CHAPTER 35 Nasal Fractures
The prominence and delicate structure of the nose make it vulnerable to a broad spectrum of injury, which accounts for why it is the most frequently fractured facial bone.1–11 Sports, falls, and assaults are the usual mechanisms responsible for the majority of nasal fractures, with alcohol consumption being an important contributing factor in many cases.7,8,12–19 Males are affected approximately twice as often as females in both the adult and pediatric populations, with a peak incidence occurring during the second and third decades of life.8,12,13,15,17,20,21 Deformity, swelling, epistaxis, and periorbital ecchymosis are signs that are suggestive of nasal fracture, whereas bony crepitus and nasal segment mobility are diagnostic.
Anatomy
The bony vault is a pyramid-shaped structure that is composed of paired nasal bones centrally and the frontal processes of the maxilla laterally. Ossification of these bones via intramembranous bone formation starts at the end of the third trimester and continues for years after birth.22 Superiorly the thickness of the nasal bones is greater above the level of the intercanthal line as they taper upward toward the nasofrontal suture. Below the intercanthal line, the thinner nasal bone projects anteriorly to join with the upper lateral cartilages at an externally defined midline point known as the rhinion (Fig. 35-1). On the inner surface of the nose, the perpendicular plate of the ethmoid fuses in the midline with the nasal bones to provide additional support to the nasal pyramid; this construct creates a tent-like structure, with the ethmoid plate representing a pole and the nasal bones representing the side walls of the tent. This interrelationship helps explain the susceptibility of the septum to injury by the transmitted forces from the external nose to the perpendicular plate of the ethmoid (Fig. 35-2).
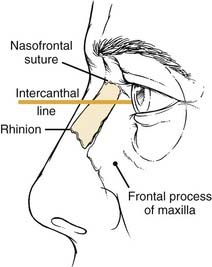
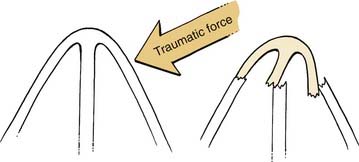
Figure 35-2. Transmitted forces from a lateral nasal bone impact resulting in fracture of the perpendicular plate of the ethmoid.
The midportion of the nose is composed of the upper lateral cartilages and the dorsal segment of the quadrangular cartilage. Made up of hyaline cartilage, these structures are fused as a single unit, with only the lower third separated by fibrous tissue.23 The cephalic ends of the upper lateral cartilages are overlapped by the nasal bones by as much as 11 mm and secured with a solid fibrous union referred to as the keystone area (Fig. 35-3).24 Laterally the upper lateral cartilages do not articulate with the bony pyramid; rather, they are attached to the frontal process of the maxilla by a fibrous aponeurosis in which the sesamoid cartilages can be found. Therefore, the preservation of the attachments of the upper lateral cartilages with the nasal bone and the septum is crucial to prevent destabilization.
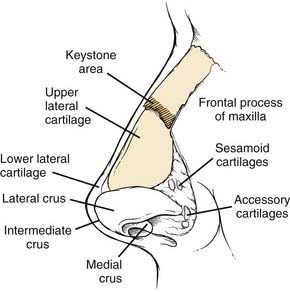
The lower third of the nose is formed primarily by the alar cartilages in addition to the accessory cartilages and fibrous fatty connective tissue that define the nostrils laterally. The alar cartilages are bilobed structures composed of medial and lateral crura with an intervening middle segment (intermediate crus) that has an important role in the definition of the nasal tip. These cartilages are interconnected as a single unit by transverse, fibrous connective tissue called the interdomal ligament.25 Structural support is mainly provided by the scrolled, overlapped upper portion of the lateral crus with the lower border of the upper lateral cartilage and the medial crural attachment with the caudal septum. The dermocartilaginous ligament, which originates from the superficial fascia of the superior nose, inserts into the intermediate crus and caudal septum to provide additional tip support.26
The septum is a key element of the structure of the entire nose. The posterior bony septum is made up of the perpendicular plate of the ethmoid superiorly and the wedge-shaped vomer inferiorly. Smaller contributions from the nasal crests of the palatine bones and the maxilla underlie the vomer and terminate anteriorly at the nasal spine. Extending anteriorly toward the nasal spine, the superior edges of the vomer and nasal crest of the maxilla form a bony groove in which a thickened inferior portion of the quadrangular cartilage lies. This articulation represents the basal foundation upon which all of the overlying nasal structures rest. Mobility of the cartilage within the groove helps prevent septal fractures by allowing for slight lateral rotation during compression of the septum.25 A thickened osteocartilaginous buttress along the septoethmoid junction is the main strut for the bony and cartilaginous dorsum, whereas a thick caudal septum provides the majority of the nasal tip support.
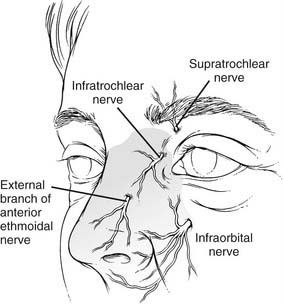
The sensory innervation of the nose is supplied by the first two divisions of the trigeminal nerve. The supratrochlear, infratrochlear, and external branches of the anterior ethmoid nerves (V1) provide sensation to the upper, dorsal, and nasal tip surfaces, whereas the infraorbital nerve (V2) supplies sensation to the side walls (Fig. 35-4). Internally along the lateral nasal wall, the anterior and posterior ethmoidal nerves provide sensation to the upper portions of the nasal cavity. The sphenopalatine ganglion (V2), which originates at the end of the middle turbinate, provides innervation throughout the posterior nasal cavity. Branches from anterior and posterior ethmoid nerves and the sphenopalatine (nasopalatine) nerve cross over superiorly and posteriorly to provide sensation to the majority of the septum.
Pathophysiology
Understanding the process by which nasal fractures occur and how injuries to key areas of support can alter appearance and function are essential to appropriate treatment. Variables such as force, impact direction, nature of the striking object, patient’s age, and other host factors will influence the pattern of injury to both the bony and cartilaginous components of the nose. Younger adults often suffer the dislocation of major segments, whereas older individuals tend to have more comminution of brittle, osteopenic nasal bones.27 Children, on the other hand, have more cartilaginous injuries and greenstick fractures due to a greater proportion of nasal cartilage and the incomplete ossification of nasal bones.9
A combination of the projection of the nose and its relatively fragile supporting structures as compared with other facial bones make it particularly susceptible to fracture. The thinner nasal bone below the intercanthal line, which projects more prominently from the face, is fractured much more easily than the thicker bone of the nasal root above the line. Lateral forces may produce an ipsilateral depressed fracture or may outfracture the opposite nasal bone, thereby resulting in significant deviation of the entire nose. Although lateral forces are a more frequent cause of nasal injuries,3 deviated fractures can occur from either frontal or laterally directed impacts as well.28
The cartilaginous portions of the external nose are able to absorb a greater amount of force without fracture as compared with the bony components, but they are still susceptible to injury given their greater exposure. Avulsion and dislocation of the upper lateral cartilage from the nasal bone and septum will result in a hollowed-out appearance of the midportion of the nose.24 This injury may also tear the external nasal artery as it exits between the nasal bone and upper lateral cartilage, thereby causing a dorsal hematoma.29 In cases of severe frontal trauma, reduction of nasal projection and increased nasal tip rotation are indicative of fracture and telescoping of the cartilaginous portions of the anterior nose and caudal septum.30
Septal injury is one of the most crucial elements of nasal deformity and dysfunction. The thinnest portions of the septum that tend to fracture most readily are located around the superior septal angle, the central-dorsal area of the quadrangular cartilage, and the posterior portion of the perpendicular ethmoid plate. Cadaver studies done both by Harrison28 and Murray and coworkers18 found that either frontal or lateral forces produced a consistent C-shaped fracture through the cartilaginous septum and perpendicular plate. Failure to reduce these septal fractures has been shown to be responsible for many cases of decreased nasal projection and lateral deviation found after unsuccessful attempts at closed reduction.18 Transmitted impact forces from the nasal bones and upper lateral cartilages can also result in septal dislocation off the maxillary crest, thus further destabilizing overlying structures and aggravating airway obstruction. Incomplete fracture of the septal cartilage was hypothesized by Fry30A to cause the release of “interlocked stress” within the cartilage, which leads to further deformity.
Associated Injuries
Injury to the structures that surround the nose often occurs in cases of high-velocity impacts, such as those sustained in motor vehicle accidents. Epiphora from disruption of the nasolacrimal drainage system occurs with 0.2% of nasal fractures.31 Severe injuries with fracture of both the lacrimal bones and the ethmoidal complex are associated with depressed nasal fractures from frontally directed forces.27 Widening of the intercanthal distance caused by the detachment of the medial canthal tendons is a classic appearance of these fractures, and these are better known as nasal-orbital-ethmoid complex fractures. Hard palate instability and open bite deformity are signs of Le Fort’s fracture, whereas unilateral malar deformity and facial asymmetry suggest a zygomaticomaxillary complex fracture. Significant trauma to the upper portions of the facial skeleton may be associated with frontal sinus fracture, cribriform plate fracture, and dural tears leading to pneumocephalus and cerebrospinal fluid rhinorrhea.32
Classification
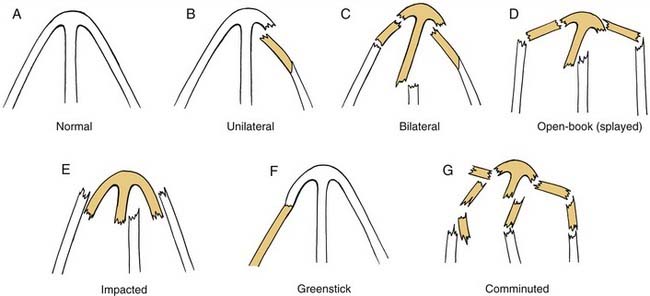
Due to the variations in individual anatomy and trauma etiology, there are several different types of nasal injuries that may be encountered. Fractures of the bony pyramid may be described as unilateral, bilateral, comminuted, depressed, open-book (splayed), impacted (telescoped), and greenstick (Fig. 35-5). Septal damage should also be documented for fractures that have caused deviation or dislocation off the maxillary crest. The extension of fractures to involve surrounding structures such as the maxilla, lacrimal bone, ethmoid complex, or frontal sinus should be included in the description as well.
Although there have been many attempts to apply an all-encompassing classification scheme to nasal fractures, the wide variety of injuries has precluded the acceptance of a single system that has practical application. Anatomic descriptions of nasal injuries often focus on the fracture pattern of the nasal bones but do not include cartilaginous components4 or do not describe the involvement of surrounding structures.28 Murray and Maran8 attempted to narrow down fractures of the nasal bones and septum to seven anatomic groupings using data collected from cadaver experiments. Although their publication is popularized for highlighting the importance of septal management to the overall success of reduction, the classification has not been widely accepted because of its complexity.
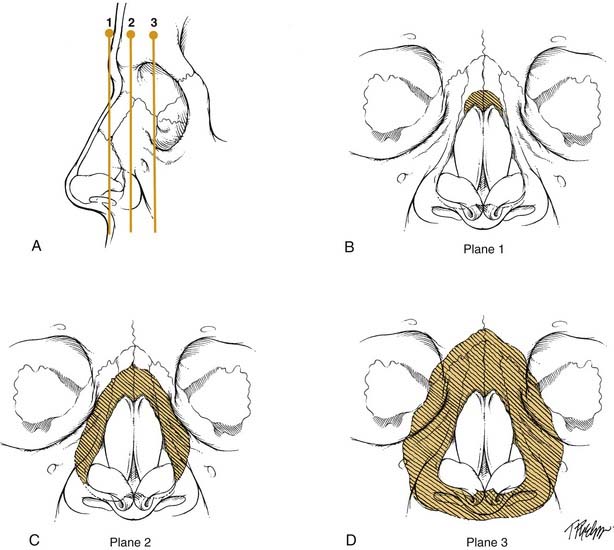
The other broad method of categorization is based on the direction of the impact force. Lateral-type injuries, which are more common, tend to have less severe damage and a better prognosis than the frontal types.27,33 Stranc and Robertson33 developed a classification system using these two main groups, with further breakdown of the frontal type into three different planes that are determined by the depth of injury from the nasal tip (planes 1 through 3) (Fig. 35-6). Each successive plane is associated with a higher likelihood of residual deformity after reduction. Plane 1 injury includes damage to the anterior nasal spine, the anterior septum, or the lower ends of the nasal bones. Dislocation and telescoping of the upper lateral cartilages and septum may be found with a plane 1 injury. Plane 2 injury results in more extensive damage to the nasal bones and ascending maxillary process but does not involve the orbital rims. The septum has a significant amount of deviation and may lack stability to support the nasal dorsum. Plane 3 injury results in nasal-orbital-ethmoid complex disruption. Patients with this injury are usually found to have other midface and cranial base fractures; the nasal bones and septum are severely comminuted and overlapped. Surgery for plane 3 injuries often is unable to fully restore the preexisting nasal appearance and function, particularly if the orbital-ethmoid complex components of the injury are not recognized and treated properly. These conclusions were supported in a study by Daw and Lewis3 that showed a significantly higher incidence of residual anatomic and functional defects in frontal injuries as compared with lateral injuries.
Diagnostic Assessment
History
A detailed account of the events surrounding nasal trauma is helpful in determining the type and severity of injuries that may be present. In cases of motor vehicle accidents, information about the speed, direction of impact, and the presence of restraining devices should be obtained. Young children who are located in the front passenger seat are at risk for head and cervical injuries related to airbag deployment, even in incidences of low-speed collisions. Patients who present after an assault should be questioned about the nature of the striking object and the direction of the blows. It is important to note that up to 30% to 60% of women with facial trauma as a result of assault are victims of domestic violence.34,35
In addition to changes in appearance, the patient history should be evaluated for functional changes in nasal breathing and smell as well as bleeding and watery drainage with a sweet/salty taste (possible cerebrospinal fluid [CSF] leak). Although loss of smell should be documented, poor nasal airflow as a result of edema is almost always present at the initial interview and therefore sense of smell should be reassessed after swelling has diminished. Persistent anosmia or hyposmia may occur in as many as 5% of individuals who suffer head injury with or without nasal trauma and has been observed to resolve spontaneously in only a third of cases.36
A review of a patient’s medical history includes any prior nasal injury, deformity, surgery, dyspnea, allergies, or sinus disease. Individuals who have had prior rhinoplasty are more susceptible to nasal fracture, even after complete healing.37 Old photographs or detailed descriptions of previous nasal deformities should be assessed for significant changes; up to 40% of normal individuals without a history of nasal trauma have evidence of significant malformation.7 A complete review of systems should also screen for associated trauma (e.g., ophthalmic or cervical spine injuries).
Physical Examination
Before the evaluation of internal structures, all necessary equipment and medications for the examination should be ready at the bedside, including materials to control epistaxis. Using a headlight and a nasal speculum, clotted blood is removed with a Frazier suction to visualize all mucosal surfaces for evidence of mucosal tears, hematoma, and active bleeding. The use of topical decongestants will aid visualization and help control bloody oozing. The septum is carefully evaluated for any abnormal soft-tissue swelling that is indicative of a hematoma. Bimanual palpation of the septum with cotton-tipped applicators helps differentiate hematoma, which tends to be more compressible than tissue edema. Areas of increased mobility are suggestive of septal fracture. The use of a 0- or 30-degree 4-mm rod telescope is particularly helpful to assess for posterior septal abnormalities and localization of occult bleeding sources. Although fracture and dislocation of the nasal septum is a common occurrence with nasal trauma, up to 50% of normal individuals without a history of significant nasal injury have a deviated nasal septum.6
If the patient can be examined while heavily sedated, a more complete assessment of the condition of the supporting nasal structures is possible. The Brown-Gruss provocation maneuvers break down the analysis of the infrastructure of the nose into upper, middle, and lower segments by applying digital pressure over each of the compartments.38 Lower vault compression (Brown-Gruss III) may show hyperrotation of the nasal tip with disruption of the septal angle or inward collapse if the supporting caudal septum is severely fragmented. Middle vault compression (Brown-Gruss II) will produce a saddle deformity when the central portion of the septum has been damaged. Upper vault compression (Brown-Gruss I) will cause collapse of the upper third of the nose in cases with severe comminution of the nasal bones and frontal processes of the maxilla. Complex fractures with two or more involved vaults will show more extensive collapse or even complete disappearance of the nose in cases in which severe trauma has affected all three vaults.
Radiography
Despite clear evidence that plain films do not have a role in the management of nasal fractures, these studies are frequently obtained to evaluate individuals after nasal trauma. An investigation by de Lacey and others39 found that plain films had a 66% false-positive reading as a result of the misinterpretation of normal suture lines or developmental thinning of the nasal bones. It is also difficult to distinguish old fractures from new ones on plain films, because only 15% of nasal bone fractures heal by ossification.40 These studies are further limited by their inability to detect cartilaginous injuries, which are more prevalent in pediatric cases. Logan and colleagues16 found that, out of 100 consecutive patients presenting with nasal trauma who had undergone nasal radiography, in no case did the plain film alter management. The diagnosis and proper treatment of the majority of nasal injuries should be successfully achieved with the use of the history and physical findings alone.
However, in cases involving more severe trauma and in which there is physical evidence of other facial fractures, computed tomography should be employed to assess the extent of bony injury. Thin cut coronal and axial views are most appropriate for the evaluation of midfacial, orbital, and frontal sinus fractures. For extensive injuries involving the nasal-orbital-ethmoidal complex, a combination of both two- and three-dimensional computed tomography is recommended for the localization of fractures and the spatial orientation of displaced fragments.41



