CHAPTER 25 Nasal Reconstruction
Reconstruction of nasal defects is a common procedure for facial plastic surgeons. Such defects may result from trauma, tumor resection, prior aesthetic rhinoplasty, or congenital deformities. When planning for reconstruction of distorted or missing tissues of the nose, the surgeon should consider both form and function. Systematic evaluation of nasal defects involves perception of the nose as a three-layered structure: (1) a cover of skin and subcutaneous fibrofatty tissue, (2) an underlying bony and cartilaginous framework, and (3) a soft tissue lining of vestibular skin and nasal mucosa. Defects may involve any combination of these layers. The choice of tissue for reconstruction is generally determined by which elements are missing. The primary reconstructive goal is that each component be restored as closely as possible to its original anatomic state for optimal functional and aesthetic outcome.1
External Covering Layer
The nose has been described as being composed of concave and convex surfaces separated by ridges and valleys.2 These surfaces, known as aesthetic or topographic subunits, include the tip, the dorsum, the paired side walls, alar lobules, soft triangles, and the columella. When a defect involves greater than 50% of a subunit, replacement of the entire subunit is often better than replacement of only a part. Placement of scars along contour lines re-creates normal highlights and landmarks. Although this may require some healthy tissue to be discarded, the outcome is often improved.
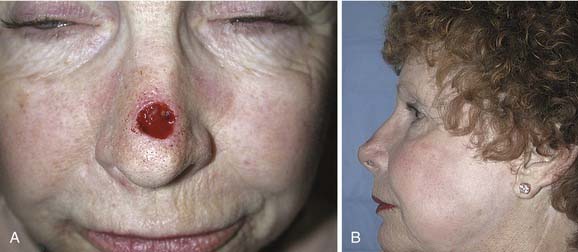
Options for repairing defects involving skin alone include healing by secondary intention, primary closure, skin grafting, and local and regional flap coverage. The choice of method is best guided by evaluation of location and depth of the wound. Healing of superficial wounds by secondary intention on concave surfaces may result in a satisfactory aesthetic outcome. For example, this method is a good choice for wounds of the medial canthal region where advancement of local tissue may distort the eyelids. However, when wounds on convex surfaces heal by secondary intention, the result is often a flattened or depressed scar. Similarly, primary closure may be used for a small defect of the mobile skin over the nasal dorsum, whereas closure of a similar defect over the tip region may result in alar retraction or asymmetry. However, in patients with tip ptosis, primary closure of a symmetrical supratip defect can improve functional as well as aesthetic results of the nose (Fig. 25-1).
Full-thickness skin grafts (FTSGs) are useful in the reconstruction of superficial defects involving convex surfaces of the nose. This is especially true in the areas of the tip and alar lobules where tissue mobility is limited for the creation of local flaps. Donor sites for FTSGs include the preauricular, postauricular, nasolabial, supraclavicular, and upper eyelid skin, each providing good color match and an easily hidden donor site. Tissue from the nasolabial crease results in the most satisfactory aesthetic reconstruction because it matches most closely the thickness, color, and texture of nasal skin.3,4 When the defect is deeper than the thickness of an FTSG, it can granulate for 7 to 14 days before the granulation tissue surface is scraped and a delayed skin graft is placed.
Because of the sebaceous nature of the lower third of the nose, an FTSG may heal with a contrasting flattened, shiny appearance.5 Thus the best results are obtained when FTSGs are used to repair superficial defects in areas of the nose where the skin is naturally thin and nonsebaceous. In addition, when placing an FTSG for reconstruction, it is often best to excise sufficient normal tissue to allow replacement of an entire nasal subunit to minimize a patched appearance. Dermabrasion of the area 3 months after grafting further improves texture match between the graft and its recipient site.6
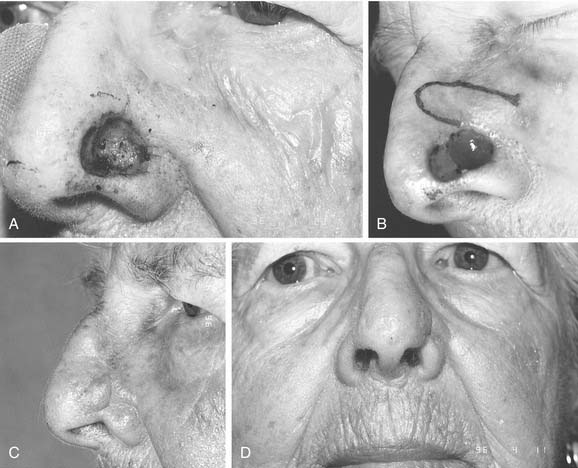
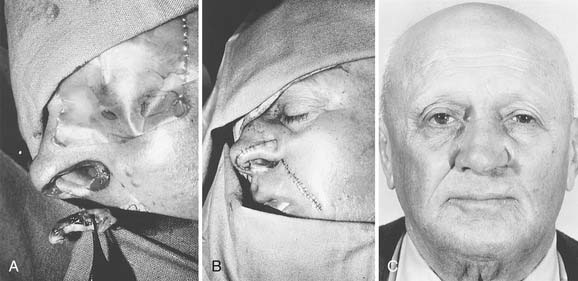
Local flaps provide several advantages over skin grafts in nasal reconstruction. Contour, color, and texture match are usually superior to FTSG, and there is usually less scar contracture, contributing to a more reliable aesthetic and functional result. Survival is greater with local flaps than with grafts because of the abundant vascular supply of the dermal and subdermal plexus. Choice among the many flaps available depends on the area of the nose to be reconstructed and the secondary deformity that will result. Simple transposition and bilobed flaps are common choices for coverage of soft-tissue defects of the dorsum or lateral walls. Using Zitelli’s modifications of the original design, the bilobed flap is the most useful of the nasal cutaneous flaps.7 This flap is most useful in the lower half of the nose where the skin from the nasal dorsum and the cheek can be recruited to close the defect of the second lobe (Fig. 25-2). Glabellar flaps are used for the more superior areas8; whereas the dorsonasal or Rieger flap is useful for single-stage repair of the more caudal regions.9 A retroauricular flap is an excellent technique for difficult nasal reconstruction in young patients. Transferring retroauricular tissue on a temporal pedicle was first described by Washio.10 Flaps should be designed so that incisions are hidden within relaxed skin tension lines and along borders of natural aesthetic units as much as possible. Wide undermining of the nasal skin and, in some cases, reduction of a dorsal hump are necessary for closure without tension. These local flaps are useful for defects of about 2 cm or less in diameter (Fig. 25-3).11

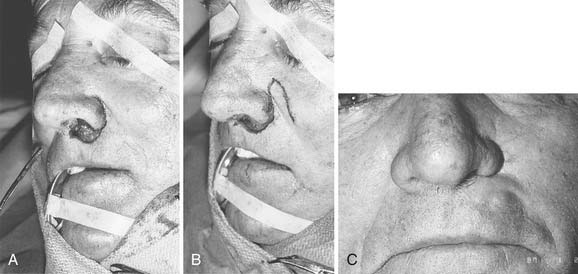
Since the earliest descriptions of the melolabial flap, many variations have been reported.12 Based superiorly, the flap may be used for defects of the lower two thirds of the nose (Fig. 25-4). With full-thickness defects, the distal portion of the flap may be turned on itself to provide internal lining coverage. When based inferiorly, the melolabial flap is appropriate for reconstruction of the upper lip, floor of nose, and columella (Fig. 25-5). Larger defects can be reconstructed using bilateral melolabial flaps or a combination of local flaps with cheek advancement.
The melolabial flap may also be used as an island flap.13 In this procedure, a circumferential skin incision is made to create a flap the size of the defect. After wide undermining of the skin, a vascular pedicle of subcutaneous tissue is made, extending from the skin island superiorly toward the infraorbital rim. The flap is then tunneled beneath the skin bridge and rotated into the defect with its subcutaneous pedicle intact. This permits one-stage reconstruction, usually without effacement of the nasofacial or alar-facial creases. The usual design of the melolabial flap requires two stages to complete, with the second procedure being a revision of the pedicle. Tacking sutures from the flap dermis to the underlying periosteum8 or temporary external mattress sutures may be used to recreate the nasofacial convexity.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


