Fig. 552 Transcanal anterior atticotympanotomy and cortical mastoidectomy (Farrior). A Farrior modification with the retroauricular approach is performed with removai of the ear canal skin, except between the 12-o’clock and 3-o’clock positions. The epithelium from the anterior part of the drum, in a situation of posterior perforation, is also removed. An anterior atticotympanotomy is performed by enlarging the ear canal up to the mastoid tegmen, leaving an intact but displaced bony ear canal between the posterior mastoidectomy and the anterior atticotomy, and exposing the entire medial wall of the attic with the lateral semicircular canal and the horizontal part of the facial nerve. The posterior bony ear canal is also widened, especially the bony annulus, exposing the genu of the facial nerve, the pyramidal eminence, the styloid eminence, and the tympanic sinuses. The drilling can be further extended to the hypotympanum. The idea is to ventilate the mastoid cavity (arrows)
If the pathology requires furter exposure of the posterior tympanum, e. g., in sinus cholesteatoma or tensa retraction cholesteatoma with involvement of the tympanic sinuses, further drilling of the posterior bony ear canal wall is performed, exposing the entire horizontal part of the Fallopian canal, the genu, and part of the vertical canal, as far as the chorda tympani, which can occasionally be preserved (Fig. 556). Usually, the chorda tympani has to be sacrified, and the posterior bony ear canal is further removed, exposing more of the Fallopian canal and the styloid eminence. A good view is provided of the tympanic sinuses, and the cholesteatoma can be safely removed. If it is required, there is a good opportunity with this technique, to continue down into the hypotympanum in order to remove cholesteatoma.

Fig. 553 The Farrior modification of the retroauricular approach, with exposure of the mastoid plane and the lower border of the temporalis muscle, as well as the terminal line, in a situation of sinus cholesteatoma and posterosuperior perforation. A circumferential ear canal incision between the 12-o’clock and 3-o’clock positions at the level of Henle’s spine, and two radial incisions at the 12-o’clock and 3-o’clock positions are performed. These two incisions are connected with a circumferential incision close to the annulus

Fig. 554 The epithelium from the drum remnant and the canal skin is removed all the way around, exposing the superior, posterior, and inferior aspects of the bony ear canal. A small cortical mastoidectomy is performed far posteriorly, and the ear canal is widened from the 1-o’clock to the 9-o’clock positions. Osteosclerosis drilling is performed to obtain information about the ossicular chain
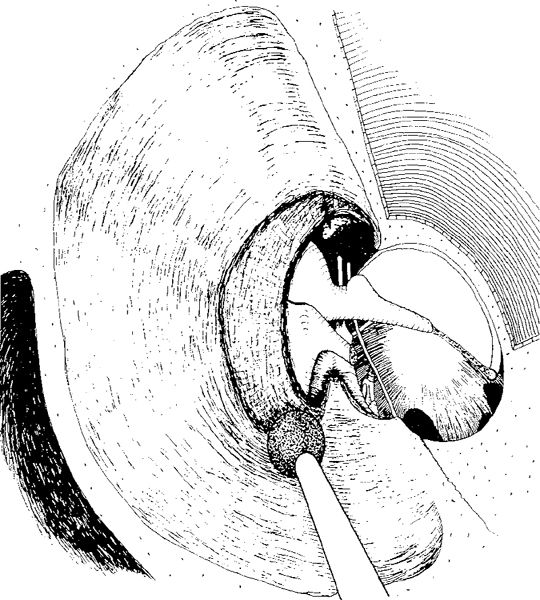
Fig. 555 With further enlargement of the ear canal and removal of the superior and posterior bony annulus, an atticotomy is performed, and part of the lateral attic is exposed. Posteriorly, with continuous drilling of the bony annulus, the facial nerve and the pyramidal eminence are exposed. The anterior bony plate (the cog) is visible (arrow)

Fig. 556 The anterior bony plate is removed and the anterior attic is further exposed, allowing a good connection to the epitympanic sinus and Eustachian tube. The lateral attic wall is almost completely removed up to the tegmen tympani and antri. After removal of the incus, the posterior and the medial attic become visible, and removal of the cholesteatoma can be carried out
To expose the entire attic, the overhangs of the mastoid tegmen and tegmen tympani are smoothened. After resection of the malleus head, as Farrior recommends, and after removal of all pathology, the transmeatal anterior atticotympanotomy is complete (Fig. 557). One must now complete the transcortical posterior mastoidectomy in order to remove any residual disease in the antrum and the mastoid process (Fig. 558).
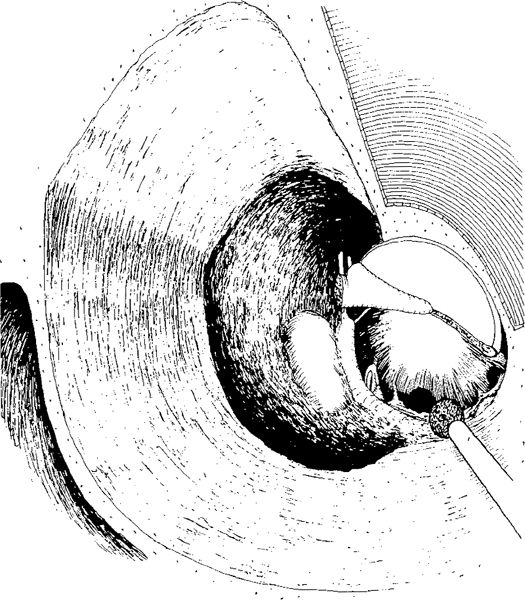
Fig. 557 The head of the malleus is resected, and the entire medial wall of the attic is cleaned. The bony overhangs of the lateral attic bone are removed, and the attic is enlarged as far as the tegmen tympani. The ear canal is further enlarged, and its bony wall is posteriorly displaced. In order to clean the tympanic sinuses, more of the posterior ear canal wall is removed, including the chordal eminence and the bone inferior to the chorda toward the hypotympanum

Fig. 558 Mastoidectomy is further elaborated. The bony ear canal wall is extremely thinned and displaced further posteriorly, but remains widely intact laterally. The “new” ear canal goes up to the mastoid tegmen. Reconstruction of the cavity: An autogenous incus is placed on the stapes. Farrior places the malleus head in the attic, possibly with a piece of bone to maintain a bony annulus. A piece of free temporalis muscle is placed in the facial recess, behind the bridge to prevent retraction (arrow)
Reconstruction of the Anterior Atticotympanotomy and Mastoidectomy
Farrior considers this technique a closed technique, and hopes for repneumatization of the mastoid cavity. By placing the resected malleus head over the lateral semicircular canal, Farrior attempts to achieve support — a form of bridge — for the fascia, and also to maintain a certain depth and ventilation of the attic. However, ventilation of the mastoid cavity can only take place superior to the malleus head (Fig. 558). A further piece of bone can be placed over the lateral semicircular canal. Within the mastoid cavity, behind the ear canal wall, Farrior places a piece of temporalis muscle as a free graft (Fig. 558) in order to prevent retraction into the cavity.
The drum, the attic, and most of the denuded bone are then covered by fascia as an anderlay graft. The drum and the lateral attic wall are covered as a sandwich graft with a free ear canal skin graft placed onto the fascia graft (Fig. 559).
Farrior recommends this form of mastoidectomy in cases with attic or sinus cholesteatoma with a poorly pneumatized zygomatic region and a well-pneumatized mastoid process. Farrior usually performs the anterior atticotympanotomy first, and then the transcortical mastoidectomy.
In the present author’s opinion, this approach is very flexible, because the posterior mastoidectomy can be avoided if a small cell system is present and the anterior atticotomy can be simply extended in a posterior direction as a canal wall-down procedure, i. e., an atticoantrotomy.
Although Farrior’s intention is to achieve a ventilated attic, it is the author’s opinion that the anterior attic will usually be obliterated by the presence of the malleus head, and this technique must therefore be considered more as a canal wall–down than a canal wall–up technique, especially since the bony ear canal wall is displaced. The residual ear canal is situated between the antrum and the aditus ad antrum, leaving the attic uncovered. One can imagine that adhesions in the attic will soon close off the superior ventilating route to the mastoid cavity (Fig. 560a) along the tegmen tympani. The inferior ventilating route through the facial recess has already been closed off with muscle.
The consequence of this inability to ventilate the mastoid cavity leads, in the present author’s opinion, to obliteration of the mastoid cavity, with complete and permanent closure of the connection between the aditus and the antrum. It is difficult to imagine what benefit good ventilation of the cavity might have for hearing in cases of a displaced bony ear canal wall (Fig. 560b).

Fig. 559 Reconstruction of the attic. Reconstruction with fascia as an underlay graft covering the incus, the malleus head, and the cortical bone, in order to pneumatize the attic and the mastoid cavity. Fascia covers the bony ear canal. Over the drum region and the attic region, the free ear canal skin graft is placed using a sandwich technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


