SURGICAL TECHNIQUE
The patient is secured in a supine position with the head turned contralateral to the tumor. Three-point pin fixation is used, and the lateral skull, face, neck, and ipsilateral abdomen are included in the sterilized field. Intraoperative electromyographic monitoring of the facial nerve and any preoperatively intact lower cranial nerves can be performed. Somatosensory monitoring of the brachial plexus is also used in selected cases according to patient body habitus or cervical spine immobility. General endotracheal anesthesia is maintained without paralytic agents.
A post-auricular reverse S-shaped incision begins in the supra-auricular temporal scalp and extends behind the ear and into a cervical skin crease at least two-finger widths below the mandible (Fig. 33.1). The entire auriculoparotid flap is elevated from posterior to anterior with preservation of the temporalis fascia above and the platysma muscle below. The cartilaginous external auditory meatus is transected and oversewn with a two-layer, blind sac closure technique. An anterior to posterior incision is made below the temporal line to allow superior reflection of a temporoparietal flap and posteroinferior elevation of the sternocleidomastoid muscle and surrounding periosteum.
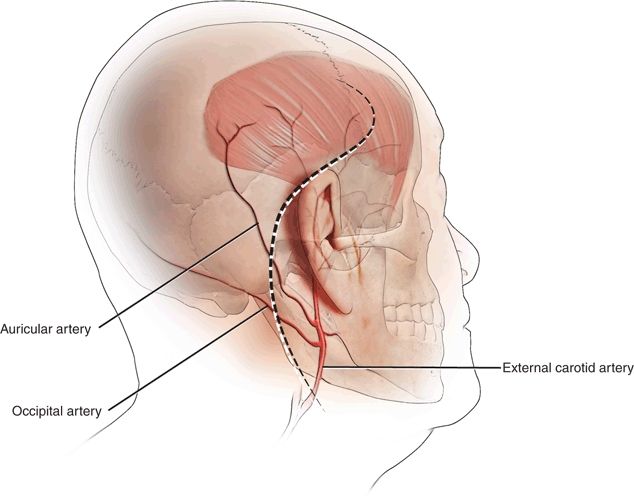
Figure 33.1 The retroauricular, reverse S-shaped incision utilized in the postauricular infratemporal fossa approach to the skull base.
The skin of the external auditory canal is removed including the tympanic membrane, the malleus, and the incus.
Subtotal Petrosectomy
A canal wall-up mastoidectomy is performed with early identification of the sigmoid sinus and the temporal dura. At least 3 cm of bone is removed posterior and inferior to the sigmoid sinus to allow preresection ligation of the vessel. The mastoid antrum is identified along with the lateral semicircular canal in order to safely open the facial recess. The bony canal wall can be removed with a rongeur or by drill curettage. The entire mastoid tip is removed with a rongeur, up to the level of the digastric groove and the stylomastoid foramen.
Under microscopic guidance, the facial nerve is skeletonized from the geniculate ganglion to the stylomastoid foramen. This facial bridge is left intact if tumor can be resected by dissecting both anterior and posterior to the nerve. Anterior transposition requires complete bone removal along the course of the nerve as well as transection of the greater superficial petrosal nerve. Retrofacial bone removal below the posterior semicircular canal and above the jugular bulb provides access to the posterior pole of the tumor (Fig. 33.2).
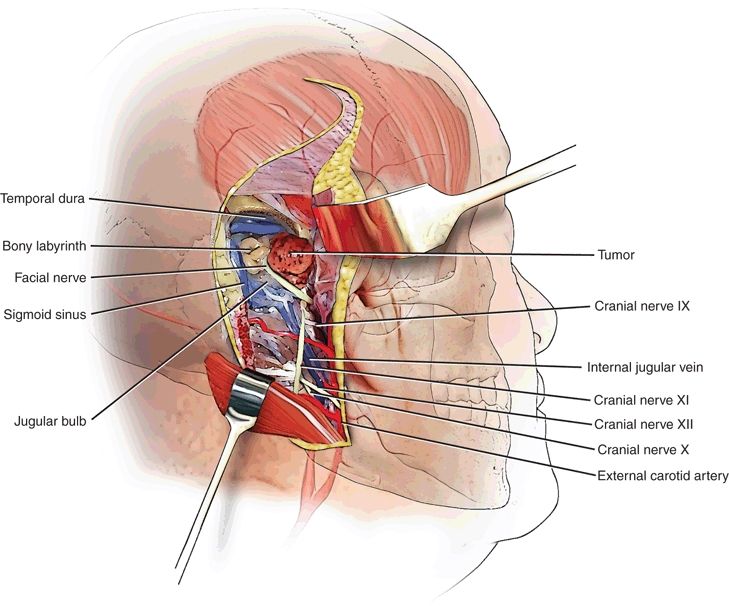
Figure 33.2 A subtotal petrosectomy approach with the “facial bridge” technique allows access to jugular foramen tumors without facial nerve transposition.
A labyrinthectomy can be performed to enhance posterosuperior exposure in patients with significant preoperative sensorineural hearing loss. Removing the anterior bony ear canal allows exposure of the temporomandibular joint and anterior retraction of the surrounding soft tissue. Anteromedial bone removal from the glenoid fossa and the styloid base provides exposure of the vertical segment of the petrous carotid canal and the eustachian tube orifice.
Neck Dissection
Following posterior sternocleidomastoid muscle reflection, the spinal accessory nerve and the IJV are identified. The IJV is circumferentially dissected, and cranial nerves IX, X, and XII are visualized. Anteromedial reflection of the digastric muscle allows superior dissection of the internal carotid artery. Vessel loops are placed around the great vessels. The facial nerve is viewed at the stylomastoid foramen, and a superficial parotidectomy is performed. If neural translocation is planned, peripheral branch dissection will reduce neural stretching and possible postoperative facial weakness.
Tumor Resection
The middle ear component of the tumor is coagulated with bipolar cautery and resected in piecemeal fashion until the bone of the promontory, the carotid canal, and the ampullated end of the superior semicircular canal are encountered. The posterior and posteroinferior margins are likewise managed, and the tumor is reduced to a relatively devascularized remnant in the jugular foramen.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


