, and SCM.
Modified Radical Neck Dissection (MRND) (Figs. 8.3 and 8.4)
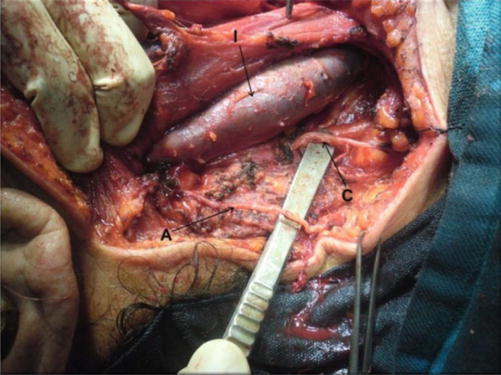
Fig. 8.3
Level V dissected, showing accessory nerve (A), branch from cervical plexus (C), and IJV (I)
Fig. 8.4
Levels III, IV and V dissected, showing accessory nerve (A), great auricular nerve (G), Erb’s point (E), IJV retracted (I), common carotid artery (C), vagus nerve (V), and trunks of brachial plexus (B)
This entails the removal of the same nodal groups as described in RND while preserving one or more of the non-lymphatic structures (SAN, IJV, and SCM). According to the current terminology, the preserved non-lymphatic structure should be named in the operation title, e.g., modified RND with preservation of IJV and SAN.
Selective Neck Dissection (SND)
This refers to the cervical lymphadenectomy with preservation of one or more nodal groups included in the original RND. This approach is based on the predictable patterns of nodal metastasis according to the site of the primary malignancy. As a result, different variations of lymphadenectomy have been described including:
Supraomohyoid neck dissection: removal of levels I–III.
Lateral neck dissection: removal of levels II–IV.
Posterolateral neck dissection: removal of levels II–V, suboccipital, postauricular, and the external jugular LNs.
Anterior neck dissection: removal of level VI LNs.
To obtain a unified terminology as regards to the variations in the extent of excision, it is recommended to mention the levels and sublevels excised following the term SND, e.g., SND [level VI].
Extended Radical Neck Dissection (ERND)
This entails removal of additional LN groups (including retropharyngeal, superior mediastinal, paratracheal, or buccinator LNs) or non-lymphatic structures or both, which are not included in the standard RND operation. Examples of non-lymphatic structures that can be removed include the vagus nerve, hypoglossal nerve, carotid artery, paraspinal muscles, or the overlying skin. The additional removed structures should be mentioned in the operation title.
8.2 Cervical Lymphadenopathy: Pathology and Clinical Pattern
8.2.1 Definition
Lymphadenopathy (LA) is a pathological process of LNs manifested by abnormally increased size or altered consistency or number [12]. Cervical lymphadenopathy (CLA) refers to cervical nodal tissue measuring more than 1 cm in diameter [13]. However, palpable supraclavicular nodes of any size are considered abnormal [14]. It is not a disease by itself; rather, it is a sign of an underlying pathology that ranges from a trivial infection to a metastatic malignant neoplasm.
8.2.2 Classification
8.2.2.1 Etiological
Cervical lymphadenopathy may be classified according to its etiology into malignant, infectious, autoimmune, miscellaneous, and iatrogenic (due to medications). These broad categories can be easily remembered using the mnemonic MIAMI [14].
8.2.2.2 Pathological
In General, CLA may be due to lymphoid hyperplasia or infiltration [15].
1.
Lymphoid hyperplasia is further subclassified, based on the anatomic and histopathology, into the following patterns: (1) follicular hyperplasia, (2) sinus hyperplasia, (3) paracortical hyperplasia, (4) necrotizing granulomatous lymphadenitis, (5) necrotizing non-granulomatous lymphadenitis, and (6) acute lymphadenitis [12].
2.
A lymph node may be infiltrated by malignant cells, in malignant lymphoma/leukemia, or by other cells, like lipid cells and glycogen-laden macrophages [15]. The former category includes a wide spectrum of lymphoid and hematopoietic neoplasms that are classified by the World Health organization (WHO) into (1) precursor B and T cell neoplasm, (2) mature B cell neoplasm, (3) mature T cell and NK cell neoplasm, (4) Hodgkin’s lymphoma, (5) histocytic and dendritic neoplasm, and (6) post-transplantation lymphoproliferative disorders ( LPDs) [16].
3.
An additional pathological entity is spindle cell lesions of LN which include (1) bacillary angiomatosis, (2) Kaposi sarcoma, (3) palisaded myofibroblastoma, and (4) inflammatory pseudotumor of LN [17].
8.2.2.3 Clinical
Based on distribution: CLA may be localized (only one area is involved), regional (two or more contagious areas are involved), or part of generalized (two or more noncontiguous areas are involved) [18].
Based on the duration: CLA is further classified into acute (2 weeks duration), subacute (2–6 weeks duration), and chronic (does not resolve by 6 weeks).
8.2.3 Etiology
A wide range of causes can result in CLA (Table 8.2). A recent cross-sectional study has demonstrated that the most likely cause of CLA depends on the age group; reactive or nonspecific inflammation was the most common cause in those younger than 14 years; tuberculous lymphadenopathy was the predominant pathology in 14–59-year group, while cancer should be suspected if the patient is 60 years or older [19].
Table 8.2
Causes of CLA
I. Infectious | II. Malignant | VI. Medications |
Viral Infectious mononucleosis Infectious hepatitis Herpes simplex Rubella Measles Adenovirus HIV Bacterial Streptococcus Staphylococcus Cat-scratch disease Tularemia Tuberculosis Syphilis leprosy Diphtheria Chlamydia Lymphogranuloma venereum Trachoma Rickettsial Scrub typhus Rickettsial pox Fungal Histoplasmosis Coccidiomycosis Parasitic Toxoplasmosis Leishmaniasis | Hodgkin’s lymphoma Non-Hodgkin’s lymphoma (NHL) Acute lymphoblastic leukemia Chronic lymphoblastic leukemia Hairy cell leukemia T cell lymphoma Multiple myeloma with amyloidosis Metastatic | Allopurinol Atenolol Captopril Carbamazepine Cephalosporin Gold Hydralazine Penicillin Phenytoin Primidone Pyrimethamine Quinidine |
III. Immunological disease | VII. Miscellaneous | |
Rheumatoid arthritis Systemic lupus erythematosus (SLE) Sjogren’s syndrome Drug hypersensitivity Silicone associated Serum diseases Graft versus host disease | Sarcoidosis Histiocytosis X Kikuchi’s disease Kawasaki’s disease Castleman’s disease Lymphomatoid granulomatosis | |
IV. Endocrine disease | ||
Hyperthyroidism Thyroiditis Adrenal insufficiency | ||
V. Lipid storage disorders | ||
Gaucher’s disease Niemann-Pick’s disease |
8.2.3.1 Infections
Cervical lymphadenopathy may occur when the draining nodes react to a nearby infection in the head and neck region including upper respiratory infection or when the infectious agent localizes in the node itself.
Acute bacterial infections are most commonly caused by Staphylococcus aureus or Streptococcus pyogenes and should be suspected in patients with pustular or vesicular lesions of the face or scalp, history of earache or discharge, and history of sore throat or cough suggesting skin, ear, or upper respiratory infections, respectively. Infection with anaerobes like bacteroides may be suspected in patients with dental abscess or periodontal disease. Pasteurella multocida infection may follow animal bites, while Yersinia pestis infection may follow flea bites [21]. Clinically, adenopathy is often solitary unilateral and usually involving submandibular, upper deep cervical, submental, and occipital area in decreasing order of frequency. Enlarged LNs are tender and may be fluctuant, and the overlying skin is warm and erythematous [15]. The patient is feverish and usually has an evident source of infection.
Acute viral adenitis typically follows an upper respiratory tract infection by rhinovirus, parainfluenza virus, influenza virus, respiratory syncytial virus, coronavirus, and adenovirus. Other less common etiologies are mumps, measles, rubella, varicella, and herpes simplex. Clinically, adenopathy is commonly multiple and bilateral. Lymph nodes are relatively small, typically not tender, and rarely suppurate, and the overlying skin is not warm nor erythematous. Patients usually have low-grade fever and commonly complaining of cough, rhinorrhea, conjunctivitis, or skin rash.
Infectious mononucleosis (IMN) is particularly common in children and adolescents and is caused by Epstein-Barr virus which spreads primarily by saliva and replicates inside B lymphocytes and epithelial cells of the pharynx. Diagnosis is based on Hoagland’s criteria: at least 50 % of lymphocytes and at least 10 % of atypical lymphocytes in the presence of fever, pharyngitis, and adenopathy. Cervical adenopathy usually involves the posterior group and may be associated with axillary adenopathy, inguinal adenopathy, or splenomegaly. Diagnosis should be confirmed serologically through the classic Paul-Bunnell test, which detect heterophil antibodies by agglutination of sheep red cells, or through the more sensitive detection of antibodies to viral capsid antigens [22].
Chronic infectious lymphadenopathy is defined by failure to resolve or improve despite 2–6 weeks of appropriate therapy. Important causes of chronic infectious lymphadenopathy are detailed in the following sections.
Tuberculosis (TB)
Tuberculosis (TB) is an ancient multisystem disease that has been detected in Egyptian mummies dating to 5000 BC. It continues to be one of the most prevalent communicable diseases particularly among third-world countries. The developed countries witness a health challenge caused by TB because of increasing migration from developing countries and rising incidence of HIV in these countries [23]. The causative organism is Mycobacterium tuberculosis, though it can also be caused by other mycobacteria. Though TB can virtually involve any body organ, the lymphatic system is the most common site of extrapulmonary affection, within which cervical LNs are the most commonly involved [24]. The portal of entry usually determines the affected nodal group; involvement of jugulodigastric LNs usually denotes infection entering through tonsils or adenoids, while a pulmonary source is usually manifested by supraclavicular lymphadenopathy [25]. Histopathologically, tuberculous LNs demonstrate epithelioid, macrophages and giant cells, caseation necrosis, and scanty acid fast bacilli appearing as fragmented or beaded rods inside or outside cells [26].
In a study of 102 patients presenting with neck mass (Fig. 8.5) of tuberculous etiology, fever was present in 64 % of patients, weight loss in 42 %, and sweating in 18 % [24]. Locally, Jones and Campbell classified tuberculous lymphadenopathy into five distinct stages (Table 8.3) [27].

Fig. 8.5
Matted tuberculous cervical lymph nodes in a 23-year-old young gentleman
Table 8.3
Stages of TB lymphadenopathy
Stage | Description | Pathogenesis | Clinical features |
|---|---|---|---|
1 | Discrete LNs | Nonspecific reactive hyperplasia; | Large, firm, and mobile LNs |
2 | Matted LNs | Periadenitis | Large and rubbery LNs, fixed to surrounding tissues |
3 | Cold abscess | Central softening and caseation deep to the deep fascia | Soft, smooth, nontender, fluctuant selling without involvement of the skin |
4 | Collar stud abscess | As a result of increased pressure caseous material perforates the deep fascia | Abscess is adherent to the overlying skin |
5 | Tuberculous sinus/ulcer | When the abscess bursts | Chronic nonhealing sinus or ulcer with thin, bluish, undermined edges and scanty watery discharge |
Syphilis
Syphilis is a sexually transmitted disease, caused by Treponema pallidum, which can invade mucous membranes not only of the genital region but also of the head and neck such as the lips, tongue, and tonsils. Clinically, chancre is usually present at primary site of infection; its absence, however, is reported in some cases in which diagnosis becomes more difficult. Enlarged LNs are multiple, firm, mobile, and not tender. Diagnosis is usually made serologically through rapid plasma reagin (RPR) test, T. pallidum hemagglutination assay (TPHA) test, and Venereal Disease Research Laboratory (VDRL) slide test [30, 31].
Cat-Scratch Disease
Cat-scratch disease is a zoonotic disease transmitted through cats, caused by Bartonella henselae. Diagnosis requires at least 2 of the following three criteria: (1) presence of typical clinical symptoms, (2) serological detection of antibodies against B. henselae, and (3) detection of Bartonella DNA in the extirpated lymph nodes. Clinical symptoms include fever, lymphadenopathy, asthenia, pharyngitis, laryngitis, and skin rash. Lymphadenopathy is the most common clinical manifestation with the cervical nodes being the most frequently involved [32].
Toxoplasmosis
Toxoplasmosis is a zoonotic disease transmitted through ingestion of undercooked meat containing oocytes of Toxoplasma gondii present in cat’s feces. Cervical lymphadenopathy is present in 90 % of cases and may be associated with fever, sore throat, and myalgias. The nodal enlargement is usually solitary, discrete, mobile, and nontender [33].
8.2.3.2 Malignancy
Although CLA is more commonly caused by a benign etiology, a sinister underlying malignant process is not uncommon, necessitating careful evaluation of such patients. Exclusion of malignancy is in fact the first and the single most important aim sought by the physician when evaluating CLA. The incidence of malignancy in patients with CLA seems to vary considerably with their demographics: age, gender, and race. The rate of malignant etiologies rises with age. A cross-sectional study by Biswas et al. [19] demonstrated that the rate of malignancy among patients with CLA was 12.1 %, 21.7 %, and 100 % in the age groups <14, 15–59, and ≥60 years, respectively. In their study, Shakya et al. [34] observed a malignancy rate as high as 50 % in patients with CLA in 51–60-year age group. Such high incidence of malignancy among the aforementioned age groups led to the belief that any neck mass in an adult should be suspected as malignant until proven otherwise [35]. Gender issue has also been studied with the uniform finding of higher frequency of malignancy among males [36]. Similarly, incidence of malignancy in patients with CLA differs among different racial groups. A malignancy rate as high as 50 % was observed among Iranians presenting with unknown neck masses [37], while it was 28.2 % and 4.8 % among Indians and Nepalese, respectively [19, 34].
Malignant cervical LNs may be caused by secondary metastasis from another primary or less commonly by lymphoma [19, 34]. However, in their audit of 140 patients with CLA, Magsi et al. [38] found that lymphoma was more common than metastasis. Among the latter group, Naeimi et al. [37] found that SCC was the most common pathology regardless of age with the larynx and hypopharynx being the most common sites of the primary tumor. Similar findings were reported by Biswas et al. [19] with adenocarcinoma coming second in frequency. Lymphoma, as a cause of malignant CLA, ranks the second in frequency with NHL being more common in some series [19], while others reported that Hodgkin’s lymphoma was more common [37].
Histologically, the presence of Reed-Stenberg cells (large cells with abundant basophilic cytoplasm and multiple nuclei) in a background of inflammatory cells is characteristic of Hodgkin’s disease (HD) (Fig. 8.6). The WHO classified HD into five subtypes according to the predominant cell types: (1) nodular sclerosis, (2) lymphocyte rich, (3) mixed cellularity, (4) lymphocyte depleted, and (5) nodular lymphocyte predominant [12]. In NHL, parafollicular or marginal zone distribution of B cells occurs in nodal marginal zone b cell lymphoma, while complete, partial, sinus, or interfollicular involvement with variable cytology occurs in diffuse large B cell lymphoma, not otherwise specified [17].
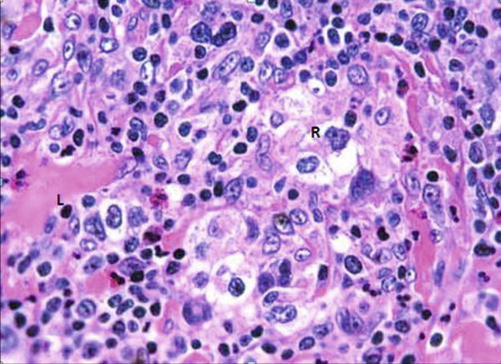
Fig. 8.6
H&E-stained section demonstrating classical pathology in Hodgkin’s lymphoma (L lymphocyte, R Reed-Sternberg cells)
Clinical features suggestive of malignant etiology of CLA include:
Generally: NHL usually presents with generalized lymphadenopathy with or without hepatosplenomegaly, in contrast to Hodgkin’s lymphoma in which the lymphadenopathy is initially localized and subsequently spreads orderly to contiguous nodal regions. Systemic manifestations like fever, weight loss, night sweats, and pruritus are called B symptoms and are suggestive of lymphoma: being less common in non-Hodgkin’s type [18].
Regionally: a pigmented skin lesion or mass that is mobile with deglutition may suggest metastatic deposits from nearby melanoma or papillary thyroid cancer [12].
Locally: enlarged supraclavicular LN carries the highest risk of malignancy and should always be viewed with suspicion [39, 40]. Hard, fixed, painless lymph nodes are highly suggestive of metastatic deposits (Fig. 8.7), while rubbery or firm mobile nodes are more suggestive of lymphoma, though amalgamation (Fig. 8.8) and limitation of mobility may occur later [14].

Fig. 8.7
Bilateral cervical lymphadenopathy, metastatic from unknown primary, in an old female patient

Fig. 8.8
Left-sided neck mass, turned out to be amalgamated LNs, in an old female with lymphoma
8.2.3.3 Autoimmune Disease
Lymphadenopathy is a detectable physical finding in up to 82 % and 69 % of rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) cases, respectively, but it could also be seen in almost any autoimmune disorder. In these disorders, adenopathy of cervical nodes ranks second in frequency after axillary lymphadenopathy [41]. Histopathologically, inflamed nodes show reactive follicular hyperplasia, polyclonal plasma cell infiltration with occasional mitosis in the interfollicular area, moderate vascular proliferation, and no compression of reticulin fibers; this is to differentiate it from lymphoma in which interfollicular area shows many mitosis, scarce plasma cells, and compressed reticulin fibers [42].
When present, cervical lymphadenopathy is usually associated with axillary and/or inguinal lymphadenopathy. Lymph nodes are usually multiple, relatively small, soft, mobile, and not tender [43]. Diagnosis should be made on the ground of relevant clinical and laboratory criteria. Polyarthritis of small joints, lasting more than 6 weeks together with elevation of serum rheumatoid factor (RF), anti-citrullinated protein antibody (ACPA), and acute phase reactants (APR) is diagnostic for RA [44]. Presence of malar rash, discoid rash, nonerosive arthritis, photosensitivity, oral ulcers, and renal, neurologic, and hematologic disorders and elevated antinuclear antibodies and anti-DNA antibodies are diagnostic of SLE [45]. Dryness of the mouth and eyes is suggestive of Sjogren’s syndrome [46].
8.2.3.4 Endocrine Disease
Sahlmann et al. [47] reported that cervical lymphadenopathy (levels II–IV, VI) occurred in more than 80 % of patients with autoimmune thyroiditis (AIT). Similarly, cervical lymphadenopathy was detected in 23 % of cases of Hashimoto’s thyroiditis (HT) [48]. Graves’ disease has also been reported to be associated with cervical lymphadenopathy [49, 50]. Pathology is reactive lymphoid hyperplasia. Therefore, AIT including HT should be included in differential diagnosis of patients with thyroid nodes and cervical LNs. Presence of cervical lymphadenopathy in a patient with clinical features of chronic adrenal insufficiency should alert the physician to the possibility of secondary adrenal involvement or to the very rare entity of primary adrenal lymphoma [51, 52].
8.2.3.5 Drug-Induced Lymphadenopathy
Certain medications can cause diffuse lymphadenopathy; of which phenytoin-induced lymphadenopathy is the most widely described in the literature. The reaction tends to occur few months after initiation of therapy and usually disappear within weeks after stopping drug administration. Pathophysiology is thought to be due to medication-induced immunologic disturbances, including reduced humoral and cellular immunity. Pathology usually reveals partial or complete effacement of the lymph node architecture by polymorphous infiltration of lymphocytes, plasma cells, and eosinophils [53, 54].
Phenytoin, in particular, has also been associated with a characteristic nodal pathology, termed pseudolymphoma. Differentiation from lymphoma is based on the absence of clonal proliferation of T cells. Clinically, cervical adenopathy tends to be bilateral and usually part of generalized lymphadenopathy. Condition is often associated with fever, rash, and eosinophilia. A high index of suspicion should always be kept since the condition can be easily confused with lymphoma. History of phenytoin exposure, improvement on phenytoin discontinuation, and pathological examination of a surgically excised lymph node are the clues to correct diagnosis [55].
8.2.3.6 Miscellaneous Causes of Cervical Lymphadenopathy
Kawasaki Disease (KD)
It is a type of systemic vasculitis of unknown etiology, also known as lymphocutaneous disease. It commonly occurs in children under 5 years of age. Cervical lymphadenopathy is present in approximately 42–65 % of KD patients [56]. Histopathologically, adenopathy is caused by sinus expansion and paracortical zone enlargement. Lymph nodes may also show ischemic changes in the form of necrotic foci, developing below the capsule and accompanied by fibrin thrombi in the surrounding small vessels [57]. Diagnosis should be clinically suspected in the presence of: (1) fever more than 5 days; (2) cervical lymphadenopathy, usually unilateral; (3) edema, erythema, and/or desquamation of the palms and soles; (4) non-purulent bilateral conjunctivitis; and (5) strawberry tongue. A high index of suspicion should be kept when evaluating these children as the condition may be complicated by coronary artery abnormalities (aneurysm, thrombosis, infarctions) in 25 % of untreated children. Helpful laboratory data are elevated white cell count with neutrophilia and lymphopenia; elevated acute phase reactant, C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR); and elevated liver enzyme, aspartate transaminase (AST) and alanine transaminase (ALT) [58].
Sarcoidosis
It is a multisystem chronic inflammatory condition of unknown etiology. Cervical lymphadenopathy is the most common head and neck manifestation of the condition, though it accounts only for 1.7 % of all head and neck lymphadenopathy. Histopathologically, it is characterized by the presence of noncaseating epithelioid cell granulomas (Fig. 8.9).
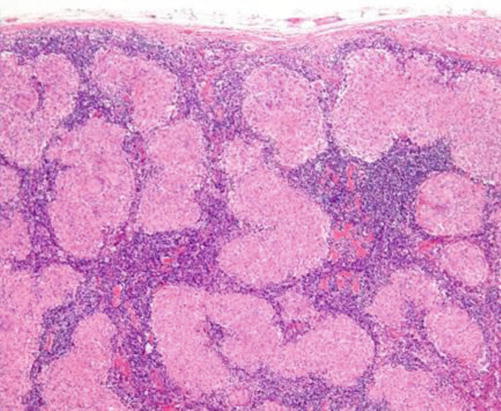
Fig. 8.9
H&E-stained section in an LN showing multiple sarcoid granulomas
Diagnosis is usually established on the basis of compatible clinical and radiologic findings of hilar lymphadenopathy, pulmonary infiltration, and skin and ocular lesions. However, a diagnostic challenge arises when isolated cervical lymphadenopathy is the sole clinical feature. The latter condition usually necessitates exclusion of other granulomatous disease particularly tuberculosis, histopathological examination of surgically excised lymph node, and immunohistochemical detection of high expression of tumor necrosis factor-α (TNF-α) in epithelioid cells [59, 60].
Histiocytosis X
It is a rare disease predominantly affecting children. A controversy exists regarding its etiology: reactive versus neoplastic. Nodal involvement may be an isolated lesion or more commonly a part of systemic disease [61]. The pathological hallmark is presence of clonal proliferation of antigen-presenting dendritic cells called Langerhans cells (LCs) (Fig. 8.10): so-called Langerhans cells histiocytosis [59].
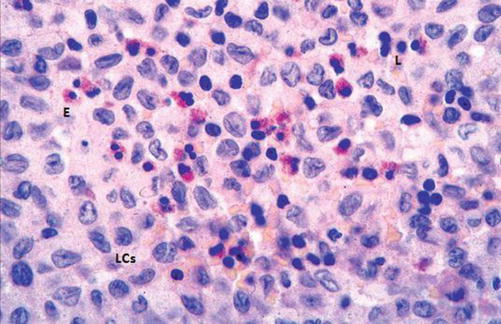
Fig. 8.10
H&E-stained section in a histiocytosis lymph node showing proliferation of Langerhans cell (LCs) and scattered eosinophils (E) and lymphocytes (L)
Clinically, the disease has a broad spectrum of severity. The mildest form is called eosinophilic granuloma and is characterized by solitary bone, skin, lung, or stomach lesions. The moderate form of the disease is called Hands-Schuller-Christian disease and is characterized by a triad of diabetes insipidus, exophthalmos, and lytic bone lesions. The most severe form is Letterer-Siwe disease and is a life-threatening multisystem disorder.
Diagnosis can be made from fine-needle aspiration cytology which demonstrates many LCs through its characteristic nuclear features, namely, nuclear grooves and pseudoinclusions, as well as immunohistochemical detection of positivity for S-100, peanut agglutinin (PNA), MHC class II, CD1a, and langerin (CD207) [61].
Kikuchi-Fujimoto Disease (KFD)
It is a benign and self-limited disease, mainly affecting young Japanese women. Etiology is unknown; however, an infectious cause has been proposed. Histopathologically, the LN shows single or multiple areas of necrosis and histiocytic cellular infiltrate (Fig. 8.11), so-called histiocytic necrotizing lymphadenitis. Clinically, patients usually present with localized lymphadenopathy, fever, and leucopenia. The disease may be associated with autoimmune phenomena and may occur in the setting of SLE [62].
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
