Uveitis is usually due to immune or infectious causes; however, certain systemic or local drugs may also precipitate intraocular inflammation. In general, the pathogenesis of drug-induced inflammation is not well understood. It is hypothesized that direct and/or indirect mechanisms are involved. Direct mechanisms are thought to play a role with topically or intracamerally instilled drugs and usually are observed soon after medication use. Indirect mechanisms result from immune complex deposition in uveal tissues, immune reactions to antigens liberated from antibiotic-induced death of a microorganism, or drug-induced alteration of melanin’s ability to scavenge free radicals. These mechanisms may result in intraocular inflammation weeks to months after initial use of the drug.
The most common medications implicated in drug-induced uveitis are discussed in the following pages.
RIFABUTIN
Rifabutin is prescribed for the treatment and prophylaxis of Mycobacterium avium complex (MAC) infection in HIV-positive patients. Symptoms of acute uveitis may present 2 weeks to more than 7 months following initiation of therapy. Uveitis has been reported to occur with rifabutin alone as well as in combination with other antimicrobial agents such as azithromycin, erythromycin, clarithromycin, ethambutol, and fluconazole. It has been reported with doses as low as 300 mg per day. It recurs with re-challenge and increases in severity with dose escalation.
Symptoms
 Unilateral or bilateral
Unilateral or bilateral
 Pain
Pain
 Redness
Redness
 Photophobia
Photophobia
 Blurred vision
Blurred vision
Signs
 Conjunctival injection
Conjunctival injection
 Keratic precipitates
Keratic precipitates
 Anterior chamber cell/flare with or without hypopyon
Anterior chamber cell/flare with or without hypopyon
 Vitreous cell
Vitreous cell
 Perivascular retinal infiltrates
Perivascular retinal infiltrates
Treatment
 Discontinue rifabutin.
Discontinue rifabutin.
 Treat inflammation with topical steroids and cycloplegic agents.
Treat inflammation with topical steroids and cycloplegic agents.
Prognosis
 In most cases, uveitis resolves within 1 to 2 months of discontinuation of rifabutin and administration of topical corticosteroids, with favorable outcomes (complete resolution of symptoms and normalization of vision in many cases).
In most cases, uveitis resolves within 1 to 2 months of discontinuation of rifabutin and administration of topical corticosteroids, with favorable outcomes (complete resolution of symptoms and normalization of vision in many cases).
REFERENCES
Jacobs DS, Piliero PJ, Kuperwaser MG, et al. Acute uveitis associated with rifabutin use in patients with human immunodeficiency virus infection. Am J Ophthalmol. 1994;118(6):716–722.
Moorthy RS, Valluri S, Jampol LM. Drug induced uveitis. Surv Ophthalmol. 1998;42(6):557–570.
CIDOFOVIR
Cidofovir has been used intravenously and intravitreally for the treatment of cytomegalovirus (CMV) retinitis. Anterior uveitis has been reported to occur in 26% to 59% of patients receiving IV cidofovir after a median of 4 to 11 doses. Hypotony and uveitis have also been reported following IV cidofovir in a patient with nonocular CMV infection (encephalitis) and an otherwise normal fundus exam, suggesting a direct effect of the drug on the ciliary body. Anterior uveitis also occurs with intravitreal cidofovir for treatment of CMV retinitis. One cases series reported anterior uveitis in 26% of patients after a single intravitreal cidofovir injection. Concomitant use of systemic probenecid decreased the frequency of inflammation. Because of its association with immune recovery uveitis, cidofovir should not be used if immune recovery is expected.
Signs and Symptoms
 Pain, redness, photophobia, tearing, and decreased vision
Pain, redness, photophobia, tearing, and decreased vision
 Unilateral or bilateral nongranulomatous anterior uveitis with or without keratic precipitates, posterior synechiae, hypopyon, and anterior vitreous cell
Unilateral or bilateral nongranulomatous anterior uveitis with or without keratic precipitates, posterior synechiae, hypopyon, and anterior vitreous cell
 The uveitis may be severe and fibrinous, and accompanied by hypotony.
The uveitis may be severe and fibrinous, and accompanied by hypotony.
Treatment and Prognosis
 Aggressive topical steroid and cycloplegic agents
Aggressive topical steroid and cycloplegic agents
 Cessation of cidofovir is usually required.
Cessation of cidofovir is usually required.
 Outcome is variable with potential for permanent structural complications such as posterior synechiae and hypotony.
Outcome is variable with potential for permanent structural complications such as posterior synechiae and hypotony.
REFERENCES
Ambati JK, Wynne KB, Angerame MC, et al. Anterior uveitis associated with intravenous cidofovir use in patients with cytomegalovirus retinitis. Br J Ophthalmol. 1999;83(10):1153–1158.
Kempen JH, Min YI, Freeman WR, et al. Studies of Ocular Complications of AIDS Research Group. Risk of immune recovery uveitis in patients with AIDS and cytomegalovirus retinitis. Ophthalmol. 2006;113(4):684–694.
Moorthy RS, Valluri S, Jampol LM. Drug induced uveitis. Surv Ophthalmol. 1998;42(6):557–570.
BISPHOSPHONATES
Bisphosphonates are used to inhibit bone resorption in patients with osteoporosis and to manage hypercalcemia associated with osteolytic bone cancer, metastatic disease to bone, and Paget’s disease of bone. Ocular inflammation has been reported most commonly with pamidronate disodium, but is also seen with other agents in this class including zoledronic acid, alendronate sodium, risedronate sodium, and etidronate disodium. Onset has been reported anywhere from 24 hours to weeks after initiation of therapy.
Symptoms
 Unilateral or bilateral
Unilateral or bilateral
 Redness
Redness
 Pain
Pain
 Photophobia
Photophobia
 Blurred vision
Blurred vision
Signs
 Conjunctivitis
Conjunctivitis
 Episcleritis
Episcleritis
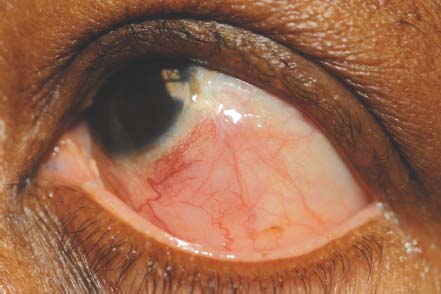
 Scleritis (Fig. 12-1)
Scleritis (Fig. 12-1)
 Iritis: Anterior chamber reaction with cell/flare
Iritis: Anterior chamber reaction with cell/flare
Treatment
 Nonspecific conjunctivitis seldom requires treatment; NSAID eye drops may provide symptomatic relief. In these cases, the bisphosphonates may be continued.
Nonspecific conjunctivitis seldom requires treatment; NSAID eye drops may provide symptomatic relief. In these cases, the bisphosphonates may be continued.
 Episcleritis may be treated with topical steroids or NSAIDS.
Episcleritis may be treated with topical steroids or NSAIDS.
 Anterior uveitis can vary markedly in severity, and may be treated with topical or systemic steroids depending on severity. In most instances, the bisphosphonate must be discontinued for the uveitis to resolve, and they must be discontinued for cases with scleritis.
Anterior uveitis can vary markedly in severity, and may be treated with topical or systemic steroids depending on severity. In most instances, the bisphosphonate must be discontinued for the uveitis to resolve, and they must be discontinued for cases with scleritis.
Prognosis
 Good, with resolution of symptoms in all cases, and resolution of scleritis with medical management and discontinuation of bisphosphonate therapy
Good, with resolution of symptoms in all cases, and resolution of scleritis with medical management and discontinuation of bisphosphonate therapy
REFERENCES
Fraunfelder FW, Fraunfelder FT, Jensvold B. Scleritis and other ocular side effects associated with pamidronate disodium. Am J Ophthal. 2003;135(2):219–222.
Moorthy RS, Valluri S, Jampol LM. Drug induced uveitis. Surv Ophthalmol. 1998;42(6):557–570.
Figure 12-1. Mild diffuse scleritis in a patient taking a bisphosphonate.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


