CHAPTER 175 Transnasal Endoscopic-Assisted Surgery of the Anterior Skull Base
The past decade has brought about technologies and insights that have revolutionized our strategy in treating patients with lesions involving the skull base, orbit, and optic nerve. Our work developed from microscopic anterior skull base approaches that aimed to avoid nerve and brain retraction and were developed along two basic anterior midline routes, the transoral and the transnasal.1–3 We have expanded the scope of the surgery we perform through these approaches and have expanded our armamentarium in achieving postresection reconstruction. Effective and safe treatment of lesions involving the skull base still presents significant challenges, however, because although we have improved postresection reconstruction, the expanded scope of surgery has added risks to the procedures.
Surgical Anatomy
Anterior Cranial Fossa
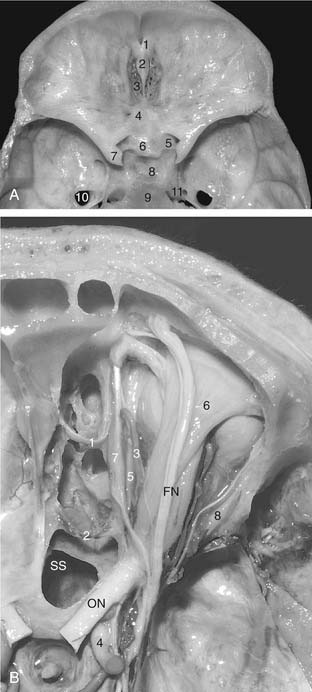
The anterior cranial fossa is composed of the orbital portion of the frontal bone anteriorly, the cribriform plate of the ethmoid bone centrally, and the lesser wing and body of the sphenoid bone posteriorly (Fig. 175-1A). The cribriform plate is located in a midline depression between the orbital roofs and separates the anterior cranial fossa from the nasal cavity. It has 15 to 20 small foramina that transmit the olfactory nerves from the superior nasal mucosa to the olfactory bulb. The crista galli projects upward at the median anterior portion of the cribriform plate and serves as the site of attachment of the falx cerebri. Between the crista galli and the frontal crest, the foramen cecum in the frontoethmoidal suture transmits an emissary vein to the superior sagittal sinus. The anterior and posterior ethmoidal branches of the ophthalmic artery exit the orbit by passing through the ethmoidal foramina to enter the cranium at the anterolateral and posterolateral edges of the cribriform plate, respectively (see Fig. 175-1B). Posteriorly, the cribriform plate articulates with the sphenoid body, which from anterior to posterior is the site of the planum sphenoidale, limbus sphenoidale, chiasmatic sulcus, tuberculum sella, pituitary fossa, and the dorsum sella. The planum sphenoidale forms the roof of the posterior ethmoid sinus and the anterior part of the sphenoid sinus and borders on the optic canals posterolaterally.4
Nasal Cavity
The nasal cavity is wider below than above and is bounded superiorly by the anterior cranial fossa, laterally by the orbits and the maxillary sinus, and inferiorly by the hard palate. This cavity is divided sagittally by the nasal septum, which is formed anteriorly and superiorly by the perpendicular plate of the ethmoid bone, posteriorly and inferiorly by the vomer, and anteroinferiorly by septal cartilage (Fig. 175-2). The nasal cavity opens anteriorly onto the face through the pyriform anterior nasal aperture and is continuous posteriorly with the nasopharynx at the posterior nasal apertures.
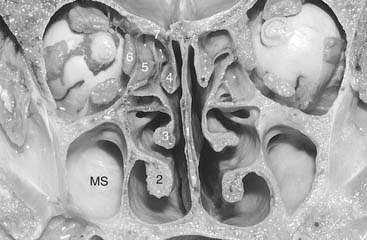
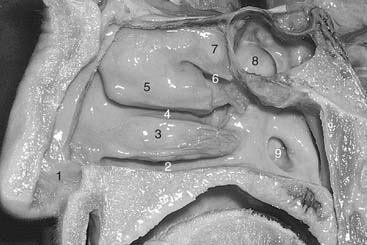
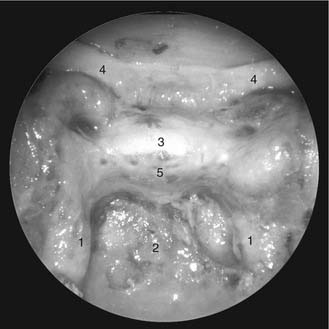
The lateral nasal wall usually has three medially directed projections: the superior, middle, and inferior nasal turbinates or conchae (Fig. 175-3). The airway passages below these turbinates are termed the superior, middle, and inferior nasal meatuses, respectively. The paired sphenoethmoidal recesses are located above and behind the superior turbinate and in front of the upper anterior aspect of the sphenoid body. They are the sites of the paired sphenoid ostia that form the communication between the nasal cavity and the sphenoid sinus (Fig. 175-4). The upper half of the lateral nasal wall corresponds to the medial orbital wall. From anterior to posterior, it is composed of the frontal process of the maxilla, the lacrimal bone, and the orbital plate of the ethmoid bone (lamina papyracea), each separated from the next by a vertical suture. The extremely thin lacrimal and ethmoid bones contain the ethmoid air cells that separate the nasal cavity from the orbit. The nasolacrimal groove and canal (the site of the lacrimal sac and nasolacrimal duct, respectively) pass downward in front of the anterior end of the middle turbinate and open into the inferior nasal meatus. The frontoethmoidal suture is located at the level of the roof of the nasal cavity and the cribriform plate.

The anterior and posterior ethmoidal foramina transmit the anterior and posterior ethmoidal arteries and nerves and are located in, or just above, the frontal ethmoidal suture. These arteries and nerves exit the ethmoidal foramina and enter the anterior cranial fossa at the lateral edge of the cribriform plate. The anterior ethmoidal artery is a terminal branch of the ophthalmic artery and supplies the mucosa of the anterior and middle ethmoid air cells and the dura covering the cribriform plate and the planum sphenoidale. The posterior ethmoidal artery usually is smaller than the anterior and is absent in nearly 30% of persons.5 It supplies the mucosa of the posterior ethmoid cells and the dura of the planum sphenoidale. The distance from the anterior lacrimal crest of the maxilla’s frontal process to the anterior ethmoidal foramen is 22 to 24 mm; the distance between the anterior and posterior ethmoidal foramina is 12 to 15 mm, and that between the posterior ethmoidal foramina and the optic canal usually is 3 to 7 mm. In the midline transfacial procedures, these ethmoidal arteries can be divided in a subperiorbital plane along the medial orbital wall. Care should be taken to prevent damaging the optic nerve, which sometimes is located immediately behind the posterior ethmoidal foramen (see Fig. 175-1B).
The inferior half of the lateral nasal wall comprises part of the medial wall of the maxillary sinus. It is formed anteriorly by the maxilla and posteriorly by the perpendicular plate of the palatine bone. The base of the middle turbinate attaches to the lateral nasal wall near the junction of the orbit and the maxillary sinus. Thus, the medial wall of the maxillary sinus is made up of the lateral wall of the middle and inferior nasal meati and the inferior turbinate. The maxillary sinus communicates with the middle nasal meatus through an opening located in the medial wall just below the roof of the sinus.4
The pterygopalatine fossa is situated between the posterior wall of the maxillary sinus anteriorly and the pterygoid process of the sphenoid posteriorly. The pterygopalatine fossa contains the pterygopalatine ganglion, which receives the nerve of the pterygoid canal (vidian nerve), the maxillary nerve just as it leaves the foramen rotundum, the internal maxillary artery (one of the two terminal branches of the external carotid artery), and the maxillary artery’s two terminal branches, the posterior lateral nasal artery and the septal artery. Both of these terminal branches enter the nasal cavity through the sphenopalatine foramen just above the caudal aspect of the bony end (not the soft tissue end) of the middle turbinate. The septal artery courses along the roof of the nasal cavity toward the sphenoid rostrum and divides into a number of vessels that extend to the septum and the superior nasal walls. In the lateral wall of the nasal cavity, the posterior lateral nasal artery divides and provides nourishment to the turbinates and meatal spaces6 (Fig. 175-5).
Paranasal Sinuses
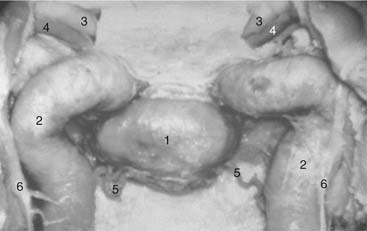
The sphenoid sinus varies in shape and size and is asymmetrically divided into two parts by an irregular septum. When the sphenoid sinus is well developed, its thin lateral wall is the medial wall of the cavernous sinus. The intracavernous portion of the internal carotid artery is the most medial structure within the cavernous sinus, and in well-developed sphenoid sinuses it produces a serpiginous bony elevation in the lateral wall of the sinus called the carotid prominence. The carotid prominence is divided into presellar, infrasellar, and retrosellar segments.11 The presellar segment corresponds to the anterior vertical segment and the anterior bend of the intracavernous portion of the internal carotid artery. The infrasellar segment corresponds to the short horizontal portion of the carotid, and the retrosellar segment reflects the posterior bend and posterior vertical segment (Fig. 175-6).
The optic canal often is partially encircled by the sphenoid sinus and creates a bony bulge in the superoanterior portion of its lateral wall. The bony depression between the optic canal and the presellar segment of the carotid prominence is called the opticocarotid recess; it extends a variable distance into the optic strut. The bony lateral sphenoid sinus wall over the internal carotid artery and the optic nerve usually is very thin and may be absent in some areas. Although Lang7 observed that the canal of the optic nerve was dehiscent in 6% of cases, Seibert8 found that 57% of the optic nerves bulged into the sphenoid sinus and 1% had no bony canal. Seibert8 also noted that the horizontal portion of the intracavernous carotid artery extended prominently into the sphenoid sinus in 67% of cases and that its bony covering was dehiscent in 6%. In his series, the maxillary nerve was prominent in the sphenoid sinus in 48% of specimens and dehiscent in 5%, and the pterygoid nerve (vidian nerve) was prominent 18% of the time.
Just below the tuberculum sellae, where they are closest to each other, the average distance between the left and right internal carotid arteries is 13.9 mm (range, 10 to 17 mm). At the anterior wall of the sella, the carotid arteries are separated by 20 mm (range, 13 to 26.5 mm), and at the level of the clivus, the distance between them is 17.4 mm (range, 10.5 to 26.5 mm).9
The maxillary sinus has thin walls that face the lower nasal cavity medially, the orbit superiorly, the infratemporal fossa posterolaterally, the pterygopalatine fossa posteromedially, and the soft tissue of the cheek anterolaterally. The maxillary sinus provides a transantral avenue for extending a midline surgical approach for more extensive lateral exposures of the cavernous sinus and the infratemporal fossa.4
Nasopharynx
The nasopharynx is situated behind the posterior nasal apertures where the septum and the inferior turbinate end. It is partially separated from the oropharynx below by the soft palate. The roof of the nasopharynx is formed by the mucoperiosteum of the upper clivus. The posterior nasopharyngeal wall is formed in successive layers by the mucosa, the superior pharyngeal constrictor muscle, the prevertebral fascia, and the longus capitis muscle. It abuts the mid- to lower clivus, the anterior aspect of the foramen magnum, and the anterior arch of the atlas (see Fig. 175-3). The pharyngeal tubercle is a small bony elevation located in the midline at the junction of the middle and lower clivus approximately 1 cm above the foramen magnum and serves as the site of attachment of the pharyngeal raphe of the superior pharyngeal constrictor muscle. The longus capitis muscles are attached to the clivus lateral to the pharyngeal tubercle on each side.
The eustachian tube, also termed the pharyngotympanic or auditory tube, opens into the lateral wall of the nasopharynx immediately posterior to the medial pterygoid plate. The fossa of Rosenmüller (pharyngeal recess) is located at the junction of the lateral and the posterior walls of the nasopharynx and projects laterally just behind the orifice of the eustachian tube. At the posterolateral depths of the fossa of Rosenmüller, only a thin layer of fibroconnective tissue separates the mucosa from the cervical internal carotid artery. The horizontal segment of the internal carotid artery in the petrous portion of the temporal bone is located immediately medial and posterior to the eustachian tube.4
Clivus
The extracranial surface of the clivus gives rise to the pharyngeal tubercle at the junction of the middle and lower clivus. The upper clivus faces the roof of the nasopharynx, which extends downward in the midline to the level of the pharyngeal tubercle (Fig. 175-7).

Retroclival Region
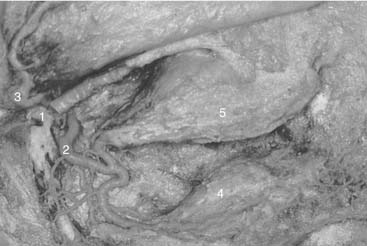
When all the bone of the posterior and lateral walls of the sphenoid sinus has been removed, only periosteum covers the underlying anatomy (Fig. 175-8). The tectorial membrane protects the clival dura in the middle and lower clivus. When the external layer of the dura is opened, the basilar venous plexus and cranial nerve VI (the aducens nerve) on each side can be seen. The average distance between the two abducens nerves at the dural emergence is 19.8 mm.10
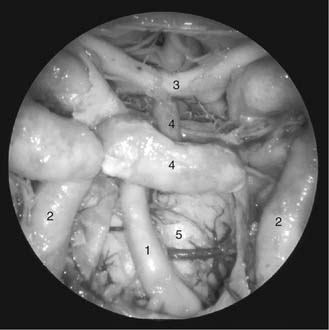
On opening the inner layer of the clival dura, the view through the 0-degree endoscope reveals the vertebral arteries, basilar artery and its branches (superior cerebellar arteries, anterior inferior cerebellar arteries), posterior cerebral arteries, brainstem, mammillary bodies, and the intradural pathway of cranial nerves III, IV, V, and VI. Just above the pituitary gland, the pituitary stalk, optic nerves, and optic chiasm can be seen. By introducing a 30-degree or 45-degree angled endoscope, it also is possible to view the cerebellopontine angle and cranial nerves VII and VIII, as well as the lower cranial nerves and the retrosellar region (Fig. 175-9).
Preoperative Assessment
CT angiography is a robust technology that allows simultaneous visualization of bony and vascular structures. Venous and arterial structures can be visualized separately in the venous and arterial phases, or seen together. “Angio-CT” is especially useful in assessing the internal carotid and vertebrobasilar systems. Venous structures of particular interest include the cavernous sinus, the inferior aspect of the superior intercavernous sinuses, and the basilar venous plexus. This technology allows us to better plan surgical procedures11 (Fig. 175-10).

Operative Technique
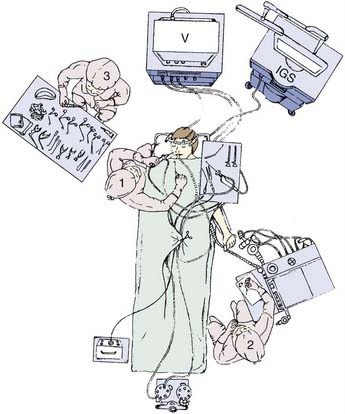
Transnasal endoscopic-assisted surgery of the skull base is performed with the patient under general controlled hypotensive anesthesia (Fig. 175-11). Compressed-rayon surgical sponges (Cottonoids) containing epinephrine, 1 : 2000 concentration, are placed in the nasal cavity, especially over the areas of surgical access. These Cottonoids are left in place for approximately 10 minutes before the surgical procedure is begun. If the surgical access is through the nasal septum, the septum is infiltrated with lidocaine and epinephrine, 1 : 100,000. When the surgery includes the pterygopalatine and zygomatic fossae and the sphenoid, the region of the sphenopalatine foramen is infiltrated with approximately 2.0 mL of the same concentration solution with an angulated 25-gauge spinal needle after first aspirating. If necessary, epinephrine-soaked Cottonoids are used for hemostasis during the surgery. If a CSF fistula is suspected, intrathecal fluorescein can be introduced at the beginning of the surgical procedure to facilitate its precise location.12 If the use of the image-guided system is contemplated, the head frame is set up for calibration.