9 Infratemporal Fossa Approaches
 Infratemporal Fossa Approach Type A (Figs. 9.1–9.31)
Infratemporal Fossa Approach Type A (Figs. 9.1–9.31)
Indications
• Lesions of the jugular foramen:
–Types C and D glomus jugulare tumors.
–Lower cranial nerve schwannomas and meningiomas of the jugular foramen. However, in the majority of these cases we resort to the petro-occipital transsigmoid approach, with preservation of the middle ear function and without transposing the facial nerve.
• Lesions of the infralabyrinthine and apical compartments of the temporal bone:
–Infralabyrinthine and some cases of apical cholesteatoma.
–Lower clivus chordomas.
Surgical Steps
1. After the craniotemporocervical skin incision has been made and after blind-sac closure of the external auditory canal, the main trunk of the facial nerve is identified at its exit from the temporal bone, using the perpendicular bisection of the line joining the cartilaginous pointer to the mastoid tip. The main trunk is traced in the parotid until the proximal parts of the temporal and zygomatic branches are identified.
2. The posterior belly of the digastric muscle and the sternocleidomastoid muscle are divided close to their origin. The internal jugular vein and the external and internal carotid arteries are identified in the neck and marked with umbilical tapes.
3. The remaining skin of the external auditory canal is removed along with the tympanic membrane, malleus, and incus.
4. A canal wall—down mastoidectomy is performed as described previously. The difference here is that the extent of bone removal should include the bone over, anterior to, and posterior to the sigmoid sinus and 2–3 cm of the bone covering the lateral aspect of middle cranial fossa.
5. The superstructure of the stapes is removed after its crura have been cut with straight microscissors. The aim of this step is to avoid touching the stapes with the rotating burr during tumor removal.
6. The facial nerve (FN) is skeletonized from the stylomastoid foramen to the geniculate ganglion. To avoid any injury to the FN while this delicate step is carried out, drilling should be carried out under high magnification using a large diamond burr moved in a direction parallel to the nerve. Ample irrigation during drilling provides adequate visualization and prevents thermal injury to the nerve. In live surgery, the facial nerve monitor is very useful.
7. A new fallopian canal is drilled in the root of the zygoma, superior to the eustachian tube.
8. The mastoid tip is amputated using a rongeur.
9. The last shell of the bone covering the nerve is carefully removed using a double-curved raspatory. We have found that leaving the pregeniculate portion of the facial nerve in place without rerouting it anteriorly helps preserve its blood supply and yields better FN results. Despite this, it is better to remove the bone covering of the GG to prevent sharp bone speckles remaining over the ganglion from injuring the anteriorly transposed nerve. When the live operation is carried out correctly, the facial nerve monitor should remain silent during the whole procedure.
10. Using sharp scissors, a tunnel is created in the tissues of the parotid gland.
11. The facial nerve is freed at the level of the stylomastoid foramen using strong scissors, leaving the soft tissue at this level attached to the nerve to protect it while transposition is being carried out.
12. The mastoid segment is elevated next. A Beaver knife is used to cut the fibrous attachments between the nerve and the bony canal at this level.
13. The tympanic segment of the nerve is elevated carefully short of the pregeniculate segment.
14. A nontoothed forceps is used to hold the soft tissue left attached to the nerve at the level of the stylomastoid foramen, and anterior rerouting is carried out.
15. A tunnel created in the parotid gland to accommodate the transposed nerve is sutured around the nerve.
16. The soft tissues surrounding the facial nerve at the level of the stylomastoid foramen are sutured to the soft tissues at the root of the zygoma, and in live surgery, fibrin glue is used to fix the nerve to the new bony canal created previously.
17. The muscles attached to the styloid process are sharply dissected, and the process is then cut with strong scissors or a rongeur.
18. Using a diamond burr, drilling of the infralabyrinthine cells is completed, and the vertical portion of the internal carotid artery is identified if the extent of the pathology requires this step.
19. The tympanic bone is drilled away, completing the exposure of the vertical portion of the internal carotid artery and the junction between the internal jugular vein and jugular bulb.
20. If further control is required over the genu and horizontal portion of the internal carotid artery (ICA), the mandibular condyle is separated from the anterior wall of the external auditory canal using a large septal raspatory. To keep the condyle displaced anteriorly, a self-retaining retractor is applied.
21. The proximal portion of the sigmoid sinus is closed by extraluminal packing with Surgicel.
22. The internal jugular vein is then double-ligated and cut.
23. The lateral wall of the sigmoid sinus is opened, and the cavity of the sinus is packed distally and proximally with two large pieces of Surgicel.
24. The internal jugular vein is then carefully dissected away, starting with the lower part. In cases in which the eleventh nerve passes lateral to the vein, the latter has to be pulled under the nerve to prevent it from being damaged.
25. If the medial wall of the bulb is not infiltrated by the tumor, it must be left covering cranial nerves IX and X, minimizing unnecessary surgical trauma to the nerves.
26. In live surgery, the tumor may be infiltrating the internal carotid artery; generally, the tumor invades only the periosteum rather than the carotid wall. Dissecting away this layer is therefore sufficient for adequate tumor removal. The plane of cleavage between the artery and the periosteum infiltrated by the tumor is best established at the level of the carotid foramen. The dense soft-tissue layer at the entrance of the artery into the carotid foramen is held using a nontoothed forceps and incised using a pair of curved scissors, with the tip directed away from the artery. The tumor is then dissected from the artery using a combination of sharp and blunt dissection.
27. If the tumor is found to be infiltrating the bone anterior to the internal carotid artery, the suction tube can be used to displace the artery laterally and medially to create the space for safe drilling of the infiltrated bone to achieve total tumor removal.
Hints and Pitfalls
• The facial nerve has to be freed in the parotid. This provides an extra length of free nerve and prevents the nerve from being stretched during anterior transposition.
• The facial nerve has to be properly uncovered. Bone at the level of the geniculate ganglion should be completely removed. Any sharp bone left over the nerve can lead to injury to the nerve during transposition.
• While the mastoid tip is being removed, care should be taken not to injure the facial nerve, which lies anteriorly. Using a rongeur, the mastoid tip is held firmly and is rotated posteriorly away from the nerve after the soft-tissue attachments at the anterior border of the tip have been sharply separated.
• During anterior rerouting of the facial nerve, a Beaver knife is used to cut the sharp attachments of the mastoid segment of the facial nerve.
• A soft-tissue cuff is left around the nerve at the level of the stylomastoid foramen. This tissue offers protection for the nerve during transposition.
• Direct suction over the facial nerve is avoided. A Brackmann suction tip is used instead. Cottonoids can also be used to avoid direct trauma from the suction tip.
• Bone medial to the internal carotid artery should be drilled. The haversian system of this bone is usually invaded by the tumor and is a frequent cause of recurrence.
• In about 50% of cases, the accessory nerve passes anterolateral to the internal jugular vein in the neck. After the vein has been ligated, care is taken not to injure the nerve when it is being elevated.
• We currently preserve the medial wall of the internal jugular vein and jugular bulb, which protect the closely related lower cranial nerves when not infiltrated by the tumor.
• Glomus tumors usually infiltrate the jugular bulb and penetrate the openings of the inferior petrosal sinus. Finger-like tumor projections of this type should be removed and bleeding can be controlled with Surgicel packing. However, overzealous packing should be avoided, as it may cause excessive swelling, with resultant paralysis of the intimately related lower cranial nerves due to compression.
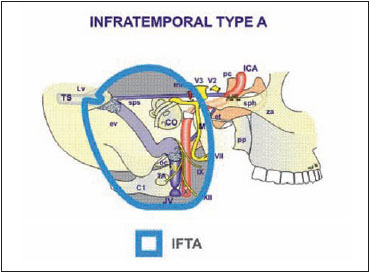
Fig. 9.1 The structures controlled by the infratemporal fossa approach type A. See Fig. 4.1, p. 57, for key to abbreviations.
Fig. 9.2 The skin incision is made as shown.
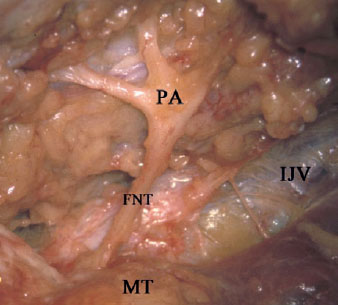
Fig. 9.3 A cadaveric dissection, showing the facial nerve trunk (FNT) as it exits the stylomastoid foramen and the start of the pes anserinus (PA). IJV Internal jugular vein, MT Mastoid tip
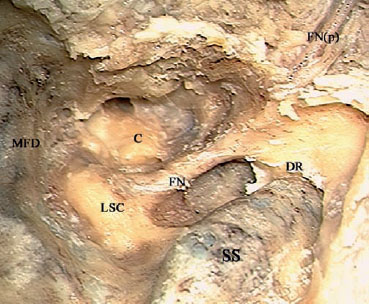
Fig. 9.4 In a right temporal bone, the intraparotid segment of the facial nerve (FNp) has been identified. An extended mastoidectomy has been carried out, removing the bony covering of the sigmoid sinus (SS) and revealing the posterior fossa and middle fossa dura (MFD). Skeletonization of the mastoid and tympanic segments of the facial nerve (FN) has been carried out. C Basal turn of the cochlea (promontory), DR Digastric ridge, LSC Lateral semicircular canal
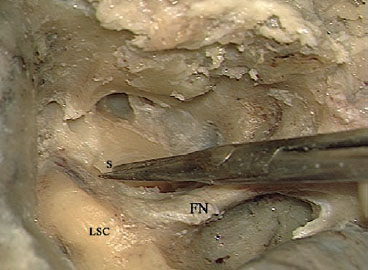
Fig. 9.5 The superstructure of the stapes (S) is being cut using straight scissors. FN Facial nerve, LSC Lateral semicircular canal
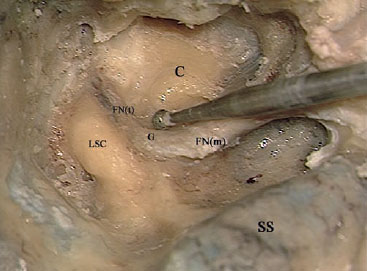
Fig. 9.6 Decompression of the nerve is being carried out. C Basal turn of the cochlea (promontory), FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, G Facial nerve genu, LSC Lateral semicircular canal, SS Sigmoid sinus
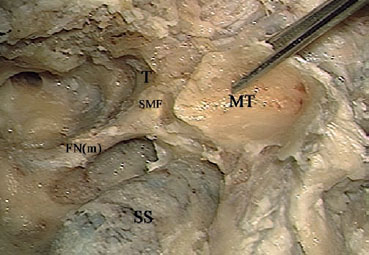
Fig. 9.7 The mastoid tip (MT) is being removed by avulsing it posteriorly away from the stylomastoid foramen (SMF), to avoid injuring the nerve at this level. FN(m) Mastoid segment of the facial nerve, SS Sigmoid sinus, T Tympanic bone
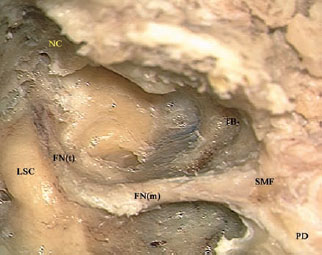
Fig. 9.8 The last shell of bone covering the mastoid (FNm) and tympanic (FNt) segments of the facial nerve is now ready to be removed. The new fallopian canal (NC) drilled into the root of the zygoma can be seen. LSC Lateral semicircular canal, PD Posterior belly of the digastric muscle, SMF Stylomastoid foramen, TB Tympanic bone
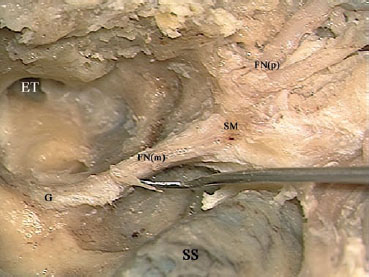
Fig. 9.9 The last shell of bone covering the mastoid segment of the facial nerve (FNm) is being removed. ET Eustachian tube, FN(p) Intraparotid facial nerve, G Genu, SM Stylomastoid foramen, SS Sigmoid sinus
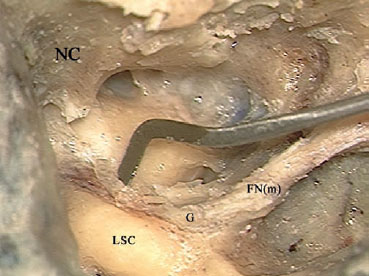
Fig. 9.10 The bony covering of the tympanic segment of the facial nerve is being removed. FN(m) Mastoid segment of the facial nerve, G Genu, LSC Lateral semicircular canal, NC New fallopian canal
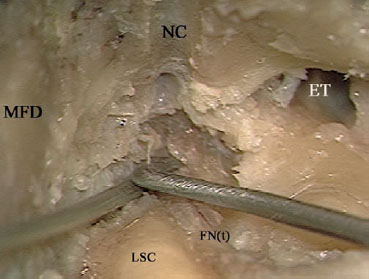
Fig. 9.11 The bone overlying the proximal part of the tympanic segment (FNt) and the geniculate ganglion is being removed, although the nerve is not to be rerouted at this level. The reason for removing bone here is to prevent it from injuring the rerouted part of the nerve. ET Eustachian tube, LSC Lateral semicircular canal, MFD Middle fossa dura, NC New fallopian canal
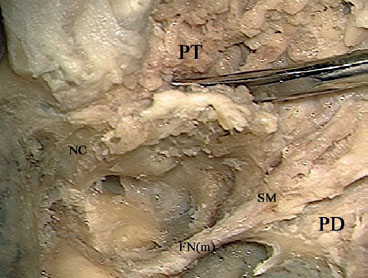
Fig. 9.12 A tunnel is being created in the soft tissues of the parotid gland (PT) to accommodate the distal part of the rerouted nerve. FN(m) Mastoid segment of the facial nerve, NC New canal, PD Posterior belly of the digastric muscle, SM Stylomastoid foramen
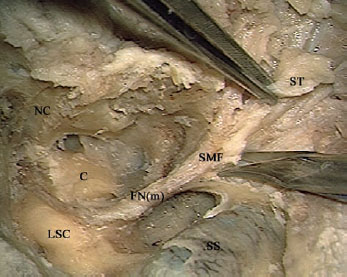
Fig. 9.13 A nontoothed forceps is used to hold the soft tissues (ST) surrounding the nerve at the level of the stylomastoid foramen (SMF), and sharp scissors are used to dissect the soft tissues from the bone at that level. C Cochlea, FN(m) Mastoid segment of the facial nerve, LSC Lateral semicircular canal, NC New canal, SS Sigmoid sinus

Fig. 9.14 The fibrovascular attachments (<) between the mastoid segment of the facial nerve (FNm) and the fallopian canal (FC) should be sharply cut.
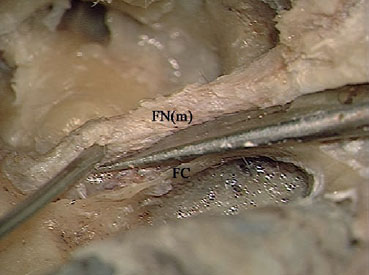
Fig. 9.15 The attachments shown in Fig. 9.14 are being sharply cut to avoid injuring the mastoid segment (FNm) of the nerve. FC Fallopian canal
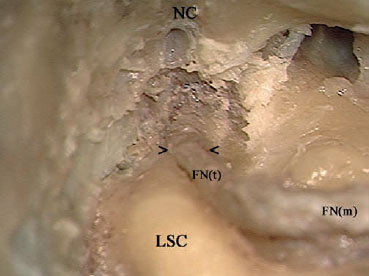
Fig. 9.16 The required length of the facial nerve has been dissected away from the fallopian canal; the arrows (> <) show the limit. Keeping this proximal part of the tympanic segment of the nerve (FNt) and the geniculate ganglion attached to the canal medially will help preserve part of the blood supply, resulting in better facial nerve function. FN(m) Mastoid segment of the facial nerve, LSC Lateral semicircular canal, NC New canal
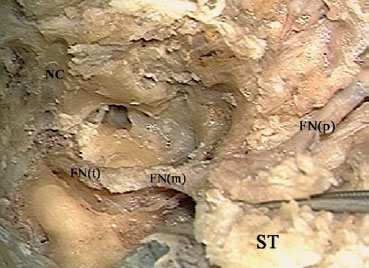
Fig. 9.17 In preparation for rerouting, the soft tissues (ST) surrounding the facial nerve at the stylomastoid foramen are being held by a non-toothed forceps. FN(m) Mastoid segment of the facial nerve, FN(p) Intraparotid facial nerve, FN(t) Tympanic segment of the facial nerve, NC New canal
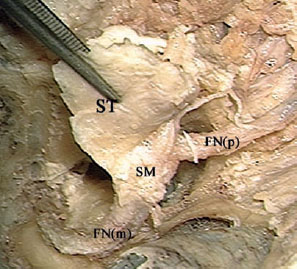
Fig. 9.18 Rerouting of the facial nerve. FN(m) Mastoid segment of the facial nerve, FN(p) Intraparotid facial nerve, SM Facial nerve at the stylomastoid level, ST Soft tissues
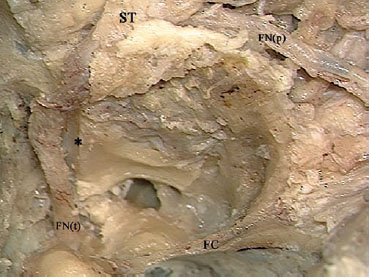
Fig. 9.19 The facial nerve has been rerouted into the new canal (*). FC Fallopian canal, FN(p) Rerouted part of the intratemporal facial nerve, FN(t) Rerouted part of the tympanic segment of the facial nerve, ST Soft tissues
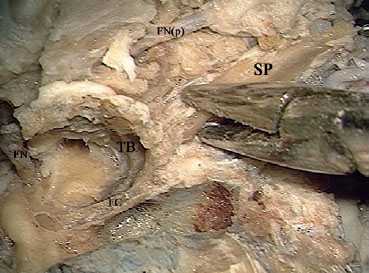
Fig. 9.20 After the attached muscles have been dissected away, the styloid process (SP) is fractured using a rongeur. FC Fallopian canal, FN Facial nerve, FN(p) Rerouted part of the intraparotid facial nerve, TB Temporal bone
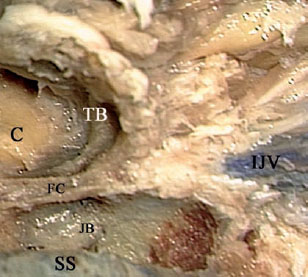
Fig. 9.21 To obtain control over the vascular structures as they enter the temporal bone, the tympanic bone (TB), the fallopian canal remnants (FC), and the infralabyrinthine air cells are all to be removed. C Basal turn of the cochlea (promontory), IJV Internal jugular vein, JB Jugular bulb, SS Sigmoid sinus
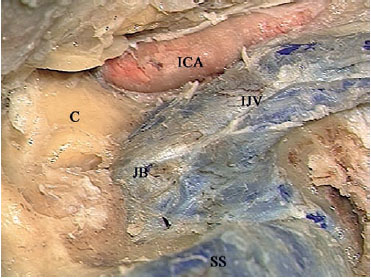
Fig. 9.22 The view after completely uncovering the lateral surfaces of the vascular structures. C Basal turn of the cochlea (promontory), ICA Internal carotid artery, IJV Internal jugular vein, JB Jugular bulb, SS Sigmoid sinus
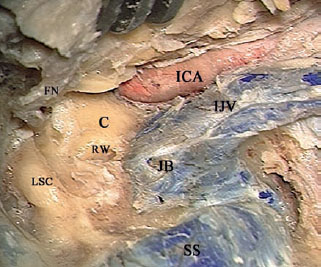
Fig. 9.23 If further anterior exposure of the internal carotid artery (ICA) is required, a retractor is used to keep the mandibular condyle displaced anteriorly. C Basal turn of the cochlea (promontory), FN Rerouted facial nerve, IJV Internal jugular vein, JB Jugular bulb, LSC Lateral semicircular canal, RW Round window, SS Sigmoid sinus
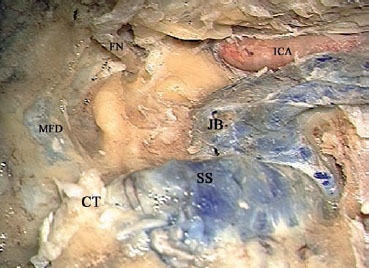
Fig. 9.24 The proximal end of the sigmoid sinus is closed by extraluminal packing of connective tissue (CT). FN Rerouted facial nerve, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura, SS Sigmoid sinus
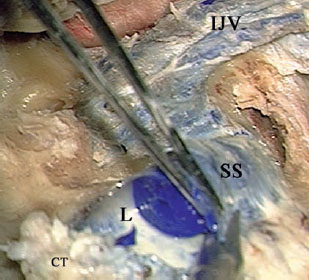
Fig. 9.25 The lateral wall of the sigmoid sinus (SS) has been opened. CT Connective tissue, IJV Internal jugular vein, L Lumen of the sigmoid sinus
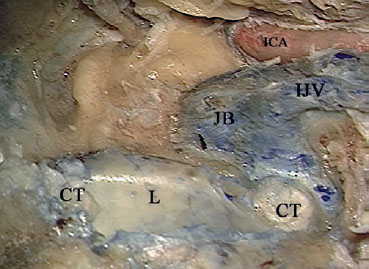
Fig. 9.26 The distal portion of the opened sigmoid sinus is packed with connective tissue (CT). ICA Internal carotid artery, IJV Internal jugular vein, JB Jugular bulb, L Lumen of the sigmoid sinus

Fig. 9.27 The internal jugular vein (IJV) is being dissected away. ICA Internal carotid artery, JB Jugular bulb
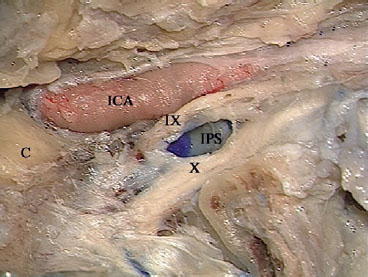
Fig. 9.28 The view after removal of the internal jugular vein and jugular bulb. Note that in live surgery, the opening of the inferior petrosal sinus (IPS) will start bleeding, requiring it to be packed. IX Hypoglossal nerve, X Vagus nerve, C Basal turn of the cochlea (promontory), ICA Internal carotid artery

Fig. 9.29 The plane of dissection between the internal carotid artery (ICA) and the overlying periosteum (P) is best developed at the entrance of the artery into its canal. C Basal turn of the cochlea (promontory)

Fig. 9.30 A suction tube is used to displace the internal carotid artery (ICA) laterally while the medially lying bone is being drilled. C Basal turn of the cochlea (promontory), IPS Inferior petrosal sinus
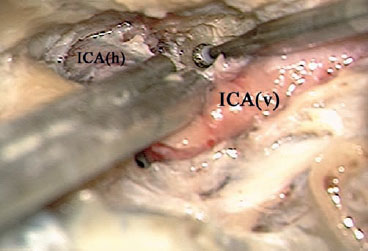
Fig. 9.31 The suction tube is used here both to displace the artery and to protect it during drilling of the anteriorly lying bone. ICA(h) horizontal segment of the internal carotid artery, ICA(v) vertical segment of the internal carotid artery
 Infratemporal Fossa Approach Type B (Figs. 9.32–9.63)
Infratemporal Fossa Approach Type B (Figs. 9.32–9.63)
Indications
• Petrous apex lesions, such as petrous bone cholesteatoma of the apical and infralabyrinthine types and cholesterol granuloma.
• Clival lesions, such as chordoma, chondrosarcoma, and extensive glomus tumors invading the clivus.
• Other rare lesions involving the infratemporal fossa, such as choristomas of the eustachian tube and giant-cell tumors of the petrous bone.
Surgical Steps
1. After the skin flap has been created and cul-de-sac closure of the external auditory canal skin has been carried out, the extratemporal facial nerve is exposed in the parotid, and the frontal branch of the nerve is followed until it crosses the zygomatic arch.
2. The temporalis muscle is detached from its bed and reflected anteriorly. The zygomatic arch is exposed, with care being taken not to injure the frontal branch of the facial nerve. The periosteum of the zygomatic arch is incised.
3. The arch is transected after two burr holes have been created for further refixation at the end of the procedure in live surgery.
4. The skin of the external auditory canal, the tympanic membrane, the malleus, and the incus are removed after disarticulation of the incudostapedial joint.
5. A subtotal petrosectomy is performed. The facial nerve is skeletonized and the inner ear is preserved.
6. The anterior wall of the external auditory canal is drilled. The vertical segment of the internal carotid artery is identified and skeletonized. The capsule of the temporomandibular joint is detached and cut using strong scissors. The articular disk is removed, exposing the mandibular condyle.
7. A small minicraniotomy is created, and a retractor is applied to displace the head of the mandible inferiorly.
8. The glenoid fossa is drilled. The sphenoid spine serves as a landmark for the middle meningeal artery. The artery is completely exposed, bipolarly coagulated, and cut.
9. With further drilling, the mandibular nerve is identified and cut after bipolar coagulation in live surgery.
10. The bony eustachian tube is drilled, and the horizontal carotid artery is further identified. Tumor removal follows next.
11. At the end of the procedure in live surgery, the eustachian tube is sutured, the zygomatic process is refixed into place, the temporalis muscle is used to obliterate the cavity, and the wound is closed in layers. A drain is inserted.
Hints and Pitfalls
• Exposure of the extratemporal portion of the facial nerve is useful in preventing overstretching of the nerve during the application of the infratemporal fossa retractor.
• The sphenoid spine serves as a landmark for the middle meningeal artery, which lies immediately anterior to it.
• Before the mandibular nerve is transacted in live surgery, bipolar coagulation helps reduce bleeding from the venus plexus surrounding the nerve.
• Drilling should always be parallel to the course of the internal carotid artery in order to reduce the risk of tearing the artery wall.
• Bleeding from the veins within the carotid sheath may easily be controlled by Surgicel packing.
• Bleeding from the inferior petrosal sinus can be controlled by intraluminal packing.
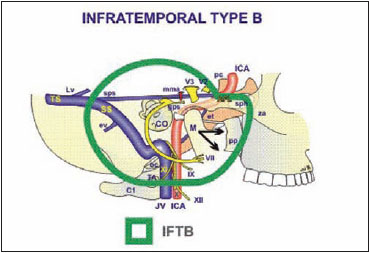
Fig. 9.32 The structures controlled by the type B infratemporal fossa approach. See Fig. 4.1, p. 57, for key to abbreviations.
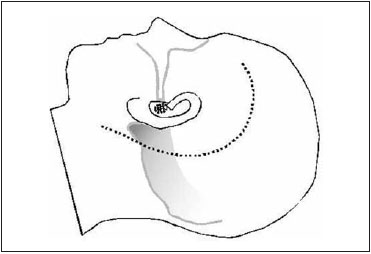
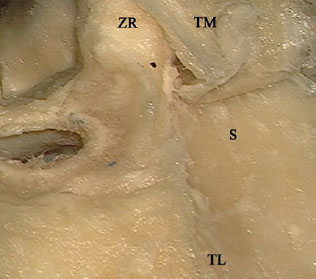
Fig. 9.34 The temporalis muscle (TM ) of a left temporal bone has been reflected anteriorly after it has been dissected from the squamous bone (S). TL Temporalis line, ZR Root of the zygomatic process
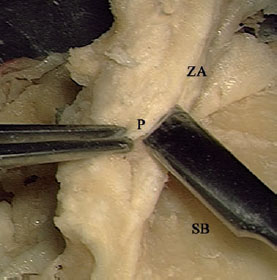
Fig. 9.35 The periosteum (P) overlying the zygomatic arch (ZA) is being dissected away. This step helps avoid the laterally lying frontal branch of the facial nerve. SB Squamous bone
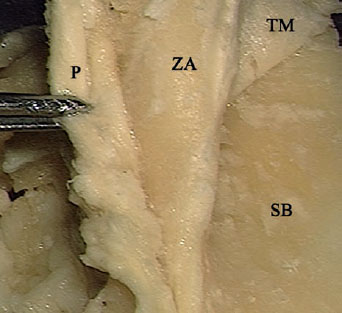
Fig. 9.36 The view after dissection of the periosteum (P) from the zygomatic arch (ZA). SB Squamous bone, TM Temporalis muscle
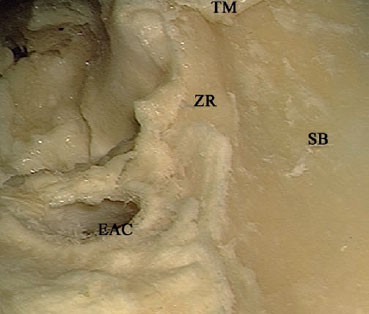
Fig. 9.37 The zygomatic arch has been transected. EAC External auditory canal, SB Squamous bone, TM Temporalis muscle, ZR Zygomatic root
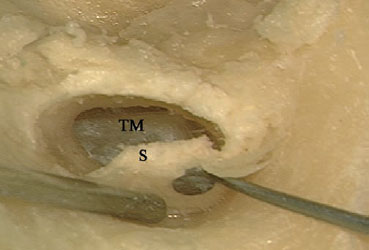
Fig. 9.38 The skin of the external auditory canal (S) is being dissected away under the microscope. TM Tympanic membrane
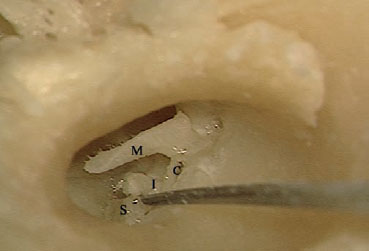
Fig. 9.39 After complete removal of the external auditory canal skin and tympanic membrane, the incudostapedial joint is disarticulated in order to remove the ossicular chain. C Chorda tympani, I Incus, M Malleus, S Stapes

Fig. 9.40 The mastoid cavity and the posterior and superior walls of the external auditory canal have been partially drilled. FB Facial bridge, FR Facial ridge, MFP Middle fossa plate, SS Sigmoid sinus
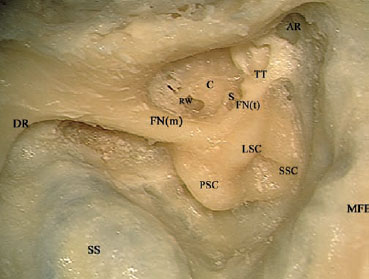
Fig. 9.41 A radical mastoidectomy has been carried out, and the facial nerve has been skeletonized. AR Anterior attic recess, C Basal turn of the cochlea (promontory), DR Digastric ridge, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, LSC Lateral semicircular canal, MFP Middle fossa plate, PSC Posterior semicircular canal, RW Round window, S Stapes, SS Sigmoid sinus, SSC Superior semicircular canal, TT Tensor tympani
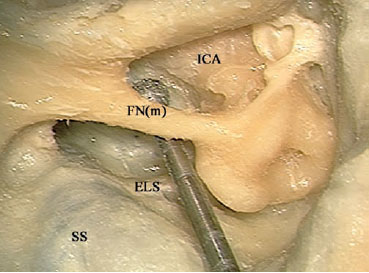
Fig. 9.42 The retrofacial and infralabyrinthine air cells are being drilled using an appropriately sized diamond drill. Attention must be paid during this step to avoid injuring the laterally lying facial nerve with the burr or the shaft. ELS Endolymphatic sac, FN(m) Mastoid segment of the facial nerve, ICA Internal carotid artery, SS Sigmoid sinus
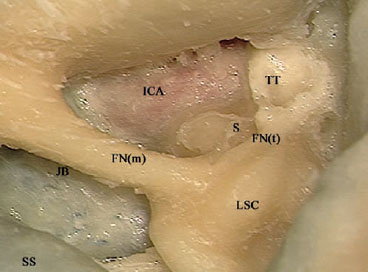
Fig. 9.43 The anterior wall of the external auditory canal has been partially drilled, and the vertical segment of the internal carotid artery (ICA) has been identified. FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, JB Jugular bulb, LSC Lateral semicircular canal, S Stapes, SS Sigmoid sinus, TT Tensor tympani
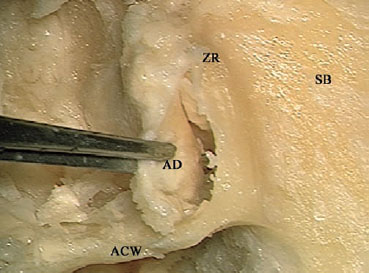
Fig. 9.44 Dissecting the articular disk (AD) of the temporomandibular joint. ACW Anterior canal wall, SB Squamous bone, ZR Zygomatic root
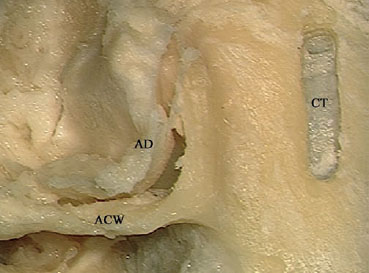
Fig. 9.45 A small craniotomy (CT) has been created in the squamous bone. ACW Anterior canal wall, AD Articular disk
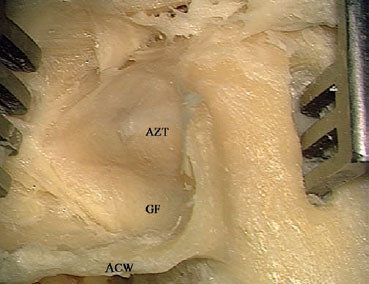
Fig. 9.46 A self-retaining retractor is used to keep the mandible retracted inferiorly. ACW Anterior canal wall, AZT Anterior zygomatic tubercle, GF Glenoid fossa
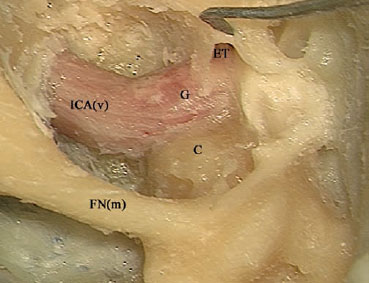
Fig. 9.47 The rest of the anterior canal wall has been drilled away, and the internal carotid artery is better skeletonized. C Basal turn of the cochlea (promontory), ET Eustachian tube, FN(m) Mastoid segment of the facial nerve. G Genu of the internal carotid artery, ICA(v) Vertical segment of the internal carotid artery
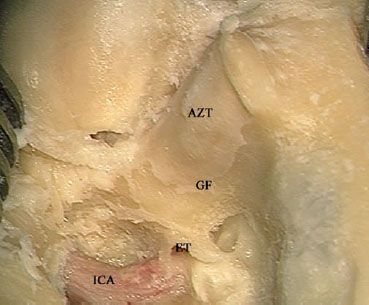
Fig. 9.48 To obtain control of the horizontal segment of the internal carotid artery, the eustachian tube (ET), glenoid fossa bone (GF), and the anterior zygomatic tubercle (AZT) have to be carefully drilled away. ICA Vertical segment of the internal carotid artery
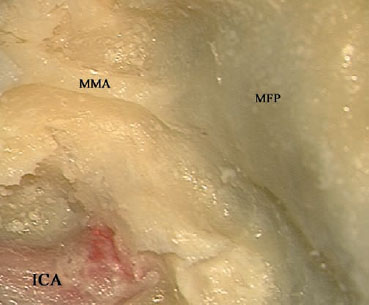
Fig. 9.49 In live surgery, the middle meningeal artery (MMA) should be coagulated to prevent bleeding. ICA Internal carotid artery, MFP Middle fossa plate
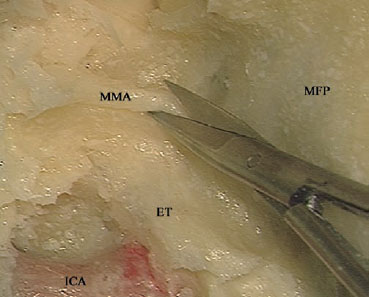
Fig. 9.50 The middle meningeal artery (MMA) is being sharply cut. ET Eustachian tube, ICA Internal carotid artery, MFP Middle fossa plate
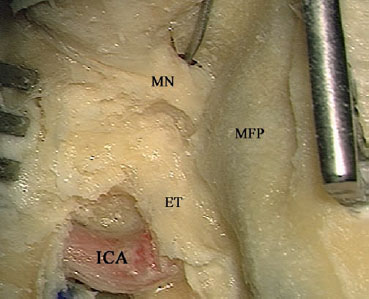
Fig. 9.51 Further anterior drilling uncovers the mandibular nerve (MN). This nerve also has to be coagulated in live surgery before it is cut. ET Eustachian tube, ICA Internal carotid artery, MFP Middle fossa plate
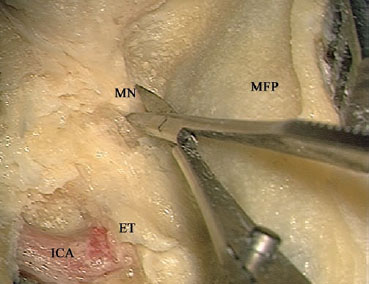
Fig. 9.52 Sharply cutting the mandibular nerve (MN). ET Eustachian tube, ICA Internal carotid artery, MFP Middle fossa plate
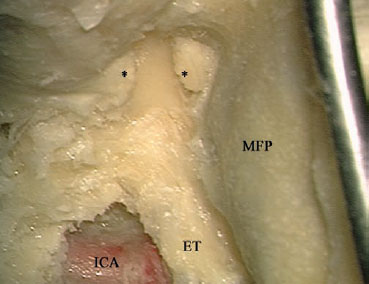
Fig. 9.53 The stumps of the mandibular nerve (*). ET Eustachian tube, ICA Internal carotid artery, MFP Middle fossa plate
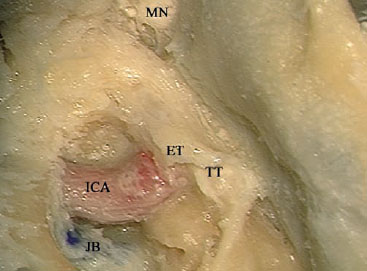
Fig. 9.54 The eustachian tube (ET) and tensor tympani muscles (TT) are the last structures lying lateral to the horizontal segment of the facial nerve and should be removed. ICA Internal carotid artery, JB Jugular bulb, MN The cut end of the mandibular nerve
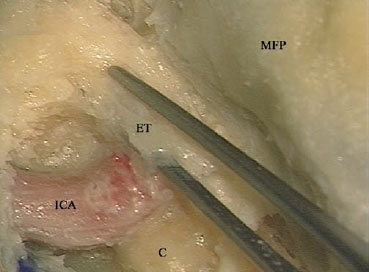
Fig. 9.55 The lateral, thin part of the eustachian tube (ET) that remains can be removed with forceps. C Basal turn of the cochlea (promontory), ICA Internal carotid artery, MFP Middle fossa plate

Fig. 9.56 The tensor tympani muscle has been dissected away from its canal (TTC). ET Medial wall of the eustachian tube, ICA Internal carotid artery, MFP Middle fossa plate
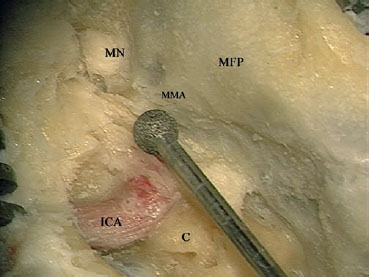
Fig. 9.57 A large diamond burr is used to remove the remaining bone overlying the horizontal segment of the internal carotid artery. C Basal turn of the cochlea (promontory), ICA Vertical segment of the internal carotid artery, MFP Middle fossa plate, MMA Stump of the middle meningeal artery, MN Stump of the mandibular nerve
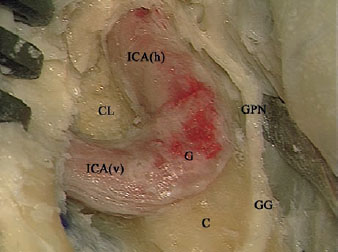
Fig. 9.58 The horizontal segment of the internal carotid artery (ICAh) has been skeletonized. Note that the greater petrosal nerve (CPN) is adherent to the dura, and that retracting the dura will lead to stress on the facial nerve at the geniculate ganglion (GG) level. Thus, if dural retraction is needed, cutting the petrosal nerve will prevent this injury. C Basal turn of the cochlea (promontory), CL Clivus bone, G Genu, ICA(v) Vertical segment of the internal carotid artery
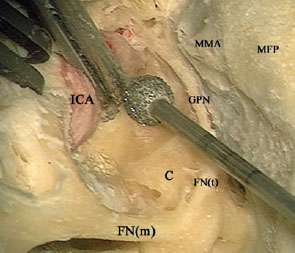
Fig. 9.59 The tip of the suction is used to displace the internal carotid artery (ICA) laterally while the medially lying bone is being drilled. C Basal turn of the cochlea (promontory), FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GPN Greater petrosal nerve, MFP Middle fossa plate, MMA middle meningeal artery stump
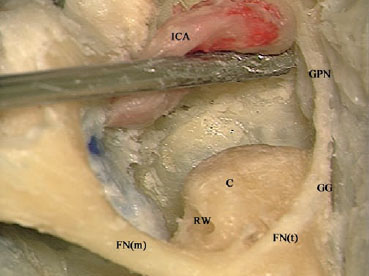
Fig. 9.60 Drilling of the clivus has been completed. C Basal turn of the cochlea (promontory), FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, GPN Greater petrosal nerve, ICA Internal carotid artery, RW Round window
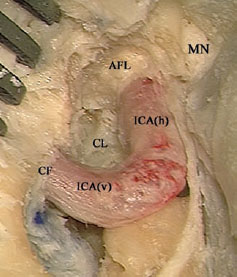
Fig. 9.61 The full course of the intratemporal internal carotid artery has been freed. AFL Anterior foramen lacerum, CF Carotid foramen, CL Dura overlying the clivus area, ICA(h) Horizontal segment of the internal carotid artery, ICA(v) Vertical segment of the internal carotid artery, MN Stump of the mandibular nerve

Fig. 9.62 The view after completion of the approach.
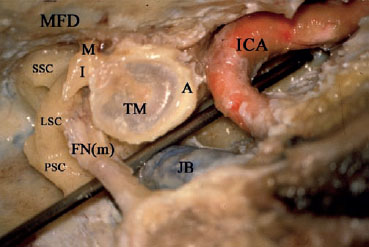
Fig. 9.63 The relationship of the internal carotid artery (ICA) to the tympanic membrane (TM) and middle ear in a right temporal bone. A Annulus, FN(m) Mastoid segment of the facial nerve, I Incus, JB Jugular bulb, LSC Lateral semicircular canal, M Malleus, MFD Middle fossa dura, PSC Posterior semicircular canal, SSC Superior semicircular canal
< div class='tao-gold-member'>



