
FIGURE 3.1 A. Drawing of binostril endoscopic approach to sella with endoscope in right nostril and additional instruments in each nostril. The inset drawing shows convergence of suction and ring curette in lower sella for adenoma removal as viewed by 0-degree endoscope placed in sphenoid sinus (A, adenoma; P, compressed pituitary gland; D, dura). B. Intraoperative photograph of hand positions and endoscope with otolaryngologist holding endoscope and irrigation while neurosurgeon has suction in left hand (in right nostril) and ring curette in right hand (in left nostril). (Image copyright Daniel Kelly Brain Tumor Center 2012.)
Instrumentation
Endoscopic equipment includes 4-mm rigid endoscopes (18 cm in length) with 0-, 30-, and 45-degree angled lenses and high-definition (HD) camera and two flat panel monitors (Karl Storz, Tuttlingen, Germany). Given the narrow working space afforded by the binostril endoscopic approach, all instruments should be as thin and low profile as possible. They may be straight or bayoneted depending upon the surgeon’s preference. After many years of performing endonasal microscopic pituitary surgery, We prefer bayoneted microinstruments. Microdissectors, ring curettes, and microblades are on bayoneted handles. Similarly, microscissors, tumor grasping forceps (both straight and up angled), and the bipolar cautery are used in a single-shaft pistol-grip design to minimize visual obstruction. High-speed drills, microdebriders, and ultrasonic aspirators also are of the lowest possible diameter with angled handpieces. Straight and curved variable suctions should also be available. A micro-Doppler (Koven, Inc. or Mizuho, Inc.) probe is also used for all cases to localize the cavernous carotid arteries prior to opening the dura. Warm (99°F/37°C) sterile saline is used for irrigation both to clean the tip of the scope and to promote local hemostasis. A 50-cc syringe with a curved irrigation tip is used to deliver the irrigation into the operating field when necessary.
Preoperative Medications
Preoperative antibiotics (typically cefazolin) are given and continued for 24 hours. In patients with normal preoperative adrenal function or those with Cushing’s disease, no perioperative glucocorticoids are administered. Those with adrenal insufficiency or borderline adrenal function are given 100 mg of hydrocortisone intravenously.
Positioning, Room Setup, and Prep
Following induction of general anesthesia with the patient in the supine position, the endotracheal tube emerges from the left corner of the mouth, and the anesthesiologists and anesthesia equipment are positioned on the patient’s left side. For patients with Cushing’s disease, acromegaly, other significant medical co-morbidities, or a large and vascular tumor, an arterial line and Foley catheter are placed; for other patients with microadenomas, small macroadenomas and typical RCCs, an arterial line and Foley catheter are not used.
An ergonomically efficient operating room setup is essential to ensure comfort of both surgeons especially during lengthy procedures. Two video monitors are positioned at almost 90-degree angles to each other: one above the patients’ head and one to the left of the chest; the neuronavigation monitor is placed in between the two video monitors. Our current operating room configuration is depicted in Figure 3.2. The patient’s head is placed in a horseshoe head holder and angled approximately 30 degrees toward the left shoulder. This arrangement allows both surgeons to stand comfortably on the patient’s right side, one at the head and one immediately below the head, and able to comfortably view their respective video monitors. The head is inclined in a neutral plane (0 degree) relative to the floor for sellar lesions; for suprasellar lesions, 10 to 15 degrees of neck extension is used, and for infrasellar and clival lesions, 10 to 15 degrees of neck flexion is used. The surgical navigation mask (Stryker Navigation) is placed on the face, and the system is registered to the preoperative MRI and/or CT angiogram. Only in prolonged cases is the head pinned in 3-point fixation, for example, with a craniopharyngioma or tuberculum sella meningioma in which the operative time may exceed 6 hours and there is risk of pressure necrosis with the horseshoe head holder.
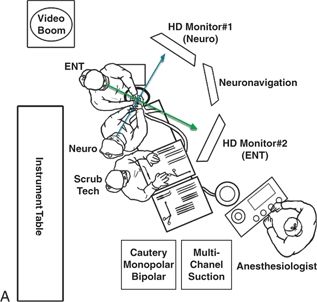

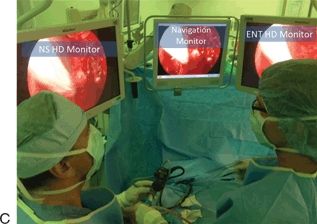
FIGURE 3.2 A. Diagram of operating room setup for endoscopic endonasal surgery for two surgeons with two HD video monitors, neuronavigation monitor, and ancillary equipment. (Image copyright Daniel Kelly Brain Tumor Center 2012.) B. Photograph of operating room setup showing HD monitors, neuronavigation monitor, and patient positioning prior to final draping. C. Intraoperative photograph of two surgeons looking toward their respective monitors.
The nasal cavity is prepped with decongestant (oxymetazoline 0.05%)-soaked Cottonoids placed in both nares for several minutes. The face, perinasal area, and right lower abdominal area (for a possible adipose tissue graft) are sterilely prepped and draped. A clear drape is used to allow visualization of the navigation mask during surgery. If the patient is fixed in pins and the tracking unit for navigation is attached to the Mayfield, a clear drape is not needed. Xylocaine 1% with 1:100,000 epinephrine is injected into the inferior and middle turbinates and lateral nasal walls bilaterally.
Approach to the Sphenoid Sinus
The initial approach through the nasal cavity uses a 0-degree 4-mm rigid endoscope and includes handling of the turbinates, raising of bilateral nasoseptal (NS) mucosa-preserving rescue flaps, wide sphenoidotomy, posterior septectomy, and posterior ethmoidectomies. As described below, we rarely use a vascularized nasoseptal flap in the skull base reconstruction and CSF leak repair for pituitary adenomas and RCCs and instead use a NS flap only in larger extended transplanum or transclival approaches. Using a Cottle elevator, the inferior and middle turbinates are out-fractured bilaterally, and the sphenoid ostia are identified. The middle turbinates are not routinely resected. We reserve the resection of the middle turbinate for lateral skull base pathologies such as Meckel’s cave and pterygopalatine fossa lesions. It has been suggested that postoperative debridements are more difficult if the middle turbinate is not resected, but this has not been our experience. Bilateral NS “rescue flaps” based on the posterior nasal artery are created (Fig. 3.3). An extended shaft, manually bent, microtip Bovie (Megadyne E-Z Clean 6.0″/152 mm ref: 0016M, Draper, Utah) is used to incise the mucoperiosteum inferior to the sphenoid ostium preserving the posterior septal artery pedicle, which comprises two arterial branches in 80% of cases and is located 8 to 9 mm below the ostium. The incision is then extended anteriorly using the inferior aspect of the superior turbinate as a horizontal guide to preserve the septal olfactory strip (SOS mucosal flap) for approximately 2 cm along the vomer and posterior nasal septum. This maneuver is performed bilaterally. These bilateral mucoperiosteal “rescue flaps” are then pushed inferiorly toward the nasopharynx with Cottonoids to minimize obstruction and provide access into the sphenoid sinus (Fig. 3.4). The SOS mucosal flaps are pushed laterally and superiorly onto the superior turbinate where they usually become adherent and out of the surgical field. These mucosa-preserving flaps obviate the need to transect the sphenopalatine artery, thereby greatly reducing the potential for postoperative sphenopalatine hemorrhage and epistaxis. With the majority of the endonasal mucosa preserved and out of the surgical field, any remaining superior mucosa may be excised with the microdebrider but removal of this mucosa is infrequently needed. The sphenoid keel, vomer, and posterior nasal septum are demucosalized and in view. A wide sphenoidotomy is then performed with up and down biting Kerrison rongeurs or the drill. This bone removal can be done from ostia to ostia superiorly and inferiorly to preserve a large piece of keel that can be harvested and retained for possible use in reconstruction of the floor of the sella after removing the tumor. A posterior septectomy of approximately 15 to 20 mm is then performed with a backbiter typically placed through the left nostril. Care should be taken to not extend the septectomy too far superiorly or anteriorly, which can increase the risk of anosmia and nasal deformity. The sphenoidotomy is then further refined based upon the pathology being addressed in the sella. In general, however, removal of bone and mucosa should extend beyond the lateral edges of the ostia bilaterally to allow visualization of the tuberculum sella, floor of the sella, opticocarotid recesses, clival recess, and lateral sphenoid recesses. Posterior ethmoid air cells are also opened and removed to facilitate maneuverability of the endoscope and instrument superiorly.
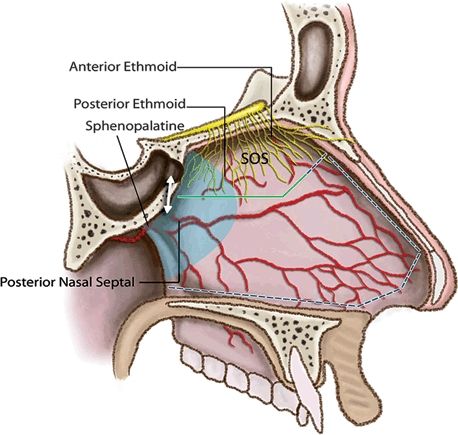
FIGURE 3.3 Illustration of NS rescue flap concept with preservation of sphenopalatine and posterior NS arteries and SOS. The mucosal incisions are started several millimeters below the inferior aspect of the sphenoid ostia and carried anteriorly as shown by the green line. The dotted line shows mucosal incisions if a complete NS flap is needed. The double arrow denotes the 9-mm distance typically between the inferior edge of the ostium and posterior nasal septal artery. The blue shading indicates the extent of the posterior septectomy. (Image copyright Daniel Kelly Brain Tumor Center 2012.)

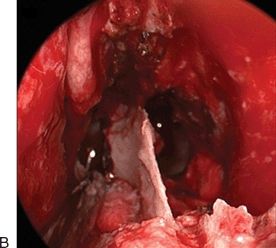
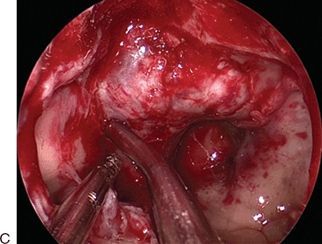
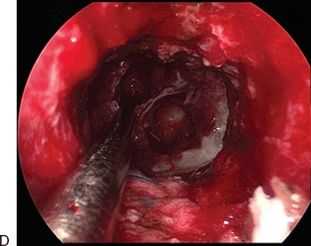
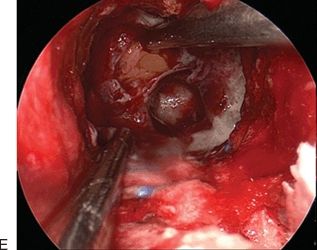
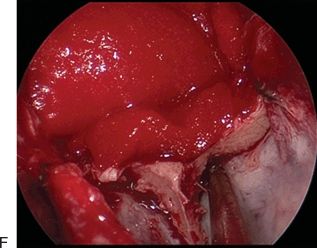
FIGURE 3.4 Intraoperative photographs with 0-degree endoscope of bilateral nasoseptal “rescue flaps” being created and preserved during tumor removal and at procedure completion. A. Sphenoid keel exposed and right rescue flap pushed down by long Cottonoid; left rescue flap being pushed downward as Cottonoid is being placed. B. Posterior septectomy completed, and both rescue flaps pushed downward by bilateral Cottonoids. C. Sphenoidotomy completed and Doppler probe localizing right cavernous carotid artery. D. After removing the tumor, view from posterior nasal cavity showing no obstruction from rescue flaps. E. Adipose tissue graft being placed into sella for reconstruction for CSF leak. F. After reconstruction is completed with adipose tissue graft and collagen sponge, Cottonoids are removed, and rescue flaps are replaced.
Sellar Exposure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


