6 Retrosigmoid–Retrolabyrinthine Approach
Indications
• Hearing preservation surgery for small vestibular schwannomas (less than 2 cm) with absence of involvement of the fundus of the internal auditory canal.
• Hearing preservation surgery for other cerebellopontine angle tumors in which the major part of the tumor is located posterior to the internal auditory canal.
Surgical Steps (Figs. 6.1–Figs. 6.23)
1. The supine position is used. A retroauricular skin incision is performed as shown.
2. A U-shaped, inferiorly based musculoperiosteal flap is elevated.
3. An extended mastoidectomy is carried out. The bone covering the middle fossa dura is removed for a distance of 1–2cm. In contrast to the translabyrinthine approach, the bony covering of the posterior fossa dura is removed here up to the posterior edge of the sigmoid sinus only; removal is not extended posteriorly beyond this level. The mastoid emissary vein is skeletonized and closed.
4. All the air cells in the mastoid cavity should be removed and the semicircular canals identified. In cases of extensive pneumatization, as many perilabyrinthine air cells as possible should be drilled out. Any remaining air cells in the region should be occluded using bone wax. This step is extremely important for avoiding postoperative cerebrospinal fluid (CSF) leakage in live surgery.
5. Since the aim of this operation is to preserve hearing, the utmost care must be taken when carrying out the retrolabyrinthine part of the approach. Drilling must always be parallel to the semicircular canal being identified, and the overlying bone should not be overthinned in order not to risk opening the labyrinth.
6. A 5 × 5-cm craniotomy is carried out using a diamond burr. The sigmoid sinus is followed to the transverse sinus, and the craniotomy should be located posterior to the sigmoid sinus and inferior to the transverse sinus.
7. The bone flap is separated from the underlying dura using a septal dissector. The lower edge of the craniotomy is trimmed using a rongeur. The sigmoid sinus is also uncovered. The bone flap is then removed and placed in a saline solution.
8. The dura is held using a toothed forceps, and a small incision is made. In live surgery, Merocel is inserted between the dura and the cerebellum in the lines of the incision, to provide protection for the cerebellum.
9. Once the dura has been opened, the dural flaps are retracted using stay sutures.
10. In live surgery, the cerebellum lies just underneath the dura, narrowing the approach. Gentle retraction of the cerebellum allows space for identifying the cistern. Opening of the arachnoid of the cistern should be carried out carefully, parallel to the direction of the lower cranial nerves and above the level of the glossopharyngeal nerve. This step results in the escape of the cerebrospinal fluid and therefore shrinkage of the cerebellum, providing the necessary space for tumor removal.
11. An inverted U-shaped dural flap is outlined on the posterior surface of the petrous bone. The long limbs lie a few millimeters inferior and superior to the internal auditory canal porus. The dura is incised using a sharp dissector or a Beaver knife. The dural flap is elevated from the underlying bone to the level of the porus. The flap can then be excised.
12. In live surgery, Gelfoam is inserted far anteriorly into the cerebellopontine angle and around the porus of the internal auditory canal, to prevent bone dust from falling into the cisterns.
13. Using a diamond burr, drilling of the posterior wall of the internal auditory canal now begins, starting from the porus and moving laterally.
14. Drilling continues until the common crus is blue-lined. The superior and posterior semicircular canals are also blue-lined just before they join into the common crus. This is the most lateral limit of drilling. If there is any doubt, examining the retrolabyrinthine part of the approach provides an adequate idea of the position of the canals.
15. The posterior wall of the internal auditory canal (as far as the blue-lined common crus) is now completely drilled. The internal auditory canal dura is opened next.
16. In live surgery, the tumor inside the internal auditory canal is removed from medial to lateral. If there is still residual tumor in the fundus area, angled instruments are used to remove it. At the end, an endoscope is used to ascertain that no residual tumor has been left behind.
17. If the tumor extends more laterally into the internal auditory canal, beyond the limit of visual control, then tumor removal can be carried out using one of the following methods:
• Exposing the fundus at the superior aspect of the internal auditory canal. To achieve this additional exposure, the dura overlying the petrous ridge and the superior surface of the petrous bone should be carefully elevated. Drilling is then shifted to the anterosuperior aspect of the internal auditory canal. The superior semicircular canal is then skeletonized. Following the anterior surface of the superior semicircular canal will lead to the fundus. The problem with this extension is the fact that the additional exposure of the fundus is very narrow and the procedure itself caries a risk of opening the labyrinth, resulting in hearing loss.
• Labyrinth drill-out. This is only applicable in cases of doubt. However, it is the surest way of eliminating the risk of residual tumor.
18. After tumor removal from the internal auditory canal, fibrin glue and a free muscle graft are used to close the internal auditory canal, while bone wax is used to close all the open air cells to avoid postoperative CSF leakage.
19. Watertight closure of the dura should be attempted, to reduce the risk of postoperative CSF leakage. If a small dural defect is noticed, a piece of muscle can be used to seal the defect, and can be fixed with a transfixion suture.
20. The bone flap (craniotomy) is turned back. This prevents contact between the muscles of the neck and the posterior fossa dura, reducing the incidence of postoperative headache.
21. Abdominal fat is used to obliterate the mastoid cavity.
Hints and Pitfalls
• Most surgeons use a vertical or slightly curved skin incision. The exposure required is achieved using retractors, which have the disadvantage of making the surgical field deeper and the working angle more acute. We prefer a wide C-shaped incision and suturing the edges of the incision. Although this is more time-consuming, it removes the need for retractors.
• Complete exposure of the sigmoid sinus allows it to be displaced forward with the dural flap, thus providing wider exposure. Exposure of the transverse sinus allows the surgeon to be aware of the exact upper limit of the approach.
• Combining a retrolabyrinthine mastoidectomy with dural exposure to the retrosigmoid has several advantages:
–The most important is the reduction of the incidence of cerebrospinal fluid leakage. The removal of the air cells in this area interrupts potential pathways between the intradural cavity and the middle ear, and filling the cavity with fat at the end of the approach adds to the seal.
–Another advantage of this combination is the fact that the sigmoid sinus and the attached dura can be retracted anteriorly, adding to the available space.
–The semicircular canal can be located more easily through the retrolabyrinthine part of the approach.
• If deep perilabyrinthine air cells are present, bone wax is used to seal them.
• Before drilling is started in the posterior wall of the internal auditory canal, the Merocel strips are removed to prevent them from becoming entangled in the burr. Gelfoam is placed in the angle and around the internal auditory canal mainly inferior to it, to avoid dispersion of bone dust in the cistern. The cerebellum is gently retracted, a large diamond burr is used, and drilling is carried out under continuous suction irrigation. Drilling should be carried out parallel to the direction of the internal auditory canal and from medial to lateral.
• Various landmarks have been proposed to help avoid injury to the labyrinth during drilling of the posterior wall of the internal auditory canal. These include the singular canal, the transverse crest, and the vestibular aqueduct. We find that the vestibular aqueduct is a constant landmark, since it lies immediately medial and inferior to the common crus. However, during surgery, identification of the vestibular aqueduct may be difficult. In such cases, we prefer blue-lining of the common crus. This method involves a risk of opening the labyrinth while blue-lining it. Another method is to follow the dura of the canal and drill laterally (about 6–7 mm) until the dura becomes narrower. This method lacks any specific landmark for the point at which drilling should stop. It does not provide the maximum possible exposure of the internal auditory canal, but involves less risk to the labyrinth. Residual tumor at the level of the fundus can be checked by endoscopy.
• While the internal auditory canal is being drilled, a wide area of bone should be removed—i.e., superior and inferior to the canal, rather than just exposing only the posterior wall. This allows more space for safer tumor removal, and reduces the risk to the facial nerve.
• A high jugular bulb reaching up to the level of the inferior border of the internal auditory canal is present in about 10% of cases. In these cases, the bulb may be injured while the posterior wall of the internal auditory canal is being drilled, with subsequent profuse bleeding that may even make it necessary to terminate the procedure.
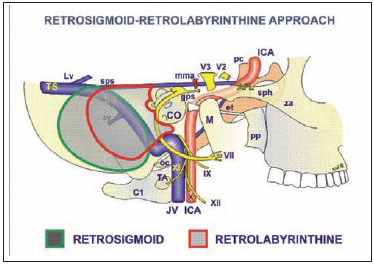
Fig. 6.1 The structures controlled by the combined retrosigmoid—retrolabyrinthine approach. See Fig. 4.1, p. 57, for key to abbreviations.
Fig. 6.2 The skin incision is made as shown.
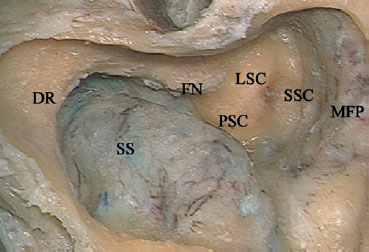
Fig. 6.3 An extended mastoidectomy has been achieved in a left temporal bone. DR Digastric ridge, FN Facial nerve, LSC Lateral semicircular canal, MFP Middle fossa plate, PSC Posterior semicircular canal, SS Sigmoid sinus, SSC Superior semicircular canal
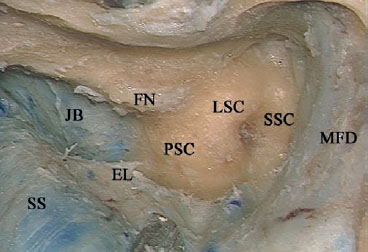
Fig. 6.4 The dura has been uncovered from the overlying bone. Note the high jugular bulb (JB), touching the posterior semicircular canal (PSC). EL Endolymphatic duct, FN Facial nerve, LSC Lateral semicircular canal, MFD Middle fossa dura, SS Sigmoid sinus, SSC Superior semicircular canal
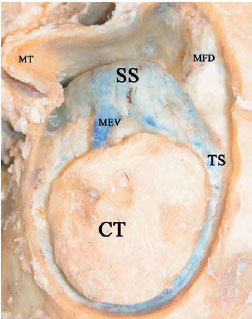
Fig. 6.5 A 5 × 5-cm craniotomy flap (CT) has been created. Note that the craniotomy should be located posterior to the sigmoid sinus (SS) and inferior to the transverse sinus (TS). MEV Mastoid emissary vein, MFD Middle fossa dura, MT Mastoid tip
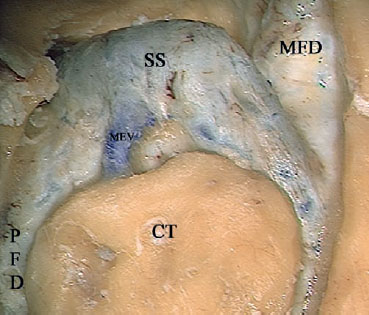
Fig. 6.6 At higher magnification. CT Craniotomy, MEV Mastoid emissary vein, MFD Middle fossa dura, PFD Posterior fossa dura, SS Sigmoid sinus
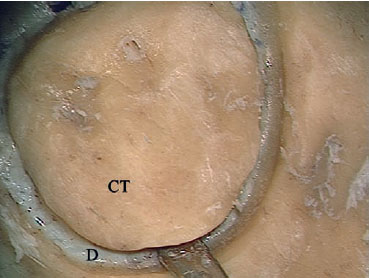
Fig. 6.7 A septal raspatory is used to detach the craniotomy flap (CT) from the underlying posterior fossa dura (D).

Fig. 6.8 The craniotomy flap is separated from the dura. MT Mastoid tip, PFD Posterior fossa dura, SS Sigmoid sinus
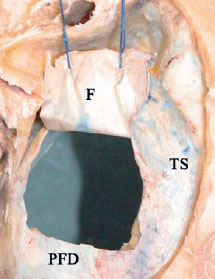
Fig. 6.9 An anteriorly based flap (F) is created in the posterior fossa dura (PFD) and fixed anteriorly using sutures. TS Transverse sinus
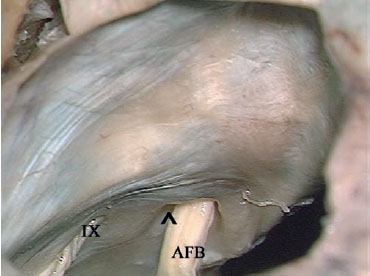
Fig. 6.10 Through the craniotomy, the acousticofacial bundle (AFB) can be seen entering the internal auditory canal (^). IX Glossopharyngeal nerve
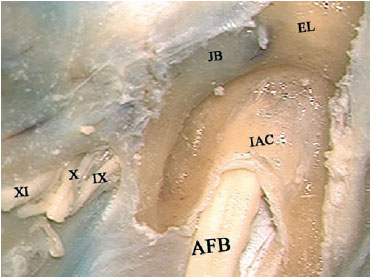
Fig. 6.11 Identification of the internal auditory canal (IAC) has been achieved by following from the porus medially until the endolymphatic duct (EL) started to show through the bone laterally. Note the high jugular bulb (JB). IX Glossopharyngeal nerve, X Vagus nerve, XI Accessory nerve, AFB Acousticofacial bundle
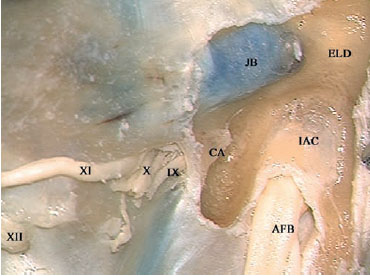
Fig. 6.12 Drilling has been carried out more inferiorly to identify the cochlear aqueduct (CA). Note the proximity of the aqueduct to the glossopharyngeal nerve (IX). X Vagus nerve, XI Accessory nerve, XII Hypoglossal nerve, AFB Acousticofacial bundle, ELD Endolymphatic duct, IAC Internal auditory canal, JB Jugular bulb
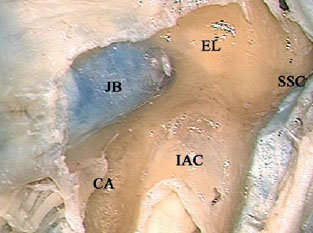
Fig. 6.13 The dura overlying the superior aspect of the internal auditory canal (IAC) has been elevated, and identification of the superior semicircular canal (SSC) has been started in order to reach to the fundus. CA Cochlear aqueduct, EL Endolymphatic duct, JB Jugular bulb
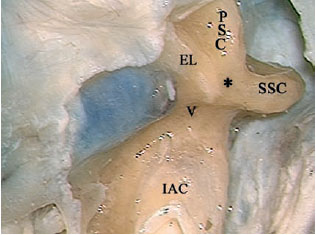
Fig. 6.14 Both the superior (SSC) and posterior (PSC) semicircular canals have been skeletonized. The endolymphatic duct (EL) can be seen lying posterior to the junction of the common crus (*), with the vestibule (V). IAC Internal auditory canal

Fig. 6.15 At the fundus, Bill’s bar (*) can be seen separating the labyrinthine segment of the facial nerve (L) from the superior vestibular nerve (SV). IX Glossopharyngeal nerve, X Vagus nerve, C Cochlear nerve, CA Cochlear aqueduct, EL Endolymphatic duct, FN(i) Internal auditory canal segment of the facial nerve, GG Geniculate ganglion, IV Inferior vestibular nerve, JB Jugular bulb, PSC Posterior semicircular canal, SSC Superior semicircular canal
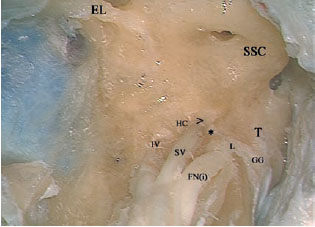
Fig. 6.16 At higher magnification, the relationship between the nerves in the fundus area can be better appreciated. * Bill’s bar, > Superior ampullary canal, EL Endolymphatic duct, FN(i) Internal auditory canal segment of the facial nerve, GG Geniculate ganglion, HC Horizontal crest, IV Inferior vestibular nerve, L Labyrinthine segment of the facial nerve, SSC Superior semicircular canal, SV Superior vestibular nerve entering the superior ampullary canal, T tympanic segment of the facial nerve

Fig. 6.17 The superior semicircular canal (SSC) and posterior semicircular canal (PSC) have been opened and can be seen as they join to form the common crus (CC) and enter the vestibule. CA Cochlear aqueduct, EL Endolymphatic duct, F Facial nerve, JB Jugular bulb, V Vestibule
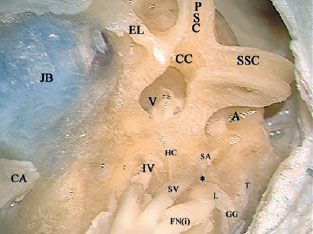
Fig. 6.18 The view at higher magnification. * Bill’s bar, A Ampulla of the superior canal, CA Cochlear aqueduct, CC Common crus, EL Endolymphatic duct, FN(i) Internal auditory canal segment of the facial nerve, GG Geniculate ganglion, HC Horizontal crest, IV Inferior vestibular nerve, JB Jugular bulb, L Labyrinthine segment of the facial nerve, PSC Posterior semicircular canal, SA Superior ampullary nerve, SSC Superior semicircular canal, SV Superior vestibular, T Tympanic segment of the facial nerve, V Vestibule
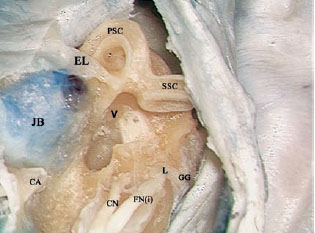
Fig. 6.19 The vestibular nerves have been removed, the vestibule (V)has been completely opened, and the cochlear nerve entering the modiolus (C) is visible inside. CA Cochlear aqueduct, CN Cochlear nerve within the internal auditory canal, EL Endolymphatic duct, FN(i) Internal auditory canal segment of the facial nerve, GG Geniculate ganglion, JB Jugular bulb, L Labyrinthine segment of the facial nerve, PSC Posterior semicircular canal, SSC Superior semicircular canal
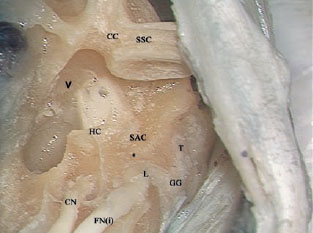
Fig. 6.20 The view at higher magnification. * Bill’s bar, C Cochlear nerve entering the modiolus, CC Common crus, CN Cochlear nerve within the internal auditory canal, FN(i) Internal auditory canal segment of the facial nerve, GG Geniculate ganglion, HC Horizontal crest, L Labyrinthine segment of the facial nerve, SAC, SSC Superior semicircular canal, T Tympanic segment of the facial nerve, V Vestibule
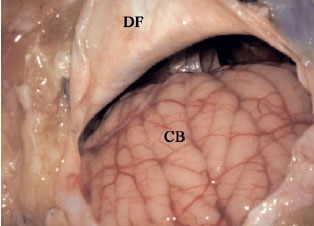
Fig. 6.21 A cadaveric dissection to show the intradural structures exposed by this approach. The dural flap (DF) has been created and reflected anteriorly, and the cerebellum (CB) can be seen.
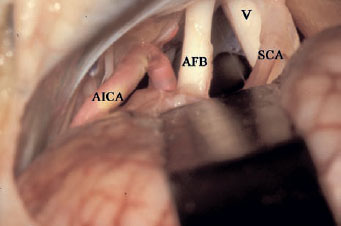
Fig. 6.22 The cerebellar retractor has been applied and the cerebellopontine angle opened. V Trigeminal nerve, AFB Acousticofacial bundle, AICA Anterior inferior cerebellar artery, SCA Superior cerebellar artery
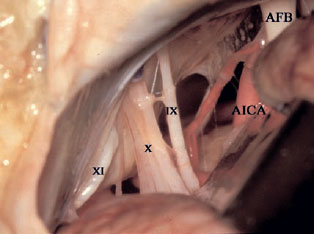
Fig. 6.23 The lower cranial nerves are visible in the lower part of the approach. IX Glossopharyngeal nerve, X Vagus nerve, XI Accessory nerve, AFB Acousticofacial bundle, AICA Anterior inferior cerebellar artery
< div class='tao-gold-member'>



