CHAPTER 58 Voice Evaluation
Patient Scales
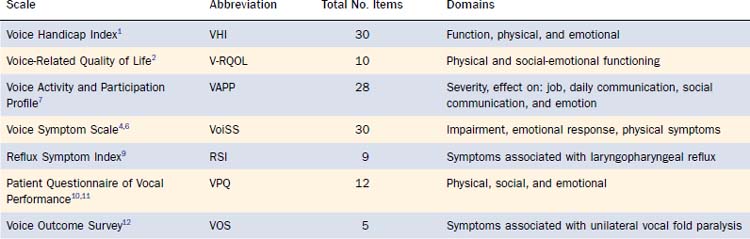
Two commonly used scales, the Voice Handicap Index (VHI)1 and Voice-Related Quality of Life (V-RQOL),2 are described here. Details and information about scale construction can be found in the reference articles, and a synopsis of current scales can be found in Table 58-1.
Voice Handicap Index
The Voice Handicap Index was designed to assess handicap, “a social, economic, or environmental disadvantage resulting from an impairment or disability.”3 The instrument consists of 30 statements that patients rate on a 5-point equal-appearing interval scale that reflects the frequency of occurrence. The total possible score is 120, with higher scores reflecting greater handicap. Although the initial publication suggests division into functional, physical, and emotional subscales,1 other writers have questioned the subscale structure,4,5 suggesting that total score appears more meaningful. Since its publication in 1997, the Voice Handicap Index has been widely used to show voice handicap in specific groups of patients, comparisons between handicap and vocal function measures, and change with treatment.
Other Patient Scales
The Voice Symptom Scale (VoiSS)4,6 is a psychometrically sound 30-item scale representing physical impairment, emotional response, and related physical symptoms. The Voice Activity and Participation Profile (VAPP)7 follows the terminology and framework of the World Health Organization’s 1997 revision8 of the International Classification of Functioning, Disability, and Health. Patients indicate their extent of limitation in daily activities and restriction of participation in corresponding activities.
The Reflux Symptom Index (RSI), the Patient Questionnaire of Vocal Performance (VPQ), and the Voice Outcome Survey (VOS) are more limited in scope. The Reflux Symptom Index, made up of 9 items, is designed to document patient symptoms of laryngopharyngeal reflux.9 The Patient Questionnaire of Vocal Performance is a 12-item scale designed to assess the physical, social, and emotional impacts of a nonorganic voice disorder.10,11 The Voice Outcome Survey is a 5-item survey designed for patients with unilateral vocal fold paralysis.12
Perceptual Evaluation
Auditory Perceptual Assessment
Several formal measures and scales have been proposed to rate voice quality; two of the most commonly used scales are described here. Auditory perceptual ratings are appealing because the ultimate goal of voice treatment is to improve perceived voice quality. Unfortunately, such measures are fraught with definition, rating, and interpretation difficulties. Voice quality is difficult to define, leading to many, often circular, definitions of each term. Raters have different internal representations of the parameters and severity. It is difficult to differentiate between related qualities, and univariate ratings do not often correlate well with global ratings or measurements (for a detailed discussion, see Kreiman and Gerratt13). Although auditory perceptual assessment often results in a number, the number represents a perceptual judgment rather than a measurement and should be treated accordingly.
GRBAS
GRBAS is a well-known standard scale that was developed by the Committee for Phonatory Function of the Japanese Society of Logopedics and Phoniatrics. As described by Hirano,14 the G represents grade or overall quality. The other four letters represent dimensions of voice quality, as follows: R for roughness, B for breathiness, A for asthenia, and S for strain. Descriptions of each parameter are given in Table 58-2. Each parameter is rated on a 4-point scale: 0 means that there is no deficit in this parameter, 1 is a mild deficit, 2 is a moderate deficit, and 3 indicates a severe deficit. There is no standard recommendation for the type of utterance(s) to use with GRBAS, so specific information about testing conditions should be documented in the report.
Table 58-2 GRBAS Scale for Auditory-Perceptual Evaluation
| Parameter | Hirano Definition* | National Center for Voice and Speech Definition† |
|---|---|---|
| Grade (G) | Overall severity | |
| Roughness (R) | Psychoacoustic impression of irregular vocal-fold vibration | An uneven, bumpy quality that appears to be unsteady in the short term but stationary in the long term; acoustically, the waveform is often aperiodic, with the modes of vibration lacking synchrony, but voices with subharmonics can also be perceived as rough. |
| Breathiness (B) | Psychoacoustic impression of air leakage through the glottis | Containing the sound of breathing (expiration) during phonation; acoustically, breathy voice, like falsetto, has most of its energy in the fundamental, but a significant component of noise is present owing to turbulence in the glottis. In hyperfunctional breathiness, air leakage may occur in various places along the glottis, whereas in normal voice, air leakage is usually at the vocal processes. |
| Asthenia (A) | Weakness or lack of power in the voice | A voice that appears too low in effort, weak; hypofunction of laryngeal muscles is apparent. |
| Strain (S) | Psychoacoustic impression of a hyperfunctional state of phonation | A voice that appears effortful; visually, hyperfunction of the neck muscles is apparent; the entire larynx seems compressed. |
* From Hirano M. Clinical Examination of Voice. New York: Springer-Verlag; 1981.
† From Titze IR. Workshop on Acoustic Voice Analysis: Summary Statement. Iowa City, IA: National Center for Voice and Speech; 1995.
CAPE-V
The Consensus Auditory-Perceptual Evaluation–Voice (CAPE-V) was developed at a 2003 consensus conference sponsored by the American Speech-Language-Hearing Association Special Interest Division 3, Voice and Voice Disorders.15 Six core and additional examiner-selected parameters are rated on a visual analog scale. The clinician uses a tick mark to rate function on a 100-mm line and then measures the distance from the left end of the line to establish a score; higher scores reflect a more severe deviation from normal quality. Core parameters are overall severity, roughness, breathiness, strain, pitch, and loudness. The judged parameters are identified as consistent or intermittent, and resonance differences can be noted. The CAPE-V is to be scored from two sustained vowels, six standard sentences, and at least 20 seconds of natural running speech. Recommendations about testing and recording environments are included.
Visual Perceptual Examination
The visual perceptual examination refers to visible and physical aspects of voice production related to etiology, maintenance, or effect of dysphonia. Koschkee and Rammage16 have divided the visual perceptual examination into the following five categories: (1) general appearance; (2) posture, breathing, and musculoskeletal tension; (3) neurologic dysfunction; (4) physical dysmorphology; and (5) clinical manifestations of disease. Several components of the visual perceptual evaluation are described in more detail here.
Tactile Perceptual Evaluation
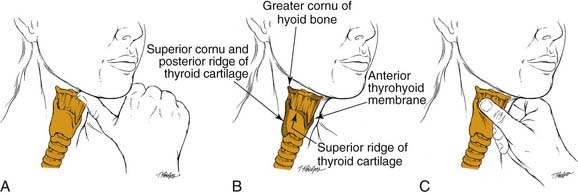
The manual examination of laryngeal musculoskeletal tension includes palpation of the suprahyoid muscles, the major horns of the hyoid bone, the superior cornu and the lateral aspects of the thyroid cartilage, the thyrohyoid space, and the anterior border of the sternocleidomastoid muscle. It is useful to assess suprahyoid tension and thyrohyoid space both at rest and during phonation. The examiner should also attempt to move the thyroid cartilage from side to side.17–19 Figure 58-1 depicts this evaluation. Some authors recommend palpating the thyrohyoid, cricothyroid, and pharyngolaryngeal (inferior constrictor and posterior cricoarytenoid) muscles as well.20,21 Normal findings include palpable space between the hyoid bone and the superior border of the thyroid cartilage and mobility of the laryngeal complex. Findings indicative of excessive musculoskeletal tension include pain with palpation (frequently more severe on one side), decrease or absence of thyrohyoid space at rest or with phonation, muscle “knots,” high carriage of the hyoid bone and thyroid cartilage, and difficulty rotating the larynx.17–21
Measures
Chest Wall Displacement
Measurements of chest wall movement can be used to estimate volume changes during voice production. Reports typically include information about the lung volumes used and chest wall shape during phonation. Lung volume variables of interest are the volumes at which the patient initiates and terminates speech. In general, people tend to initiate phonation around 20% of vital capacity above resting tidal end-expiratory level and to terminate phonation around resting tidal end-expiratory level.22 Shape is usually described in terms of rib cage wall and abdominal wall movement. Because some shapes are more mechanically advantageous to phonation, the patient’s typical shape and ability to change shape might be reported.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


