Figure 34.1 The four quadrants of the right orbit. The surgical approach is chosen by the quadrant of the orbit that is most involved by the underlying pathology. The superior quadrant is accessed by the SLC approach (see Chapter 15); the medial quadrant is entered through a PC incision; the inferior quadrant approach is made through an ITC incision; and the lateral quadrant is reached through an LRC portal. (SLC, superior lid crease; PC, precaruncular; ITC, inferior transconjunctival; LRC, lateral retrocanthal.)
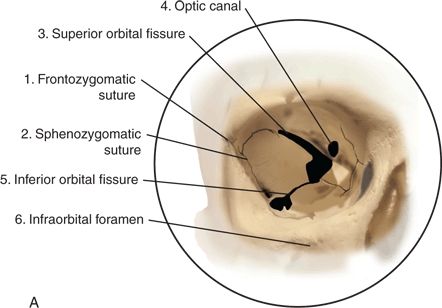
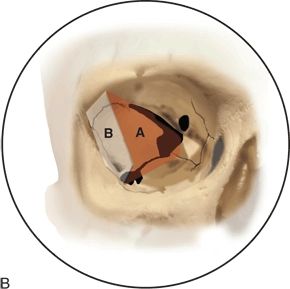
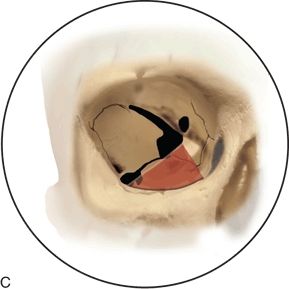

FIGURE 34.2 A. Surgical anatomy of the right orbit. 1, frontozygomatic suture; 2, sphenozygomatic suture; 3, superior orbital fissure; 4, optic canal; 5, inferior orbital fissure; 6, foramen of infraorbital nerve. B. Outline of bone removed through lateral orbitotomy: A, approach to MCF through greater wing of sphenoid bone; B, approach to infratemporal fossa. C. Region of approach through inferior orbitotomy. (MCF, middle cranial fossa.)Figure 34.2(Continued ) D. Arrow on foramen rotundum seen through inferior orbital fissure.
The choice of pathway and number of portals is made with a preoperative computerized approach analysis using a surgical navigation system and includes a full 360-degree evaluation of the anatomy involved in and adjacent to the pathology, as well as the anatomic structures that are displaced or traversed by the potential endoscopic pathways to the target. The pathway(s) are chosen to provide the most efficacious and least morbid approach. The goal of surgery is to achieve the best possible angle(s) for the endoscopic treatment of the pathology and ultimately to lessen the morbidity by avoiding an open cranial microsurgical approach (Fig. 34.3).
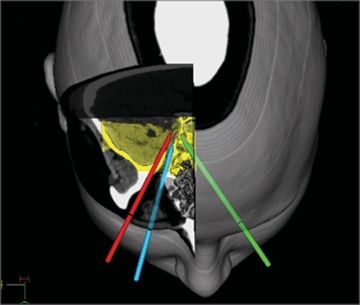
Figure 34.3 Example of preoperative computer analysis of possible endoscopic pathways to right cavernous sinus, superior view, CT scan. Lateral (red), inferior (blue) contralateral PC (green) approaches. MCF and adjacent sphenoethmoid regions are highlighted in yellow. (PC, precaruncular; MCF, middle cranial fossa.)
While the LRC approach provides retro-orbital access to regions of the MCF that cannot be safely achieved transnasally, the ITC and CPC portals provide access that can also be obtained through transnasal or transmaxillary approaches. The angles of approach that they provide to a target are quite different; the distances may be significantly shorter than transnasal approaches, and as such, the portals can be complementary. At times, however, pathology may involve the floor of the orbit (e.g., metastatic tumor) or a portion of the orbit that would be resected with the pathology. In these situations, a transorbital portal can provide a clearly advantageous surgical visualization of the orbit, particularly if orbital reconstruction will be required. As experience with all of these approaches grows, the indications and contraindications to the use of each portal will be further delineated.
This chapter provides a discussion of the transorbital endoscopic approaches that we use for access to the MCF, including the LRC, ITC, and CPC portals. Though our approach for sellar and parasellar pathology is most commonly performed through transnasal portals, a description of these is beyond the scope of this discussion.
HISTORY
The presentation and history of patients with MCF lesions are highly variable, depending on the location, type, and stage of the underlying pathology. Tumors in this region are often silent until they invade and travel along nerves, at which time they may cause facial numbness or pain. Progression within the brain may cause symptoms depending on the region involved. Tumor involvement in the infratemporal or pterygopalatine fossae may cause interference or pain with mastication. Spread anteriorly with the orbit may cause diplopia, proptosis, and progressive loss of vision.
PHYSICAL EXAMINATION
Any patient presenting with symptoms consistent with pathology involving the MCF should have a complete examination of the head and neck, as well as a thorough neurologic evaluation including all of the cranial nerves. Evaluation of facial sensation in all branches of the trigeminal nerves is important. Nasal and pharyngeal endoscopy should be performed to evaluate involvement of the medial orbit, interorbital skull base and, sphenoid and clival regions.
Imaging is then performed based on the history and physical examination, with computerized tomographic (CT) scans and magnetic resonance imaging (MRI) being the most frequently indicated studies alone or as complementary evaluations. Angiography may be indicated for examination of vascular involvement or for preoperative embolization to make surgery safer.
INDICATIONS
A wide range of pathology can involve the MCF as a primary site, through metastasis from a distant site, or through local extension from an adjacent structure. Tumors arising within the MCF are usually benign and include pituitary adenoma, meningioma, and trigeminal schwannoma. (Temporal bone pathology is excluded from this chapter.) Malignancies arising in this area include chordoma, chondrosarcoma, and osteosarcoma; perineural invasion from squamous cell carcinoma or adenoid cystic carcinoma. Local invasion and hematologic metastases are also common.
The most common open procedures to access these regions are the pterional, orbitopterional, orbitozygomatic, and transzygomatic/infratemporal fossa approaches. The open microvascular procedures, although effective, can be morbid due to brain retraction, cerebral edema, and disruption of normal structures associated with large, potentially visible scars. Furthermore, open procedures through the frontotemporal regions require displacement of the temporalis muscle that may cause significant visible hollowing of the temporal contour. In addition, the frontal branch of the facial nerve is at risk for injury during the creation of these surgical pathways. Though paralysis of this nerve is not common, when it does occur, it has a significant negative impact on a patient’s appearance and may cause blockage of the superior visual field. Removal of a large cranial bone flap also carries the risk of infection of the flap and added recovery time for the patient.
For reasons of safety, better visualization of the pathology and improved healing time, transnasal endoscopic approaches have been described and investigated for access to the parasellar regions, petrous apex, and medial aspect of the cavernous sinus. These approaches offer excellent access through a natural corridor. There are times, however, when an additional access portal to these regions may be beneficial to improve the angles of visualization of the pathology or to provide increased working space between the surgeons’ hands or instruments.
Transnasal approaches may also be limited in their ability to provide visualization and endoscopic access to the lateral aspect of the cavernous sinus/parasellar regions and locations lateral to the trigeminal ganglion, and when these regions can be reached, this endoscopic route may be at the upper limits of their effective range.
Another region of limited access transnasally is the superior infratemporal fossa and the anterior–superior MCF. These regions are within the orbital “shadow effect” of a transnasal approach, making these areas challenging to access without endangering critical neurovascular structures.
Transorbital approaches can be used to access these areas that are either difficult or dangerous to reach through the nose or to provide multiportal corridors in addition to transnasal approaches. The indications for these approaches are similar to those for transnasal portals and are expanding with growing familiarity of the anatomic perspectives and technical demands. Transorbital endoscopic approaches to the MCF are currently indicated for benign and localized malignancies involving the ventral aspects of the MCF along the inferior, medial, lateral, and anterior borders. The primary transorbital approaches to these regions are the LRC, ITC, and the CPC portals as described above.
The indications and applications of these approaches are continuing to expand and will likely further develop as advanced instrumentation becomes available. The lateral orbitotomy (LRC approach) provides access to the infratemporal fossa, the greater wing of the sphenoid, and adjacent regions of the MCF. Its applications include trauma and CSF leak repair, and resection of tumors. This pathway can be used for access to the lateral aspect of the cavernous sinus and trigeminal ganglion, with a relatively short intracranial component (Fig. 34.4). There is considerable flexibility in the placement of the entry portal in the coronal plane, and the choice of entry is made by vector analysis with regard to the surgical target.
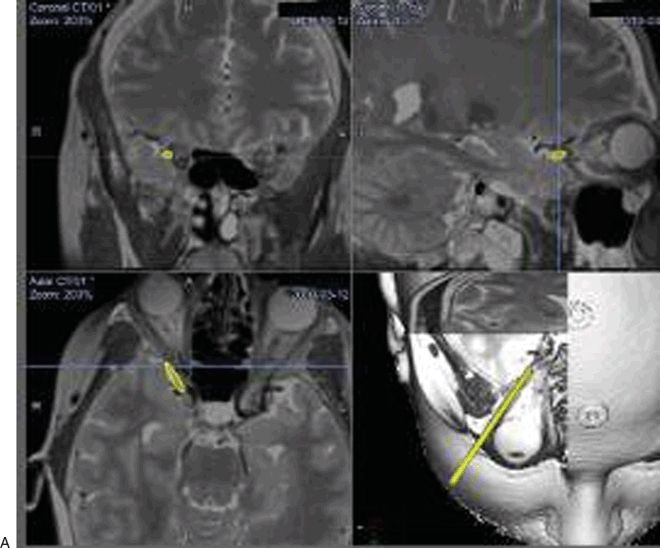
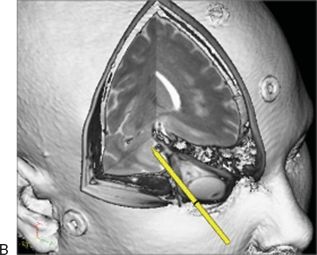
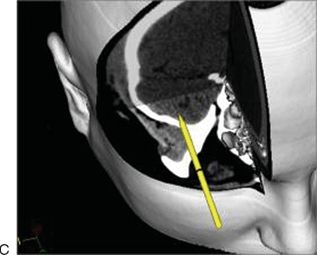
FIGURE 33.4 A. Surgical planning view, LRC approach. B. Enlargement demonstrating trajectory of LRC approach. C. Access to lateral MCF. Note proximity of infratemporal fossa that can easily be entered as needed. (LRC, lateral retrocanthal; MCF, middle cranial fossa.)
The ITC approach can be used for targets at the inferior anterior aspect of the MCF, such as the region of the foramen rotundum (Fig. 34.5). It also offers a potential pathway to the inferior lateral aspect of the cavernous sinus following a trajectory inferior to the optic nerve. This approach is particularly useful for pathology that involves the inferior orbit and maxilla, such as tumors in the infraorbital nerve.
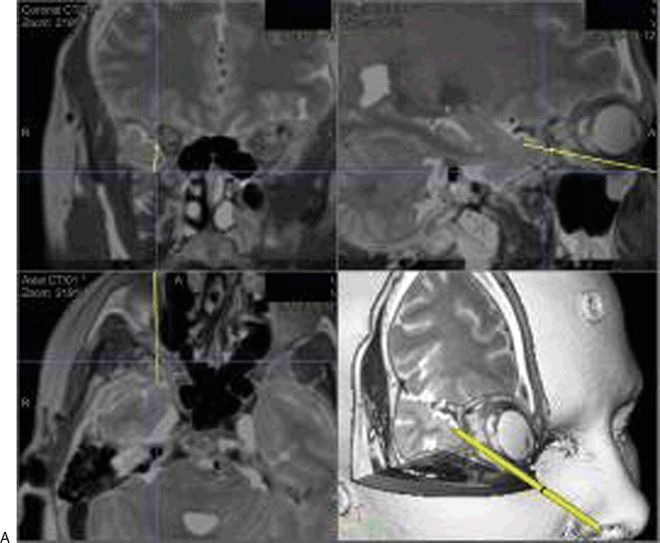
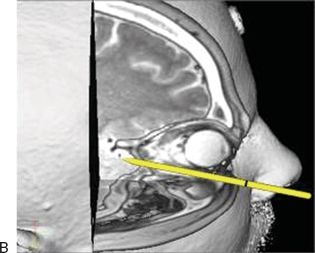
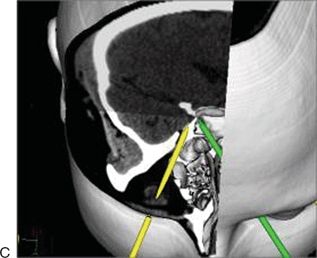
Figure 34.5 ITC approach. A. Preoperative pathway analysis with vector from entry portal to the surgical target. B. Enlarged parasagittal view demonstrating pathway inferior to the globe, leaving the orbit posteriorly, where the orbital floor rises, to enter the MCF. C. ITC approach to foramen rotundum with CPC approach (green) to lateral sphenoid. (ITC, inferior transconjunctival; MCF, middle cranial fossa; CPC, contralateral precaruncular.)
The CPC approach is indicated for pathology in the medial aspect of the cavernous sinus, optic nerve, and selected sellar and suprasellar lesions (Fig. 34.6). Pathology of the optic nerve and chiasm as well as the resection of encephaloceles are strong indications for inclusion of this portal in the surgical plan.
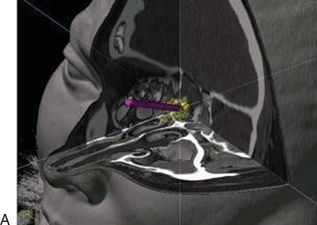
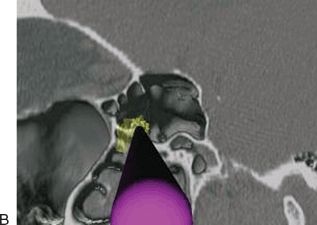
FIGURE 34.6 A. Left CPC approach to right MCF (Sternberg’s) encephalocele (yellow). B. Magnified segment of (A), with virtual endoscopy demonstrating favorable approach for viewing and instrumentation. (CPC, contralateral precaruncular; MCF, middle cranial fossa.)
CONTRAINDICATIONS
As for the transorbital approaches to the ACF (see Chapter 16), the primary contraindication to transorbital approaches to the MCF appears to be a recent history of severe orbital trauma. A history of LASIK surgery, though not a contraindication to surgery, should caution the surgeon to treat the cornea with great care and follow the patient closely postoperatively for any corneal complications (see Complications section). These patients may have partial corneal anesthesia and may be at higher risk for corneal ulceration or exposure damage. Patients with primary orbital pathology, particularly those with corneal anesthesia, should be evaluated preoperatively by an ophthalmologist and receive joint follow-up postoperatively.
The pathology must be of a suitable extent, location, and character for resection with endoscopic visualization and the instrumentation at the surgeon’s disposal. Care should be taken to ensure that the lesion is a solitary lesion in cases of metastatic disease.
Surgeons should receive adequate training and/or mentoring in these approaches before using them clinically. Each patient’s pathology should be evaluated individually with preoperative CT and MRI analysis to be certain that an endoscopic approach of any type is appropriate and to determine which type of monoportal or multiportal surgical approach will be optimal.
PREOPERATIVE PLANNING
As for any complex surgical procedure, transorbital endoscopic approaches to the MCF should be considered only after comprehensive evaluation of the patient including comprehensive imaging and consultation with all of the members of the skull base team who will be involved. When possible, it is optimal for the patients to be seen by the treating physicians synchronously to provide a comprehensive evaluation. Tumor cases should be presented and discussed at a multidisciplinary skull base tumor board involving skull base surgeons from the fields of neurologic surgery and otolaryngology as well as neuroradiologists, neuropathologists, medical oncologists, and radiation oncologists.
Approaches to the MCF are planned in the same manner as described in Chapter 16 for the ACF. Suitability of the pathology for an endoscopic approach must be considered, and the ability to successfully treat the surgical target with available instrumentation should be confirmed.
Preoperative computer analysis should be undertaken to determine the optimal surgical approach or approaches. This is performed on a planning station, using uploaded CT and/or MRI images (Fig. 34.3). The target is highlighted (Fig. 34.7), and the three-dimensional image is examined circumferentially to familiarize the surgeon with the structures that are involved with or adjacent to the pathology. The potential pathway vectors under consideration are then diagrammed and analyzed with respect to the following:
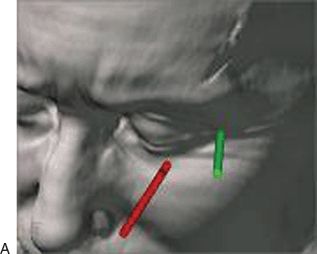
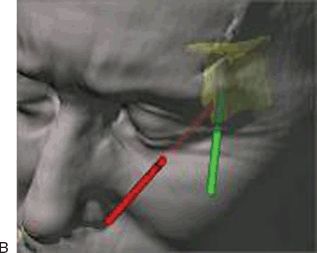
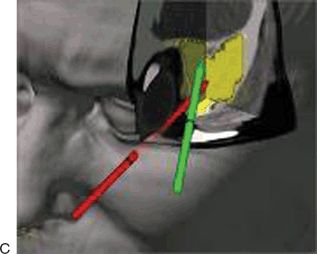
Figure 34.7 Preoperative approach planning. Lesion within bone of left greater wing of the sphenoid, segmented yellow. LRC (green
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


