8 Modified Transcochlear Approach (Type A)
Indications
• Extradural lesions: extensive petrous apex lesions with preoperative facial nerve and inner ear loss of function, e.g.:
–Petrous bone cholesteatoma of the massive, infralabyrinthine apical and (less commonly) supralabyrinthine types.
–Recurrent acoustic neurinoma with petrous bone invasion and facial nerve paralysis.
–Extensive facial nerve tumors.
• Intradural lesions:
–Large clival and petroclival lesions lying ventral to the brainstem; e. g., petroclival meningiomas.
–Residual or recurrent nonacoustic lesions of the posterior fossa with anterior extension into the prepontine cistern, particularly those with encasement of the vertebrobasilar artery or perforating arteries, or both; e. g., huge posterior fossa epidermoids.
–Recurrent acoustic neurinomas with facial nerve paralysis.
• Transdural lesions: invading the petrous apex as en-plaque meningiomas, or primary clival or temporal bone lesions with secondary posterior fossa extension such as chordomas, chondrosarcomas, and extensive glomus jugulare tumors.
Surgical Steps (Figs. 8.1–8.51)
1. After blind-sac closure of the external auditory canal, the skin covering the bony part of the external auditory canal (EAC) should be removed under the microscope. Mastoidectomy is started by creating the triangle of attack; the middle fossa dura and the sigmoid sinus are identified, and the posterior canal wall is thinned and lowered to the level of the annulus.
2. The remnants of the tympanic membrane and the ossicles are removed.
3. The digastric ridge is identified and the facial nerve skeletonized.
4. The nerve can now be seen extending from the stylomastoid foramen at the anterior edge of the digastric ridge to the second genu, housed within the curvature of the lateral semicircular canal (LSC). From here, the tympanic segment of the facial nerve (FN) runs anteriorly under the LSC to reach the geniculate ganglion (GG) superior to the cochleariform process.
5. Depending on the pathology being treated and thus the level of exposure required, a decision is taken on whether to uncover the middle fossa dura and sigmoid sinus. Whether these structures are to be uncovered or not, the edges of the cavity should be rounded and smoothed, and the bone overlying the dura and sinus should be thinned to a very fine shell.
6. If these structures are to be uncovered, a Freer periosteal elevator is used to separate the dura from the remaining bony shell, in the same way as in the translabyrinthine approach.
7. Labyrinthectomy is started by drilling the LSC. Care must be taken at this point not to injure the second genu of the FN, which lies within the curvature of the canal. Leaving the inferior wall of the canal intact will provide the necessary protection.
8. Following the cavity of the LSC superiorly will lead to the joint ampulla of the lateral and superior canals. From here, the cavity of the superior semicircular canal can be followed posteriorly to reach common crus, which is formed by the union of the nonampullated ends of the superior and posterior canals.
9. Leaving the anterior wall of the ampulla of the superior semicircular canal (SSC) intact serves to protect the tympanic and labyrinthine segments of the nerve from drilling injury, as well as providing a sign for the upper border of the internal auditory canal (IAC).
10. Following the posterior canal at this point will lead to its ampullated end, which lies a few millimeters medial to the mastoid segment of the FN. Again, care must be taken here to avoid injuring the nerve.
11. The endolymphatic sac is encountered between the sigmoid sinus (SS) and the posterior semicircular canal (PSC). Passing from behind and medial to the canal to enter between the layers of the dura, this structure exerts tension, hampering the dural retraction. In order to release the dura at this position, a Beaver knife with the sharp border directed against the bone is used to cut the endolymphatic duct.
12. The vestibule is now opened carefully. Since the genu of the FN lies at its lateral wall lies and the fundus of the IAC lies at its medial wall, the direction of drilling in this area should be parallel to these walls in a superior to inferior direction, or vice versa, and never from medial to lateral. The posterior edge of the lateral wall of the vestibule should be cautiously reduced. Although a very small amount of bone needs to be removed at this location, its removal is crucial for adequate visualization of the IAC.
13. The ampulla of the SSC serves as the landmark for the level of the superior border of the IAC. The bone between the middle fossa dura and the IAC is now drilled using an appropriately sized diamond drill. Drilling in this area should proceed from medial to lateral. Care must be taken not to injure the dura or open the wall of the IAC, jeopardizing the FN lying within. In order to avoid such mishaps, a septal dissector is used to separate the dura from the bone to be drilled. During drilling, the dura should be retracted superiorly using suction irrigation. In live surgery, the middle fossa dura can be shrunk using bipolar coagulation under irrigation, adding to the dural retraction.
14. The inferior border of the IAC is then identified by drilling the retrofacial air cells lying between that border and the jugular bulb (JB) inferiorly. During drilling in this area, the cochlear aqueduct is identified. The importance of this structure lies in the fact that it serves as a landmark for the glossopharyngeal nerve, which lies just inferior to its level. Thus, identifying the cochlear aqueduct during drilling means that the lower limit of drilling has been reached. Opening the cochlear aqueduct in live surgery also helps to allow cerebrospinal fluid (CSF) to escape, relaxing the intradural tension and improving exposure.
15. Once the IAC has been identified, drilling is continued using an appropriately sized diamond burr, moving in a semicircular fashion from superior to posterior to inferior until only a transparent shell of bone is left covering the IAC.
16. Skeletonization of the mastoid and tympanic segments of the facial nerve is started using an appropriately sized diamond burr, moving in a direction parallel to the nerve under ample suction irrigation. Drilling should be continued until only a thin, transparent bony covering is left overlying the nerve. The bone overlying the area of the stylomastoid foramen should be completely removed, especially at the posterior aspect, in order to prevent the sharp bony remnants from injuring the FN while it is being rerouted.
17. On the posterior surface of the IAC fundus, the transverse crest is identified. This crest is the bar of bone separating the superior vestibular nerve and FN, lying superior to it, from the inferior vestibular nerve and cochlear nerve, lying inferior to it. Following the superior vestibular nerve from the superior level of the transverse crest laterally to the superior ampulla will lead to the canal of the superior ampullary nerve, which forms a very important landmark for safe identification of the FN at the fundus. At this level, Bill’s bar lies anterior to the superior ampullary nerve, protecting the FN from injury while the former is dislodged from its canal. A small cutting burr is used carefully to open the canal of the superior vestibular nerve. Drilling in the expected position of the canal is carried out until the whitish color of the canal starts to appear.
18. Bill’s bar is identified using a small diamond drill. The suction irrigation tube at this step helps to irrigate the field and to retract the dura away from the drill to prevent injury to it. While the dura is retracted, drilling is advanced to identify the labyrinthine segment of the FN. Again, adequate suction irrigation is vital to avoid injury. The drill should be moved parallel to the course of this segment, and the direction of rotation of the burr should be away from the nerve.
19. The bone overlying the GG is drilled using the same diamond drill. Adequate removal of the bone lying anterior to the GG and the sharp angle of bone lying between the labyrinthine segment and the GG is important to avoid injury to the nerve while it is being rerouted posteriorly.
20. The greater superficial petrosal nerve is followed from the anterior border of the GG, and the bone overlying it is drilled to uncover the nerve. In live surgery, the nerve is sharply cut after bipolar coagulation to prevent bleeding, since the major blood supply to the FN is carried via the petrosal branch of the middle meningeal artery, following the nerve.
21. The last shell of bone overlying the full course of the FN is now removed using a double-curved hook.
22. The decision to open the dura of the IAC depends on the extent of the pathology. In the cases where the intracanalicular portion of the FN is not involved, maintaining the integrity of the dura will help to maintain the blood supply to the remaining portion of the nerve and to prevent postoperative CSF leakage.
23. At the level of the fundus of the IAC, the inferior vestibular nerve is dislodged using a double-curved hook.
24. This is followed by dislodging the superior ampullary nerve from its canal using a small hook. The superior ampullary nerve is then dissected medially until the superior vestibular nerve is reached and the FN can be identified anterior to it.
25. Rerouting of the FN is started at the level of the GG. Using an angled pick and a Brackmann’s suction tube, the GG is dislodged and followed carefully to the labyrinthine segment of the nerve. This step is the most delicate step in the rerouting, and the facial nerve is most liable to injury at this level. This is because the labyrinthine segment is the thinnest part of the FN, due to the absence of an epineural covering, and due to the sharp bony angle between the GG and labyrinthine segment, which can injure this segment if extreme care is not taken.
26. The tympanic segment is next dissected free from the canal.
27. The fibrous and vascular attachments of the mastoid segment of the facial nerve to the medial aspect of the fallopian canal should be sharply dissected. The mastoid segment of the nerve should be freed down to the stylomastoid foramen.
28. The labyrinthine segment of the FN is followed as far as the IAC. If a decision not to open the dura has been made, the cochlear nerve is freed from its attachment at the fundus, and the dura covering the anterior wall of the IAC is elevated. The whole contents of the internal auditory canal, together with the rest of the FN, are now rerouted posteriorly and laid on the posterior fossa dura just anterior to the sigmoid sinus. A piece of aluminum obtained from the covering of the surgical threads is used to protect the rerouted nerve from injury during further manipulations and drilling.
29. The remaining part of the fallopian canal is removed either using a rongeur or using a large cutting burr, and the inferior part of the tympanic ring is widely drilled.
30. Drilling the cochlea is started using a large cutting burr. When the middle turn of the cochlea is reached, the burr is exchanged for a diamond burr, since at this level the amount of bone separating the drill from the internal carotid artery is very thin. Using the diamond burr and sufficient suction irrigation, drilling is continued to remove the remaining part of the cochlea and identify the vertical segment of the ICA.
31. The petrous apex is drilled as far as the level of the midclivus, exposing the dura of the posterior surface of the temporal bone. For extradural pathologies, removal of the disease is started after this step. On the other hand, if the pathology shows intradural extension, the dura is opened after bipolar coagulation.
Hints and Pitfalls
• Special care should be taken in the region of the geniculate ganglion. All bone should be removed here to avoid injury to the nerve during transposition.
• The vertical segment of the facial nerve has tough fibrous attachments to the fallopian canal, and sharp dissection is therefore needed to avoid stretching the nerve at this level. By contrast, the tympanic and labyrinthine segments are delicate and require fine manipulation.
• Failure to free the facial nerve up to the level of the stylomastoid foramen would leave the most distal part of its mastoid segment in situ. This part would obstruct complete control of the jugular bulb and preclude visualization of the lower pole of the tumor.
• While rerouting the facial nerve, cottonoids are used to protect it against direct suction. Brackmann suction tips can be used instead.
• This approach provides excellent control of the intrapetrous internal carotid artery, and the extent to which it should be exposed depends on the extent needed for tumor removal. The artery may be merely skeletonized, or can be exposed for 360° and 270° in its vertical and horizontal segments, respectively.
• The approach allows wide exposure of the cerebellopontine angle and prepontine cistern without cerebellar and brainstem retraction. It also makes it possible to remove the infiltrated dura and bone.
• Facial nerve rerouting leads to postoperative paralysis, which usually recovers to grade III.
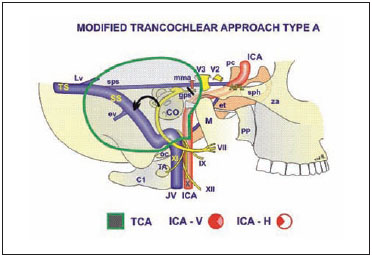
Fig. 8.1 The extent of bone removal and the structures controlled with the transcochlear approach. See Fig. 4.1, p. 57, for key to abbreviations.
Fig. 8.2 The skin incision is made as shown.

Fig. 8.3 In a left temporal bone, the mastoidectomy has been started and the mastoid antrum (A) has been identified. MFD Level of the middle fossa dura, SS Sigmoid sinus
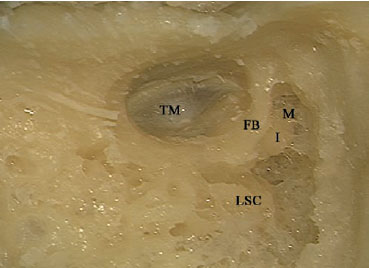
Fig. 8.4 The posterior and superior canal walls have been lowered down to the level of the annulus. FB Facial bridge, I Incus, LSC Lateral semi circular canal, M Malleus, TM Tympanic membrane
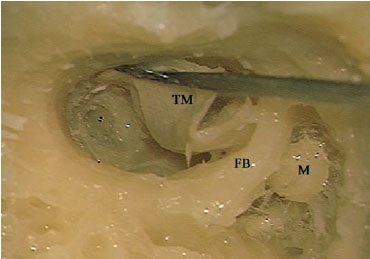
Fig. 8.5 Removal of the incus has been carried out. The tympanic membrane (TM) and malleus (M) are being removed. FB Facial bridge
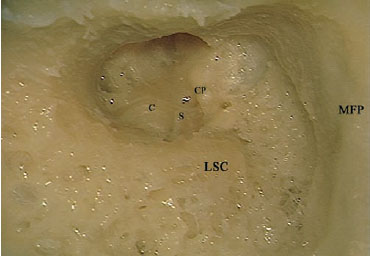
Fig. 8.6 The cavity after removal of the facial bridge. C Basal turn of the cochlea (promontory), CP Cochleariform process, LSC Lateral semicircular canal, MFP Middle fossa plate, S Stapes
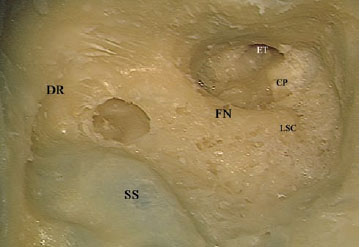
Fig. 8.7 The mastoid segment of the facial nerve (FN) has been identified. CP Cochleariform process, DR Digastric ridge, ET Eustachian tube, LSC Lateral semicircular canal, SS Sigmoid sinus
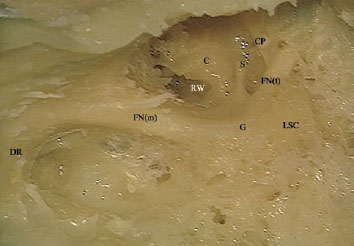
Fig. 8.8 Further reduction of the bony covering of the facial nerve has been carried out. C Basal turn of the cochlea (promontory), CP Cochleariform process, DR Digastric ridge, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, G Genu, LSC Lateral semicircular canal, RW Round window, S Stapes
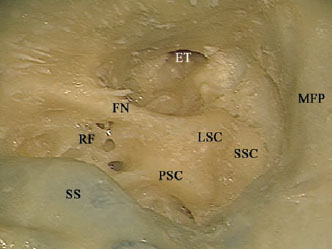
Fig. 8.9 The lateral semicircular canal (LSC), posterior semicircular canal (PSC), and superior semicircular canal (SSC) have been better identified. The retrofacial air cells (RF) are to be drilled away using a diamond burr to complete the skeletonization of the facial nerve (FN). ET Eustachian tube, MFP Middle fossa plate, SS Sigmoid sinus
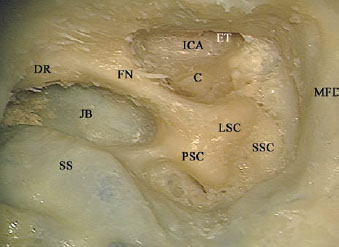
Fig. 8.10 The facial nerve (FN) has been well skeletonized, and the jugular bulb has been identified. The tympanic bone has been partially drilled away and the internal carotid artery (ICA) has been identified. C Basal turn of the cochlea (promontory), DR Digastric ridge, ET Eustachian tube, JB Jugular bulb, LSC Lateral semicircular canal, MFD Middle fossa dura, PSC Posterior semicircular canal, SS Sigmoid sinus, SSC Superior semicircular canal
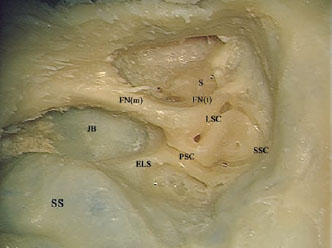
Fig. 8.11 The labyrinthectomy has been started. ELS Endolymphatic sac, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, JB Jugular bulb, LSC Lateral semicircular canal, PSC Posterior semicircular canal, S Stapes, SS Sigmoid sinus, SSC Superior semicircular canal
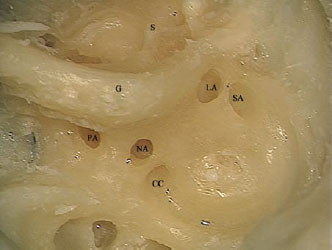
Fig. 8.12 Note the five openings into the vestibule. CC Common crus, G Genu of the facial nerve, LA Ampulla of the lateral canal, NA Nonampullated end of the lateral canal, PA Ampulla of the posterior canal, S Stapes, SA Ampulla of the superior canal
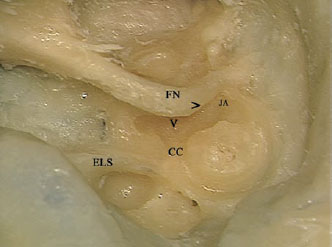
Fig. 8.13 The vestibule (V) has been opened. Note the thin amount of bone (>) separating the genu of the facial nerve (FN) from the vestibule. CC Common crus, ELS Endolymphatic sac, JA Joint lateral and superior ampullae
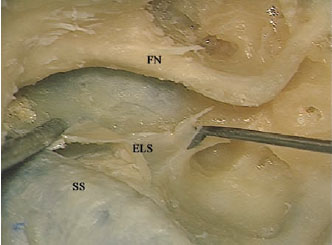
Fig. 8.14 The endolymphatic sac has been cut open and is being dissected away. ELS Endolymphatic sac, FN Facial nerve, SS Sigmoid sinus
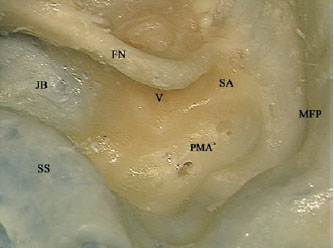
Fig. 8.15 Labyrinthectomy has been completed, and the internal auditory canal is to be identified next. FN Facial nerve, JB Jugular bulb, MFP Middle fossa plate, PMA Perimeatal air cells, SA Ampulla of the superior canal, SS Sigmoid sinus, V Vestibule
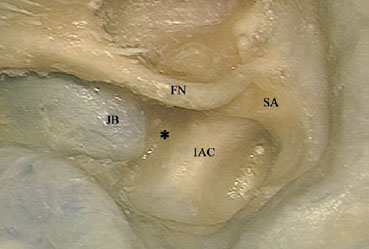
Fig. 8.16 The superior and posterior edges of the internal auditory canal (IAC) have been identified. The bone (*) between the canal and the jugular bulb (JB) is to be removed next. FN Facial nerve, SA Ampulla of the superior canal
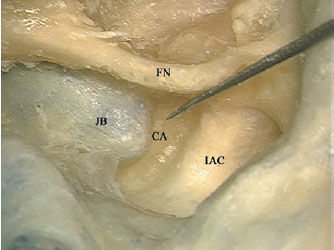
Fig. 8.17 The cochlear aqueduct (CA) has been identified. FN Facial nerve, IAC Internal auditory canal, JB Jugular bulb
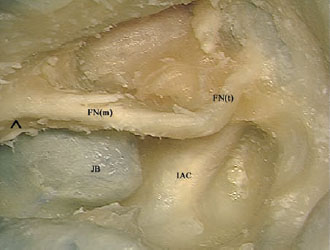
Fig. 8.18 Only a thin shell of bone is left covering the mastoid (FNm) and tympanic (FNt) segments of the facial nerve. The bone posterior to the facial nerve at the level of the digastric ridge (^) is to be further educed. IAC Internal auditory canal, JB Jugular bulb
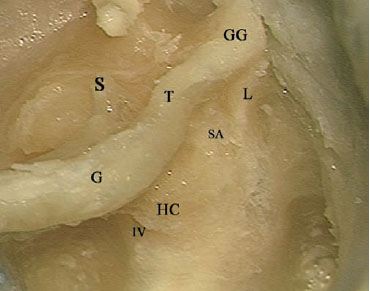
Fig. 8.19 The geniculate ganglion (GG) and labyrinthine segment (L) of the facial nerve have been identified. G Genu, HC Horizontal crest, IV Inferior vestibular nerve, S Stapes, SA Superior ampullary nerve, T Tympanic segment of the facial nerve
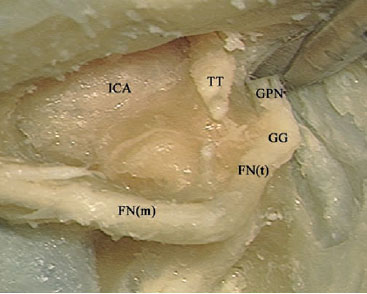
Fig. 8.20 After identification, the greater petrosal nerve (GPN) is now being cut. In live surgery, coagulation of this nerve should take place before it is cut. FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, ICA Internal carotid artery, TT Tensor tympani muscle
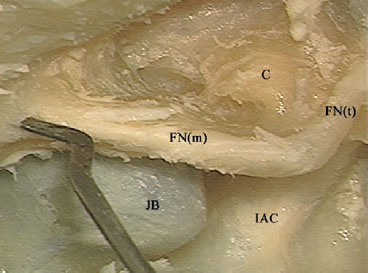
Fig. 8.21 The last shell of bone overlying the mastoid (FNm) and tympanic (FNt) segments of the facial nerve has been removed. The bone posterior to the facial nerve at the level of the digastric ridge is being removed to prevent injury to the nerve while it is being transposed. C Basal turn of the cochlea (promontory), IAC Internal auditory canal, JB Jugular bulb

Fig. 8.22 The superior ampullary nerve (SA) has been dislocated from its canal. FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, HC Horizontal crest, IAC Internal auditory canal, L Labyrinthine segment of the facial nerve
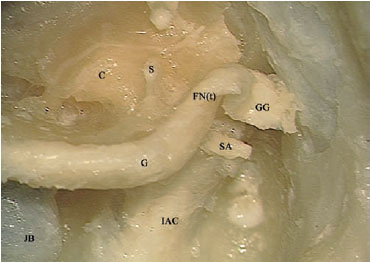
Fig. 8.23 Posterior rerouting of the facial nerve starts by the geniculate ganglion (GG). C Basal turn of the cochlea (promontory), FN(t) Tympanic segment of the facial nerve, IAC Internal auditory canal, JB Jugular bulb, S Stapes, SA Superior ampullary nerve
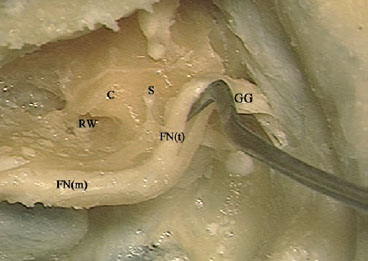
Fig. 8.24 The tympanic segment of the facial nerve FN(t) is being dissected from the canal. C Basal turn of the cochlea (promontory), FN(m) Mastoid segment of the facial nerve, GG Geniculate ganglion, RW Round window, S Stapes
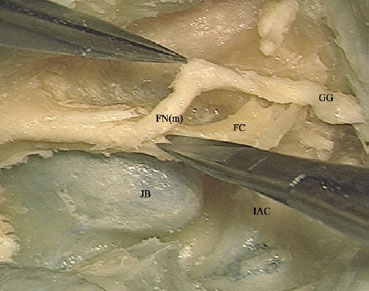
Fig. 8.25 Sharp cutting of the fibrovascular adhesions between the mastoid segment of the facial nerve (FNm) and the fallopian canal (FC). GG Geniculate ganglion, IAC Internal auditory canal, JB Jugular bulb
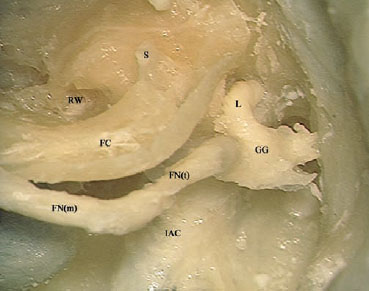
Fig. 8.26 The labyrinthine segment of the facial nerve (L) is being dissected from its canal. FC Fallopian canal, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, IAC Internal auditory canal, RW Round window, S Stapes
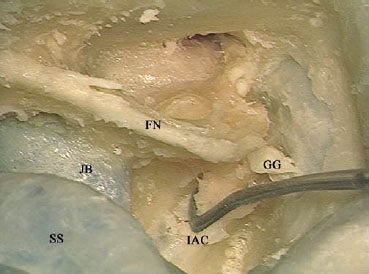
Fig. 8.27 Dislocating the inferior vestibular and cochlear nerves from the fundus. FN Facial nerve, GG Geniculate ganglion, IAC Internal auditory canal, JB Jugular bulb, SS Sigmoid sinus
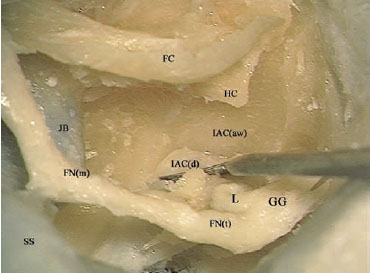
Fig. 8.28 The dura of the internal auditory canal (lACd) is being dissected from the anterior wall of the canal (IACaw). FC Fallopian canal, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, HC Horizontal crest, JB Jugular bulb, L Labyrinthine segment of the facial nerve, SS Sigmoid sinus
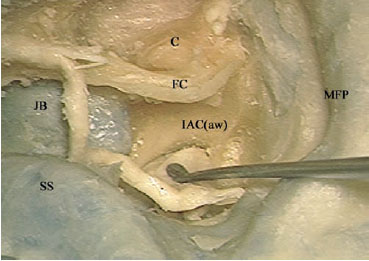
Fig. 8.29 The posteriorly rerouted facial nerve is placed between the jugular bulb (JB) and sigmoid sinus (SS). C Basal turn of the cochlea (promontory), FC Fallopian canal, IAC(aw) Anterior wall of the internal auditory canal, MFP Middle fossa plate
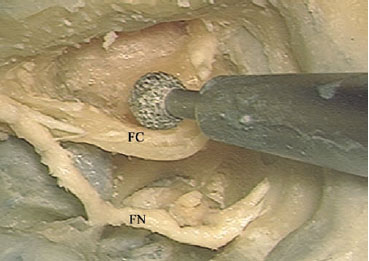
Fig. 8.30 A large diamond drill is used to remove the fallopian canal (FC). FN Facial nerve
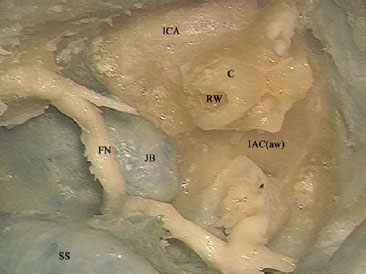
Fig. 8.31 The fallopian canal has been drilled away, and the cochlea (C)is to be removed next. FN Facial nerve, IAC(aw) Anterior wall of the internal auditory canal, ICA Internal carotid artery, JB Jugular bulb, RW Round window, SS Sigmoid sinus

Fig. 8.32 The cochlea has been drilled open, and the basal turn (BT) and middle turn (MT) can be seen. ICA Internal carotid artery, JB Jugular Bulb
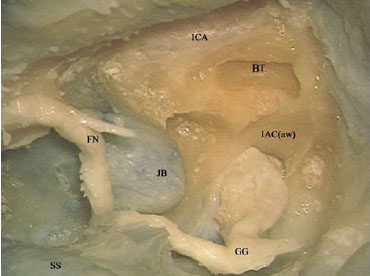
Fig. 8.33 Note the close relationship between the basal turn (BT) and the internal carotid artery (ICA). This part should be carefully removed using a small diamond burr. FN Facial nerve, GG Geniculate ganglion IAC(aw) Anterior wall of the internal auditory canal, JB Jugular bulb, SS Sigmoid sinus
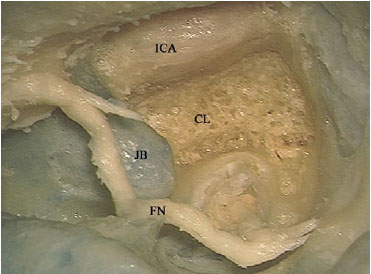
Fig. 8.34 The bone medial to the internal carotid artery (ICA) has been drilled and the clivus bone (CL) has been reached. FN Facial nerve, JB Jugular bulb
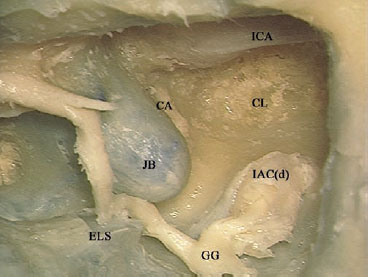
Fig. 8.35 The cochlear aqueduct (CA) can be seen in close relationship to the jugular bulb. CL Clivus, ELS Endolymphatic sac, GG Geniculate ganglion, IAC(d) Dura of the internal auditory canal, ICA Internal carotid artery, JB Jugular bulb
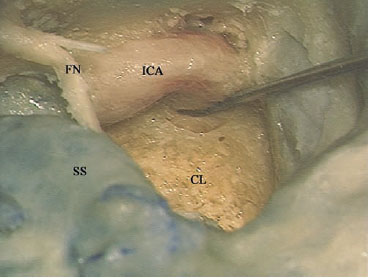
Fig. 8.36 For further drilling of the clivus bone (CL), the internal carotid artery (ICA) can be displaced laterally. FN Facial nerve, SS Sigmoid sinus
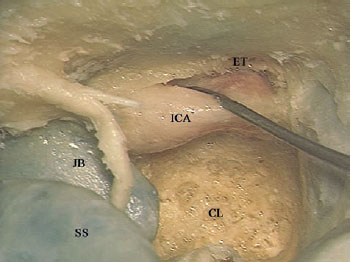
Fig. 8.37 If the bone lateral to the internal carotid artery (ICA) is to be removed, the artery can be displaced medially. CL Clivus, ET Eustachian tube, JB Jugular bulb, SS Sigmoid sinus
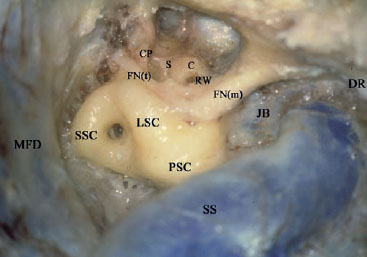
Fig. 8.38 The facial nerve of a right temporal bone has been identified from the stylomastoid foramen at the anterior border of the digastric ridge (DR) as far as the geniculate ganglion at the end of the tympanic segment of the nerve (FNt). C Cochlea, CP Cochleariform process, FN(m) Mastoid segment of the facial nerve, JB Jugular bulb, LSC Lateral semicircular canal, MFD Middle fossa dura, PSC Posterior semicircular canal, RW Round window, S Stapes, SS Sigmoid sinus, SSC Superior semicircular canal
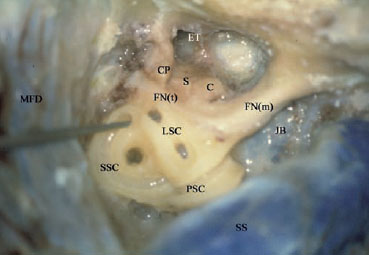
Fig. 8.39 The lateral (LSC), superior (SSC), and posterior (PSC) semicircular canals have been opened. The pointer has been introduced into the ampullae of the superior and lateral canals to show the relationship between these structures and the tympanic segment of the facial nerve (FNt). C Cochlea, CP Cochleariform process, ET Eustachian tube, FN(m) Mastoid segment of the facial nerve, JB Jugular bulb, MFD Middle fossa dura, S Stapes, SS Sigmoid sinus

Fig. 8.40 Skeletonization of the whole intratemporal course of the facial nerve has been accomplished. C Cochlea, FN Mastoid segment of the facial nerve, FN(l) Labyrinthine segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, IAC Internal auditory canal, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura, SS Sigmoid sinus
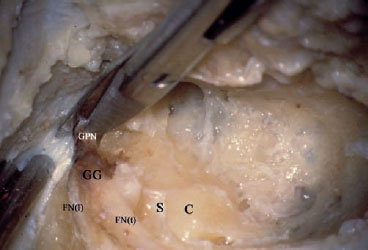
Fig. 8.41 The greater petrosal nerve (GPN) is being sharply cut following coagulation. C Cochlea, FN(l) Labyrinthine segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, S Stapes
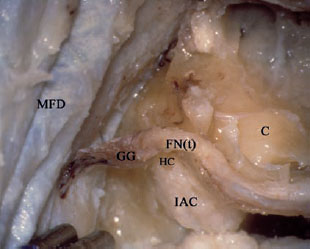
Fig. 8.42 Posterior rerouting is started by the rerouting of the geniculate ganglion (GG). C Cochlea, FN(t) Tympanic segment of the facial nerve, HC Horizontal crest, IAC Internal auditory canal, MFD Middle fossa dura
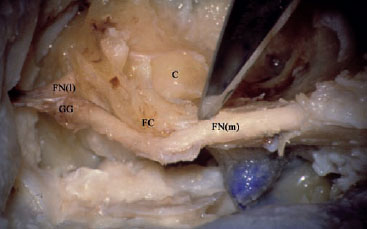
Fig. 8.43 The fibrovascular adhesions between the mastoid segment of the facial nerve (FNm) and the fallopian canal (FC) should be sharply cut. C Cochlea, FN(l) Labyrinthine segment of the facial nerve, GG Geniculate ganglion
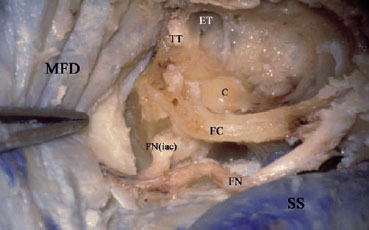
Fig. 8.44 Posterior rerouting of the facial nerve (FN) has been completed. C Cochlea, ET Eustachian tube, FC Fallopian canal, FN(iac) Internal auditory canal segment of the facial nerve, MFD Middle fossa dura, SS Sigmoid sinus, TT Tensor tympani
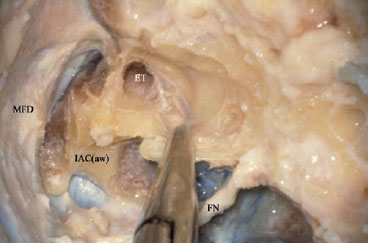
Fig. 8.45 A rongeur is used to remove the fallopian canal. ET Eustachian tube, FN Facial nerve, IAC(aw) Anterior wall of the internal auditory canal, MFD Middle fossa dura
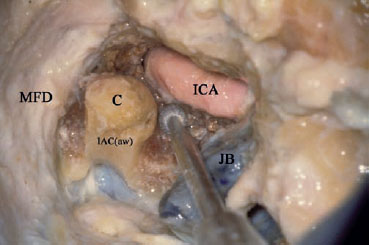
Fig. 8.46 A diamond drill of the appropriate size should be used for the drilling in the angle between the cochlea (C) and the internal carotid artery (ICA). IAC(aw) Anterior wall of the internal auditory canal, JB Jugular bulb, MFD Middle fossa dura
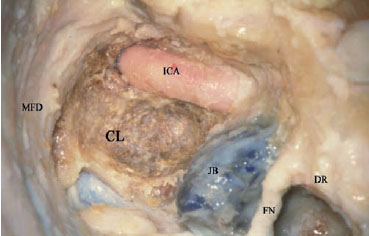
Fig. 8.47 The cochlea has been drilled out. CL Clivus, DR Digastric ridge, FN Facial nerve, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura
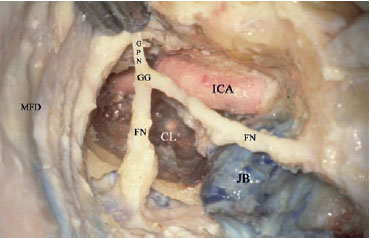
Fig. 8.48 The facial nerve (FN) has been returned into its original position, to compare the space provided by the approach before and after facial nerve rerouting. CL Clivus, GG Geniculate ganglion, GPN Greater petrosal nerve, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura
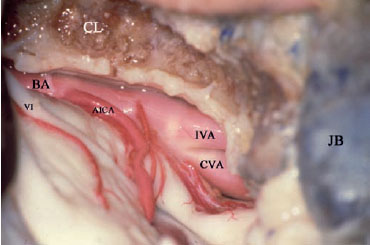
Fig. 8.49 The dura has been opened. Note the optimal control of the prepontine cistern provided by this approach. VI Abducent nerve, AICA Anterior inferior cerebellar artery, BA Basilar artery, CL Clivus, CVA Contralateral vertebral artery, IVA Ipsilateral vertebral artery, JB Jugular bulb
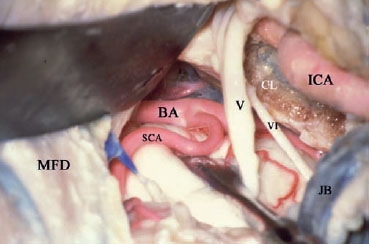
Fig. 8.50 In the upper part of the approach, the superior cerebellar artery (SCA) can be seen as it branches from the basilar artery (BA). V Trigeminal nerve, VI Abducent nerve, CL Clivus, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura
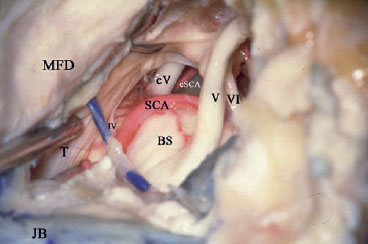
Fig. 8.51 The contralateral trigeminal nerve (cV) and contralateral superior cerebellar artery (cSCA), to indicate the excellent control of the prepontine cistern. IV Trochlear nerve, V Ipsilateral trigeminal nerve, VI Abducent nerve, BS Brainstem, JB Jugular bulb, MFD Middle fossa dura, SCA Ipsilateral superior cerebellar artery, T Tentorium
< div class='tao-gold-member'>



