7 Transotic Approach
Indications
• Some cases of cerebellopontine angle tumor with anterior extension and normal facial nerve function preoperatively (e.g., epidermoids).
• Some cases of petrous bone cholesteatoma.
• Some cases of petrous bone tumor with normal facial nerve function preoperatively.
• Some cases of vestibular schwannoma with invasion of the turns of the cochlea.
Surgical Steps (Figs. 7.1–7.36)
1. After the blind-sac closure of the external auditory canal (EAC), the remaining skin covering the bony portion of the canal is removed together with the tympanic membrane and ossicular chain. This step is carried out under the microscope in order to avoid leaving any skin remnants.
2. A canal wall-down mastoidectomy is carried out, with additional skeletonization of the middle fossa dura, the sigmoid sinus, and the posterior fossa dura. These structures are only skeletonized; the decision on whether or not to remove the overlying bone depends on the level of exposure required and is judged in accordance with the pathology being treated.
3. The facial nerve (FN) is skeletonized from the stylomastoid foramen to the geniculate ganglion (GG) without removing the overlying bone, which serves to protect the nerve later on.
4. Labyrinthectomy and skeletonization of the internal auditory canal (IAC) are carried out in the same manner as in the translabyrinthine and transcochlear approaches.
5. After the complete skeletonization of the IAC, the infralabyrinthine air cells are drilled out using a diamond burr of the appropriate size. Care should be taken when performing this step to avoid injuring the jugular bulb, lying inferiorly, and the posterior fossa dura, lying medially. It should also be noted that the medial aspect of the fallopian canal should not be overthinned, as it acts as the main support for the nerve after the approach has been completed.
6. Drilling of the inferior tympanic bone and the anterior wall is carried out.
7. Drilling now is started in the area anterior to the mastoid segment of the FN. Extreme care should be taken when carrying out the subsequent steps to avoid injuring this segment of the nerve. In general, injury to the mastoid segment rarely results directly from the rotating burr, as surgeons pay good attention to this. However, the rotating shaft of the burr is often forgotten. When there is prolonged contact between it and the nerve, it can result in heat injury to the nerve. Sometimes an instrument introduced wrongly into the middle ear space medial or lateral to the skeletonized nerve can fracture the bony covering and lead to FN paralysis. For this reason, adequate attention to these steps cannot be overemphasized.
8. Identification of the internal carotid artery can be started from the eustachian tube, which lies superior lateral to the artery or just at the anterior border of the cochlea, the middle turn of which lies behind the genu of the artery. Care should be taken when drilling in the area of the eustachian tube, as the bony septum between the two is sometimes dehiscent and injury to the artery can be sustained. For this reason, a large diamond burr should be used whenever drilling in the region of the internal carotid artery (ICA).
9. After identification of the ICA, the cochlea is drilled. The reason for this sequence is that being aware of the location of the artery helps to avoid injury to it. Drilling of the cochlea is started using a medium-sized cutting burr. When the middle turn is reached, the burr is exchanged for a diamond one to ensure the safety of the ICA. The remaining part of the cochlea and the bone overlying the posterior fossa dura and lying anterior to the internal auditory canal is removed, thus completing the skeletonization of the canal.
10. Further skeletonization of the ICA is continued if required.
11. At the end of the approach, the facial nerve is seen lying as a bridge in the middle of the approach.
Hints and Pitfalls
• When drilling anterior to the facial nerve, care should be taken to avoid injuring the nerve with the rotating shaft of the burr.
• In some cases, bone removal superior to the internal auditory canal is needed to obtain proper control of the superior pole of the tumor. Because of the proximity of the middle fossa dura, this may prove difficult. The middle fossa dura is therefore completely uncovered and gently retracted with suction aspiration.
• The transotic approach avoids facial nerve mobilization and therefore makes it possible to preserve perfect function.
• The facial nerve is left like a bridge in the middle of the approach. This limits the control of the internal carotid artery and petrous apex. In addition, the nerve itself may be endangered if rough manipulations break the fallopian canal.
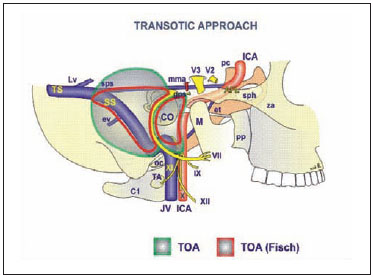
Fig. 7.1 The structures exposed by the transotic approach (TOA). Note that the amount of bone removed in the extended transotic approach (green shaded area) provides wider exposure in comparison with the classic transotic approach developed by Fisch. See (Fig. 4.1), p. 57, forkey to abbreviations.
Fig. 7.2 The skin incision is made as shown.
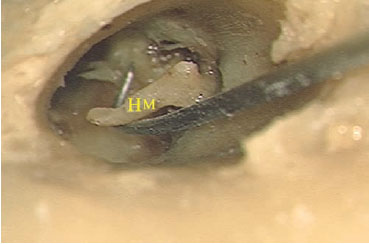
Fig. 7.3 The skin of the external auditory canal of a left temporal bone has been removed, and the handle of the malleus (HM) is being pulled using a hook.

Fig. 7.4 The expected levels of the middle cranial fossa (MF) and sigmoid sinus (SS) have been identified
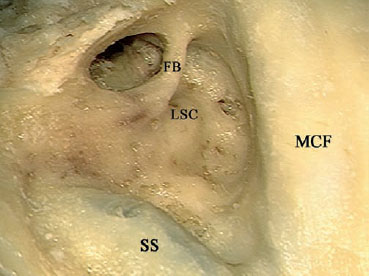
Fig. 7.5 The mastoid cavity has been drilled out, and the posterior and superior canal walls have been lowered. FB Facial bridge, LSC Lateral semicircular canal, MCF Middle cranial fossa, SS Sigmoid sinus
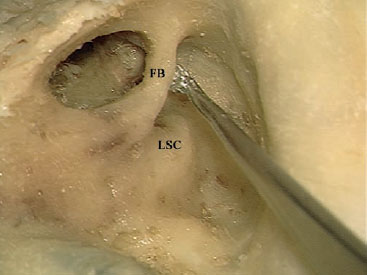
Fig. 7.6 A curette is used to remove the facial bridge (FB). LSC Lateral semicircular canal
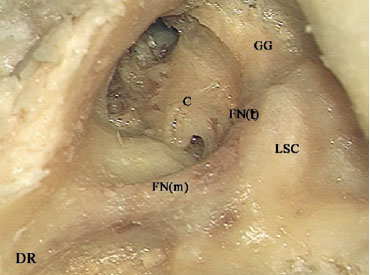
Fig. 7.7 The facial nerve has been skeletonized from the digastric ridge (DR) to the geniculate ganglion (GG). C Basal turn of the cochlea (promontory), FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, LSC Lateral semicircular canal
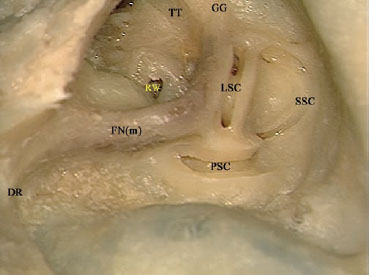
Fig. 7.8 The lateral semicircular canal (LSC), posterior semicircular canal (PSC), and superior semicircular canal (SSC) have been opened. DR Digastric ridge, FN(m) Mastoid segment of the facial nerve, GG Geniculate ganglion, RW Round window, TT Tensor tympani
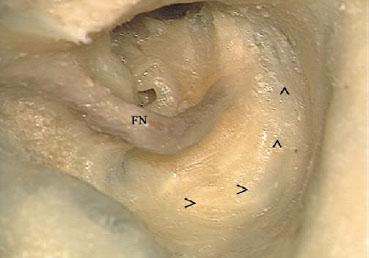
Fig. 7.9 The arrows show the semicircular movement of the drill for skeletonization of the internal auditory canal. FN Facial nerve
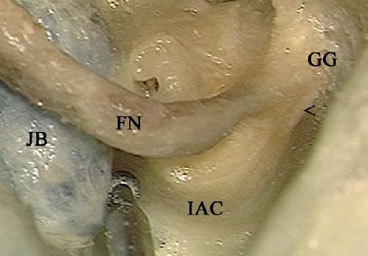
Fig. 7.10 Theinternal auditorycanal (IAC) hasbeen identified. Note the high jugular bulb (JB), almost touching the canal. Drilling of the intervening bone should proceed with extreme caution, using a small diamond drill. < Labyrinthine segment of the facial nerve, FN Facial nerve, GG Geniculate ganglion

Fig. 7.11 Note that the inferior and anterior canal wall (^ ^) are overhanging here, obscuring the required view.
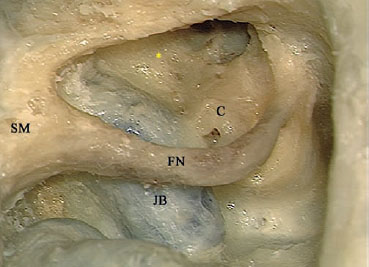
Fig. 7.12 The overhanging part of the canal wall has been drilled. The jugular bulb (JB) anterior to the facial nerve (FN) and the location of the internal carotid (*) artery are now visible. C Basal turn of the cochlea (promontory), SM Stylomastoid foramen
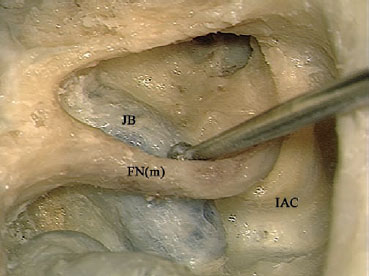
Fig. 7.13 Note that the contact seen here between the burr shaft and the facial nerve (FNm) is extremely dangerous and should be avoided. IAC Internal auditory canal, JB Jugular bulb
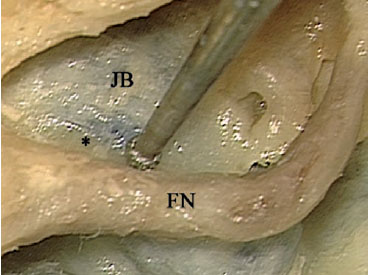
Fig. 7.14 The bone (*) between the jugular bulb (JB) and facial nerve (FN) is carefully removed using an appropriately sized diamond burr

Fig. 7.15 Identification of the internal carotid artery is either started from the eustachian tube, where the burr is located, or at the anteroinferior limit of the promontory (*). A diamond burr should be used in both cases.
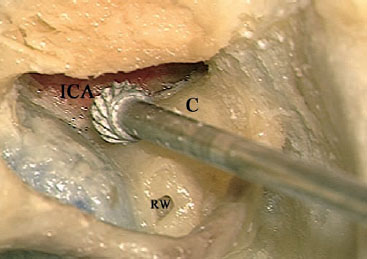
Fig. 7.16 After identification of the internal carotid artery (ICA), a cutting burr is used initially to open the cochlea (C). RW Round window
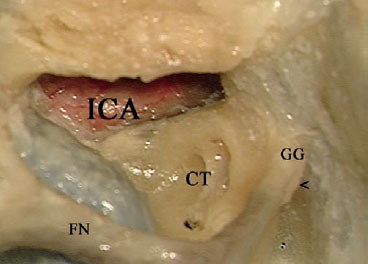
Fig. 7.17 Due to its proximity to the internal carotid artery (ICA), the internal last part of the cochlea (CT) should be drilled away using a small diamond burr. < Labyrinthine segment of the facial nerve, FN Facial nerve,
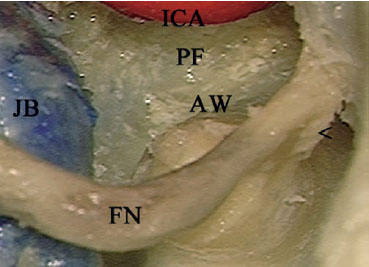
Fig. 7.18 The cochlea has been drilled out, the anterior wall of the internal auditory canal (AW) has been skeletonized, and the posterior fossa mond dura (PF) has been identified. < Labyrinthine segment of the facial nerve, FN Facial nerve, ICA Internal carotid artery, JB Jugular bulb
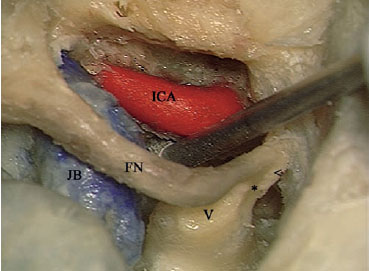
Fig. 7.19 If necessary, further drilling of the bone medial to the internal carotid artery (ICA) can be carried out. * Bill’s bar, < Labyrinthine segment of the facial nerve, FN Facial nerve, JB Jugular bulb, V Vestibule

Fig. 7.20 The clivus bone (CL) can be seen medial to the internal carotid artery (ICA). JB Jugular bulb
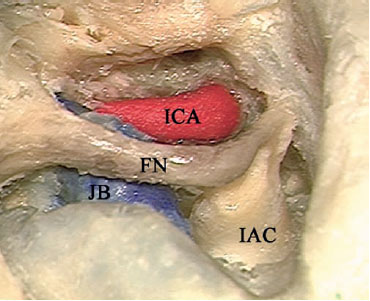
Fig. 7.21 The bone lateral to the vertical internal carotid artery (ICA) has also been drilled. FN Facial nerve, IAC Internal auditory canal, JB Jugular bulb
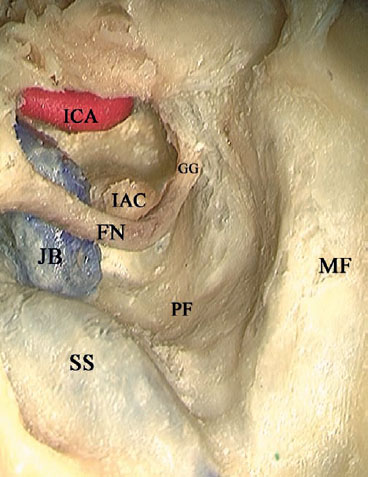
Fig. 7.22 The vertical view after the approach has been completed. Note that the facial nerve (FN) lies like a bridge in the middle of the field, limiting the surgical access. GG Geniculate ganglion, IAC Internal auditory canal, ICA Internal carotid artery, JB Jugular bulb, MF Middle fossa level, PF Posterior fossa, SS Sigmoid sinus
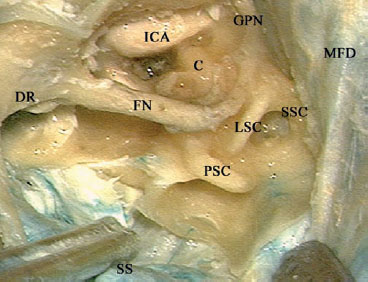
Fig. 7.23 In this left temporal bone, the bone overlying the middle fossa dura (MFD), sigmoid sinus (SS), and posterior fossa dura has already been uncovered and removed, and the facial nerve (FN), internal carotid artery (ICA), and lateral (LSC), posterior (PSC), and superior (SSC) semicircular canals have been skeletonized. C Cochlea, DR Digastric ridge, GPN Greater petrosal nerve
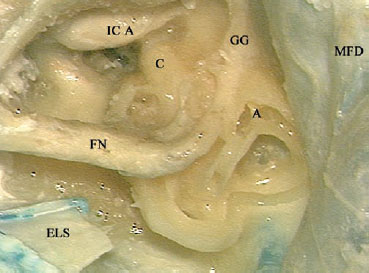
Fig. 7.24 The semicircular canals have been opened. A Ampullae of the lateral and superior semicircular canals, C Cochlea, ELS Cut endolymphatic sac, FN Facial nerve, GG Geniculate ganglion, ICA Internal carotid artery, MFD Middle fossa dura
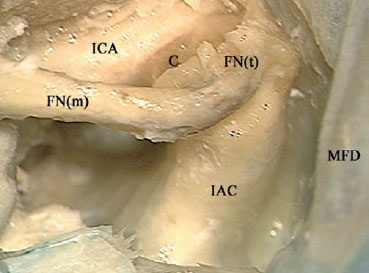
Fig. 7.25 Labyrinthectomy has been completed and the internal auditory canal (IAC) has been skeletonized. C Cochlea, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, ICA Internal carotid artery, MFD Middle fossa dura
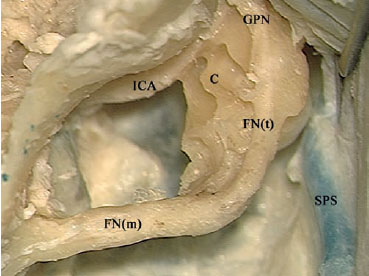
Fig. 7.26 The cochlea (C) has been opened. FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GPN Greater petrosal nerve, ICA Internal carotid artery, SPS Superior petrosal sinus
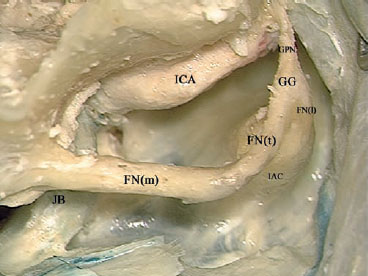
Fig. 7.27 The cochlea has been completely drilled away, and the vertical portion of the internal carotid artery (ICA) has been skeletonized. FN(l) Labyrinthine segment of the facial nerve, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, GPN Greater petrosal nerve, IAC Internal auditory canal, JB Jugular bulb
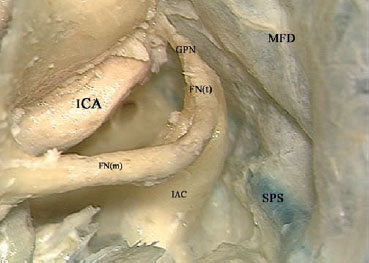
Fig. 7.28 The view after the approach has been completed. FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GPN Greater petrosal nerve, IAC Internal auditory canal, ICA Internal carotid artery, MFD Middle fossa dura, SPS Superior petrosal sinus
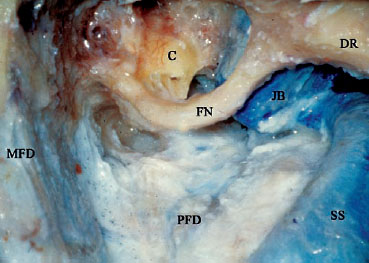
Fig. 7.29 In this cadaveric dissection on the right side, skeletonization of the facial nerve (FN) has been completed from the stylomastoid foramen at the anterior border of the digastric ridge (DR) as far as the internal auditory canal. C Cochlea, JB Jugular bulb, MFD Middle fossa dura, PFD Posterior fossa dura, SS Sigmoid sinus
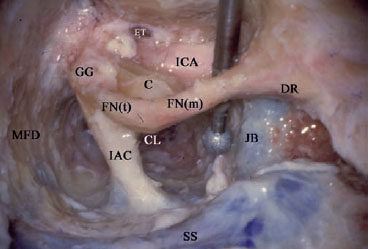
Fig. 7.30 Drilling is now started in the area anterior to the mastoid segment of the facial nerve (FNm). Extreme care should be taken not to injure this segment with the rotating burr or its shaft. C Cochlea, CL Clivus, DR Digastric ridge, ET Eustachian tube, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, IAC Internal auditory canal, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura, SS Sigmoid sinus
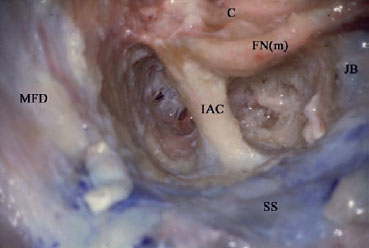
Fig. 7.31 The view after completion of the previous step. C Cochlea, FN(m) Mastoid segment of the facial nerve, IAC Internal auditory canal, JB Jugular bulb, MFD Middle fossa dura, SS Sigmoid sinus
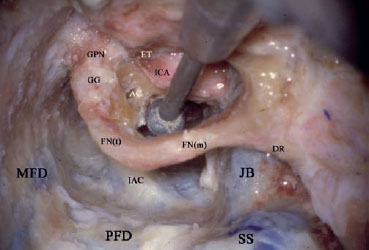
Fig. 7.32 A medium-sized diamond burr is used to drill the cochlea in the region of the internal carotid artery (ICA). AC Apical turn of the cochlea, DR Digastric ridge, ET Eustachian tube, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, GPN Greater petrosal nerve, IAC Internal auditory canal, JB Jugular bulb, MFD Middle fossa dura, PFD Posterior fossa dura, SS Sigmoid sinus
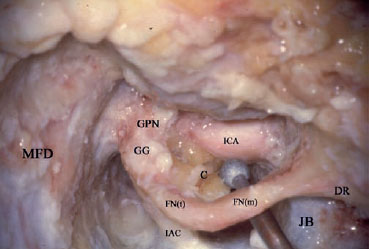
Fig. 7.33 The remaining part of the cochlea and the bone overlying the posterior fossa dura are removed. C Cochlea, DR Digastric ridge, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, GPN Greater petrosal nerve, IAC Internal auditory canal, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura
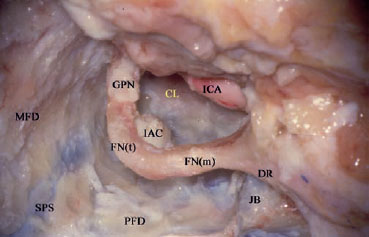
Fig. 7.34 At the end of the approach, the facial nerve is seen lying as a bridge in the middle of the approach. CL Clivus, DR Digastric ridge, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GPN Greater petrosal nerve, IAC Internal auditory canal, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura, PFD Posterior fossa dura, SPS Superior petrosal sinus
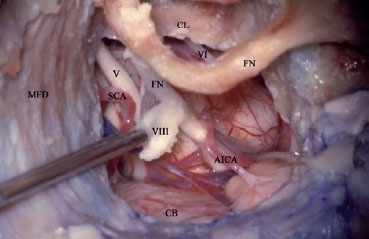
Fig. 7.35 The intracranial structures that can be seen using the transotic approach. Note that the facial nerve lies like a bridge in the middle of the approach, obstructing access to the cerebellopontine angle. V Trigeminal nerve, VI Abducent nerve, VIII Cochlear nerve, AICA Anterior inferior cerebellar artery, CB Cerebellum, CL Clivus bone, FN Facial nerve, MFD Middle fossa dura, SCA Superior cerebellar artery
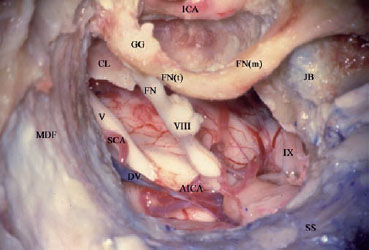
Fig. 7.36 In the lower part of the approach, the glossopharyngeal nerve (IX) can be seen. V Trigeminal nerve, VIII Cochlear nerve, AICA Anterior inferior cerebellar artery, CL Clivus bone, DV Dandy’s vein, FN Facial nerve, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura, SCA Superior cerebellar artery, SS Sigmoid sinus
< div class='tao-gold-member'>



