FIGURE 8.1 Endoscopic view of the anatomic features of the sphenoid sinus. The clival recess is bounded by the carotid arteries laterally and sella superiorly. The relationship of the internal carotid artery (ICA) and optic nerve (ON) is often accentuated by a well-pneumatized anterior clinoid (opticocarotid recess [OCR]). The petrous apex may be approached medially (direct access or lateral displacement of ICA) or inferior to the petrous ICA (arrows).
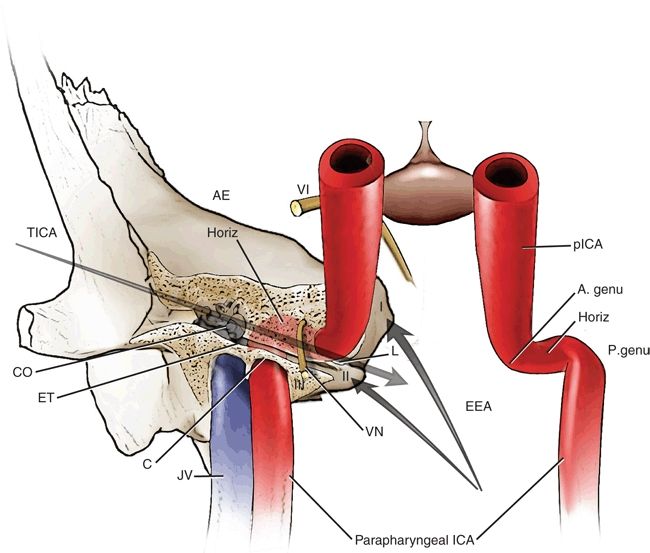
FIGURE 8.2 Schematic 3D figure to provide subjective comparison between both approaches (EEA and TICA) to petrous apex. Frontal view simulating the endoscopic endonasal approach in the operation room. Note the limits of each zone of petrous apex and the structures surrounding it, as well as the main direction provided by each approach. I, zone I of petrous apex; II, zone II; III, zone III; VI, abducens nerve; AE, arcuate eminence; CO, cochlea; JV, jugular vein, ET, eustachian tube; C, carotid canal; L, lacerum; VN, vidian nerve; P. genu, posterior genu petrous ICA; Horiz., horizontal petrous ICA; pICA, paraclival ICA; A. genu, anterior genu petrous ICA; ICA, internal carotid artery; EEA, endoscopic endonasal approach; TICA, transcanal infracochlear approach.
CONTRAINDICATIONS
Relative contraindications to an endoscopic endonasal approach include the usual patient comorbidities precluding surgery and difficult patient anatomy. If the patient has serviceable hearing, a transsphenoidal or traditional hearing sparing otologic approach should be considered (e.g., infralabyrinthine, transcanal infracochlear, or middle fossa approach). If the patient has minimal serviceable hearing and/or vestibular loss or if the direct endoscopic approach is technically difficult, then a transtemporal approach should be considered. For transtemporal operations, the temporal bone should be sufficiently pneumatized to navigate around or through the labyrinth. The middle fossa approach is technically demanding, there is no permanent drainage option, and some degree of brain retraction is required with the potential for injury to the brain. The transsphenoidal approach is better suited if continuous drainage is desirable (e.g., cholesterol granuloma).
PREOPERATIVE PLANNING
The success of any endoscopic skull base procedure depends on a thorough history, preoperative evaluation, and an informed consent conversation with the patient about the risks, benefits, and alternatives of various forms of treatment. Patients must understand the goals of surgery, which may only be diagnosis (biopsy) and the likelihood of achieving relief from symptoms. The surgical team needs to be prepared for the unexpected and have a well-developed plan in place for life-threatening complications including injury to the carotid artery.
CT and MRI are commonly used to assess petrous apex lesions. Cholesterol granuloma will typically appear on CT as an expansile lesion of the petrous apex with bony erosion and scalloping (Fig. 8.3A). Thinning of the posterior wall of the sphenoid and petrous carotid artery dehiscence may also be seen. Cholesterol granulomas have a characteristic appearance on MRI that is hyperintense on both T1-weighted and T2-weighted sequences, owing to the lipid and fluid content of these lesions (Fig. 8.3B and C). In contrast, a petrous apex cholesteatoma on MR will show a smooth, expansile mass with low signal intensity on T1-weighted imaging and high signal on T2-weighted imaging. A variety of MR pulse sequences have been described to help differentiate various petrous apex pathologies (e.g., graded recall echo).
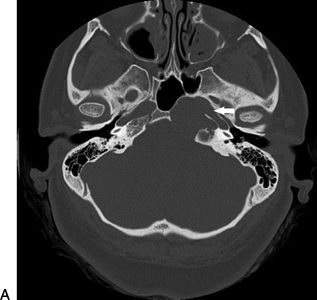
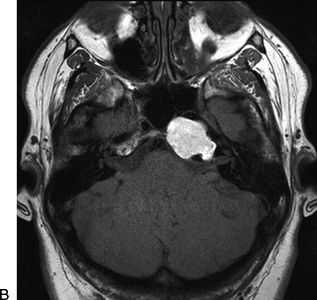
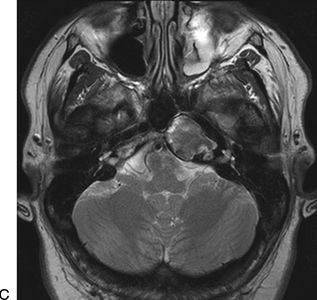
FIGURE 8.3 Axial imaging with CT and MR at similar locations of a patient with a left petrous apex lesion (biopsy proven to be a cholesterol granuloma). A. Axial CT showing an expansile lesion “bulging” into the medial sphenoid sinus. The arrow points to the left carotid canal with a dehiscent medial bony wall. B. An axial T1-weighted MR of the same patient showing a bright signal. C. An axial T2-weighted MR of the same patient showing an intermediate signal.
It is important to study the CT and MR to define the anatomy including the location of the carotid artery, optic nerve, jugular bulb, and facial nerve as well as the pneumatization of the sphenoid sinus and temporal bone (Fig. 8.4). The position and degree of bone covering/thinning of the petrous and clival portions of the carotid artery are very important. It is critical to ensure that the petrous apex pathology is not a vascular lesion such as a thrombosed aneurysm before any biopsy or drainage procedure is considered. The degree to which the pathology will be visible medial to the ICA after bone removal can be estimated on axial images by drawing a line from the pyriform aperture to the cyst (Fig. 8.4). The medial boundary is the medial edge of the pathology, and the most lateral boundary is the lacerum segment of the ICA, which cannot be retracted laterally.
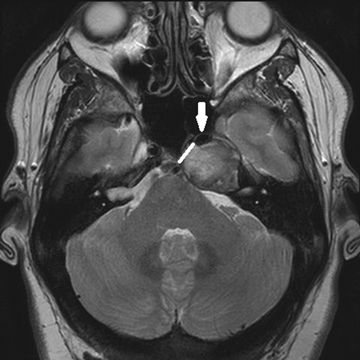
FIGURE 8.4 Axial MR showing a left petrous apex lesion pushing the carotid artery anteriorly (arrow). The artery must be identified intraoperatively and avoided during a transsphenoidal approach for management. The position of the artery narrows the corridor to access the lesion posteromedially (line).
SURGICAL TECHNIQUE (VIDEO 8.1)
The patient is placed supine on the operating room table with the head in a neutral position. The nasal mucosa is topically decongested with 1:1,000 epinephrine-soaked Neuro Patties. The image guidance system is appropriately set up, calibrated, and used to confirm important anatomy during the operation. A 0-degree 4-mm rigid nasal telescope attached to a high-definition video system is used for the majority of the operation. Angled telescopes (e.g., 30 degrees to 70 degrees) are often used to look into marsupialized cysts (e.g., cholesterol granuloma) once they have been opened.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


