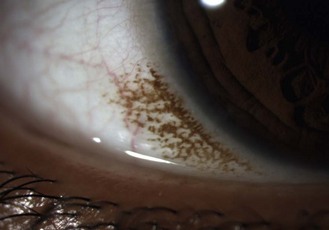
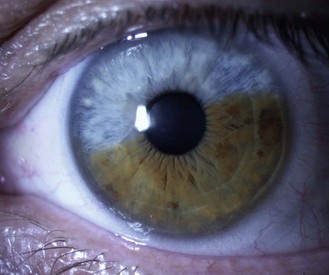
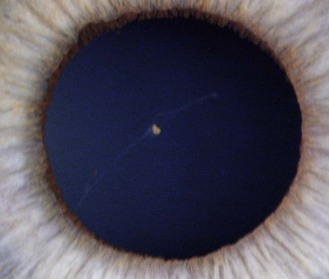
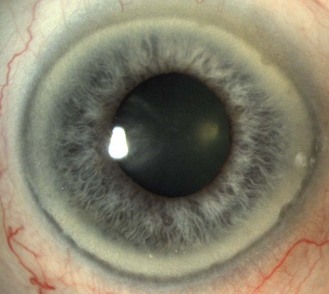
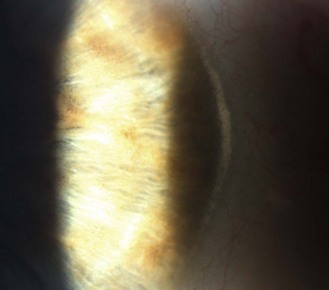
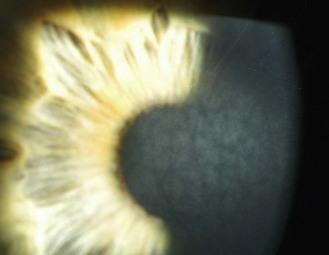
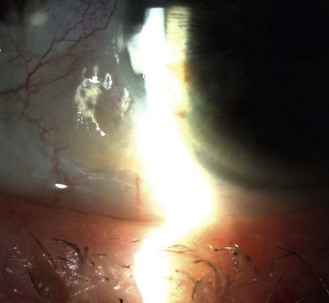
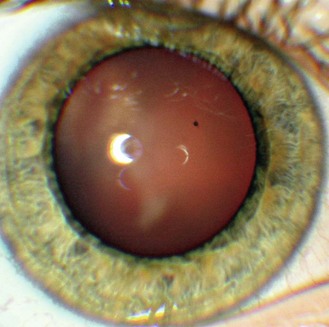
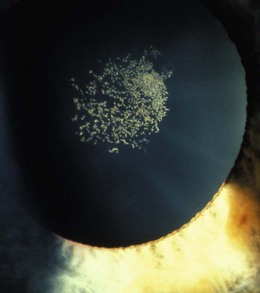
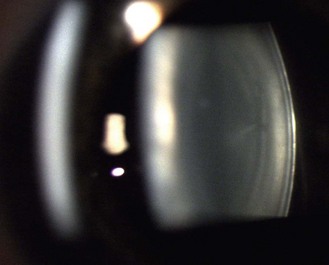
8 See online quiz 8.1 and additional online photographs 8.1i–8.5i. Concretions and pinguecula can be found in young adults, but are more common in older patients and are discussed in section 8.2. Relatively common, bilateral, benign, flat, pigmented areas of conjunctiva, typically near the limbus in young, heavily pigmented eyes (Figure 8.1 and online). The pigmentation is darkest at the limbus with decreasing intensity away from it. It is sometimes simply called complexion-associated conjunctival pigmentation to differentiate it from primary acquired melanosis, which are flat, speckled, brown lesions occurring in patients with European ancestry, do not diminish as they move away from the limbus and can rarely lead to conjunctival melanoma.1 Limbal epithelial folds that run radially. They are more easily seen in young heavily pigmented eyes and are most prominent in the lower limbus (Figure 8.2 and online). They house limbal epithelial stem cells, which produce epithelial cells to maintain the normal corneal epithelium or replace it in the event of injury.2 Little or no pigment gives ‘blue eyes’. With increasing amounts of pigment, the iris is seen as green, hazel or brown. People with blue irides have greater light scatter than those with more pigmented irides and may suffer more from disability glare in situations such as driving at night.3 Variations in pigment can produce wedge-shaped sections of hyper or hypo-pigmentation (heterochromia, Figure 8.3 and online) in one or both eyes. Hyperpigmented spots (naevi or ‘iris freckles’, Figure 8.4 and online) are common, but should be monitored using photography for changes due to the slight risk of malignant melanoma. These are strands of the embryonic pupillary membrane that remain into adulthood. One end of the strand inserts into the iris colarette and the other is either attached to the anterior lens capsule or floats in the anterior chamber (Figure 8.5 is a common example, while Figure 8.6 is rare; also online figures). Benign, bilateral drooping of upper lid tissue over the septum or lid margin with age (online figures 8.7i,ii). Cosmetic surgery is sometimes requested. Blepharoplasty or blepharoptosis repair can improve functional vision and may be recommended if the patient reports problems.4 The eyelid is either turned outward (ectropion) or inward (entropion) due to loose lids so that the inferior lid margin or puncta are not in contact with the eye. The patient may complain of epiphora or be symptomless. It is a common complaint, found in about 3% (ectropion, Figure 8.7) and 2% (entropion) of elderly patients.5 One of the most common benign eyelid tumours in the elderly.6,7 Hyperkeratinised, waxy, light grey-brown plaques found over the eyelids and face and appearing to be stuck onto the skin. Typically benign, but should be monitored for changes in size, shape, pigmentation, edge erosion, recurrent infection or inflammation and can be removed for cosmetic reasons. You should reassure the patient and monitor the lesion, ideally using photography.8 The most common benign lesion of the eyelid and often known as a ‘skin tag’.7 They are avascular, epithelial lesions of variable size, shape and colour (amelanotic to black) with a roughened surface reflecting the redundant epithelial cell growth (online figure 8.7iii). Over time, they grow and become attached to the eyelid surface by a stalk (pedunculated), so that the papilloma can be moved back and forth. You should reassure the patient and photograph the cyst, which can be removed for cosmetic reasons. Common, benign, yellowish, ‘cheesy’ cyst of variable size (typically 2–5 mm). Superficial cysts are covered by a thin layer of epithelial cells. Multiple small sebaceous cysts are often called milia. Subcutaneous or deep sebaceous cysts are larger (variable, but up to 20 mm) and slightly movable and covered by normal skin. They are caused by blockages to the sebaceous glands, with the blocked pore subsequently becoming filled with the oily sebum (Figure 8.8 and online). You should reassure the patient and photograph the cyst, which can be removed for cosmetic reasons. Bilateral, flat, light brown/yellow, triangular lipid masses with a nasal base, typically found on the inner upper eyelids of elderly patients and especially females (Figure 8.9 and online). They usually have a familial aetiology, but can be linked with atherosclerosis and high cholesterol and any initial diagnosis of xanthelasma should be referred for further investigation. They often reoccur if removed, so the patient should be warned of this if considering cosmetic removal.9 A commonly found, bilateral, 1.0–1.5 mm wide, greyish-white ring or part ring occurring in the periphery of corneas of older patients that is separated from the limbus by a thin ring of clear cornea, the lucid interval of Vogt (Figure 8.10 and online). It is called a corneal arcus rather than a corneal ring as it initially presents as arcs in the inferior and superior poles of the perilimbal cornea before spreading to form a complete ring. The inner edge is typically more diffuse than the sharper outer edge. Its prevalence increases significantly with age after 50 years.10 It is caused by lipid being deposited in the corneal stroma, having permeated from the limbal blood vessels, which become more permeable with age. Corneal arcus may be a sign of systemic hyperlipidaemias if seen in younger adults and any patient with arcus who is below the age of 50 years should be referred for further investigation. Typically asymptomatic, small (1–3 mm), yellow-white calcium lesions found in the palpebral conjunctiva of the upper and lower eyelid.11 They can be found in young adults, but are more common in elderly patients. The majority are superficial, hard and single (Figure 8.11 and online).11 A small percentage of concretions can cause symptoms, likely due to corneal irritation. Common, bilateral degenerative condition producing a narrow band of white, crystal-like opacities along the nasal or temporal limbus, typically found in older female eyes (Figure 8.12 and online). Two types are described: type I has a perilimbal clear zone similar to corneal arcus and contains numerous holes, while type II has neither holes nor a clear zone. Common, corneal orangey-brown iron deposition line found close to where the lid margins meet when blinking. The line is generally horizontal, possibly with a slight V-shape in the middle. It can be continuous or segmented and although some texts suggest that the prevalence typically matches the age of the patient, many Hudson-Stähli lines are faint and difficult to see under white light so that this high prevalence seems unlikely. However, they become more visible in cobalt blue (Figure 8.13 and online) or ultra-violet light.12 For this reason you may first notice it during a slit-lamp examination using fluorescein and cobalt blue illumination. Its aetiology is unclear, with the iron possibly arising from the tears, perilimbal blood supply and/or caused by UV radiation and the line/vortex pattern being linked with the position of eyelid closure or the growth and repair patterns of the corneal epithelium.12 Corneal iron deposition can occur in orthokeratology patients and the iron deposition pattern and position appears to change after refractive surgery.13,14 This is a polygonal pattern of white or grey opacity in the cornea that is visible on direct illumination (Figure 8.14). It takes its name from the pattern of roughly tanned hides that follow the papillae of animals’ skin. Peripheral crocodile shagreen is the most common with a reported clinical incidence of 13.4%.15 The pattern is probably related to the arrangement of corneal fibrils allowing opacities to preferentially occur in some locations. Peripheral shagreen tends to progress towards but never reaching the central cornea. It can vary from faint to striking, and while the latter may be of concern, vision seems unaffected. No treatment is required, and referral is not appropriate. These are small excrescences of abnormal basement membrane and collagen fibrillar material from distressed corneal endothelium. They occur in the periphery of all corneas where they are termed Hassall-Henle bodies or ‘warts’ and the prevalence of frank central corneal guttata in those aged over 55 is about 9%, with smoking doubling their likelihood.16 Guttata are often accompanied by a fine pigment dusting, and the endothelial layer is said to take on a beaten metal appearance when viewed with specular reflection or retro-illumination (Figure 8.15). Identification of central corneal guttata may be important in patients undergoing refractive surgery, as mild corneal guttata has been associated with increased risk of complications post surgery.17 The transition from a simple observation of corneal guttata to a diagnosis of Fuchs’ endothelial dystrophy occurs when the guttata are accompanied by corneal thickening as evidenced by signs of oedema: striae, folds or clouding. Corneal guttata are a benign clinical finding, as is early Fuchs’ endothelial dystrophy. A degenerative thickening of the bulbar conjunctiva adjacent to the limbus and often found nasally (Figure 8.16 and online). Although it is seen in adult patients who work outdoors and do not wear sunglasses, its prevalence increases with age and it is very common in the elderly.18 Pingueculae can lift the lids away from the surrounding conjunctiva, leading to a local area of drying and hyperaemia for which artificial tears can be helpful. Given their minimal impact on the patient, and a likelihood to recur, surgical excision is rarely considered. Pinguecula can increase in size with age, so the mainstay of treatment is preventative with UV blockers in spectacles and/or sunglasses. Vitreous floaters can be found in young adults, particularly the large eyes of moderate to high myopes, but are more common in older patients and are discussed in section 8.4. Seen as a small black dot in fundal retro-illumination (Figure 8.17 and online) and a white dot on the posterior capsular surface in direct illumination. It is usually displaced nasally or inferior-nasally and it is a remnant of the attachment of the hyaloid canal to the posterior lens surface. The hyaloid artery provides nutrients to the developing lens in the growing foetus and is typically fully regressed before birth ( Small, light brown or tan star shaped deposits on the anterior lens surface (Figure 8.18 and online) that are remnants of the tunica vasculosa lentis (section 8.3.1). They can be bilateral or unilateral and single or multiple. The slit-lamp appearance of the normal adult lens shows a series of zones of clear media in both the anterior and posterior lens cortex delineated by a curved line of scattered light (Figure 8.19 and online). These zones are made up of lens fibre layers with different scattering properties, likely due to different refractive indices in the continually growing lens cortex. Koretz and colleagues suggested that an adult lens typically contains three zones that originate from lens growth at approximate ages of 5, 10 and 20 years, with a fourth zone often appearing after the age of 40.19 The lens is formed by the meeting of fibres that arch over the lens equator and join with other fibres to form branching suture lines which take on an upright ‘Y’ appearance anteriorly and an inverted ‘Y’ appearance posteriorly (Figure 8.19
Variations in appearance of the normal eye
8.1 Anterior eye variations
8.1.2 Congenital conjunctival melanosis
8.1.4 Palisades of Vogt
8.1.5 Pigment changes in the iris
8.1.6 Persistent pupillary membrane
8.2 Anterior eye changes in older patients
8.2.1 Dermatochalasis
8.2.2 Ectropion and entropion
8.2.3 Seborrheic keratosis
8.2.4 Papilloma
8.2.5 Sebaceous cysts
8.2.6 Xanthelasma
8.2.7 Corneal arcus (previously arcus senilis)
8.2.8 Concretions
8.2.9 Limbal girdle of Vogt
8.2.10 Hudson-Stähli line
8.2.11 Crocodile shagreen
8.2.12 Corneal guttata
8.2.13 Pinguecula
8.3 Lens and vitreous variations
8.3.1 Mittendorf dot
 but see video 8.1 which shows a full hyaloid artery in a young adult). It runs from the ophthalmic artery at the optic disc to the crystalline lens where it spreads over both surfaces of the lens in a capillary net or tunica vasculosa lentis.
but see video 8.1 which shows a full hyaloid artery in a young adult). It runs from the ophthalmic artery at the optic disc to the crystalline lens where it spreads over both surfaces of the lens in a capillary net or tunica vasculosa lentis.
8.3.2 Epicapsular stars
8.3.3 Zones of discontinuity
8.3.4 Y-sutures
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Variations in appearance of the normal eye