Fig. 490 Osteoplastic mastoidectomy (Schnee). After excising the margins of the posterior perforation to be closed at the end of the operation, a large posterosuperior circumferential incision of the ear canal skin is made
The bone adjacent to the facial recess can be drilled away, both medial and lateral to the chorda tympani, under direct vision.
After the osteoplastic mastoidectomy has been completed, the bony ear canal wall is replaced in its normal position (Fig. 498), and the transcanal part of the procedure ensues with ossiculoplasty, closure of the drum perforation with underlay vein or fascia graft, and replacement of the ear canal skin. Care is taken to cover the resulting defects in the bone (Fig. 499). Lastly, the ear canal is filled with Gelfoam.

Fig. 491 The tympanomeatal flap and the fibrous annulus, including the drum remnant, are elevated, exposing the posterior half of the tympanic cavity. The elevation is continued far anteriorly, exposing the lateral wall of the attic. The bony annulus from the 9-o’clock to the 1-o’clock positions is removed by drilling with a diamond burr, exposing the horizontal part of the facial nerve, the whole of the long process of the incus, the neck of the malleus, and the anterior malleolar ligament
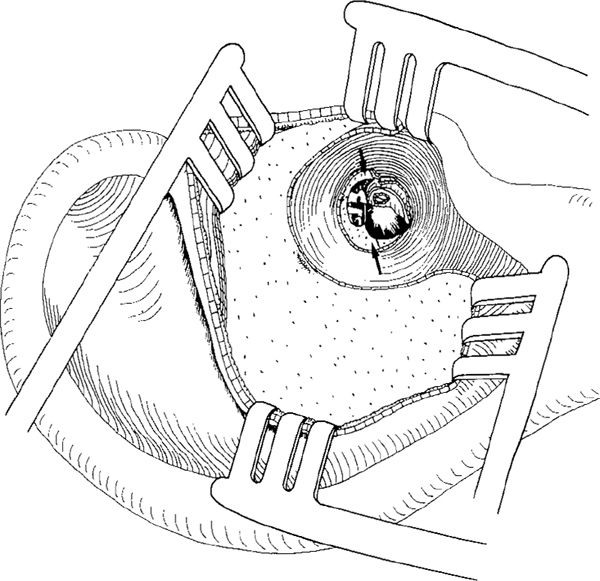
Fig. 492 A modified Lempert’s endaural approach is applied with a vertical incision and a circumferential incision through the meatal skin at the entrance of the meatus, extending form the 3-o’clock to the 5-o’clock positions. The mastoid cortex is exposed, and the retracted soft tissue is held in place by four retractors. In the tympanic cavity, the denuded bone of the medial part of the ear canal is illustrated (arrows)
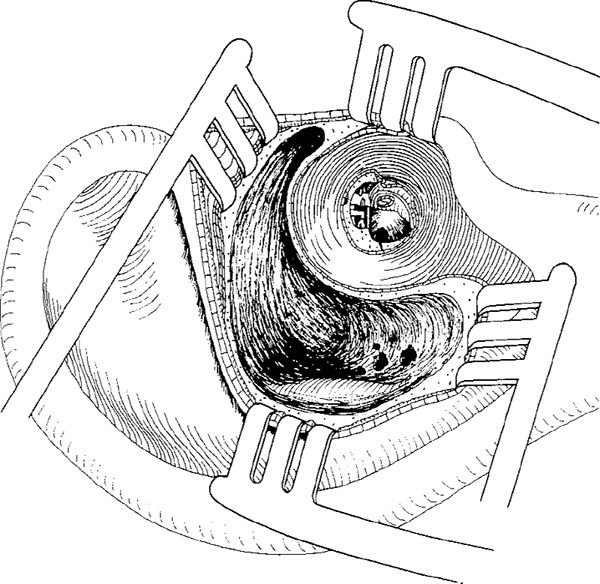
Fig. 493 Intact canal wall mastoidectomy is performed. The bony ear canal is thinned maximally all the way around as far as the anterior attic, and the ear canal skin is attached to the lateral half of the bony ear canal

Fig. 494 A superior osteotomy is performed far anteriorly toward the zygomatic root, using a small sharp burr

Fig. 495 An inferior osteotomy is performed
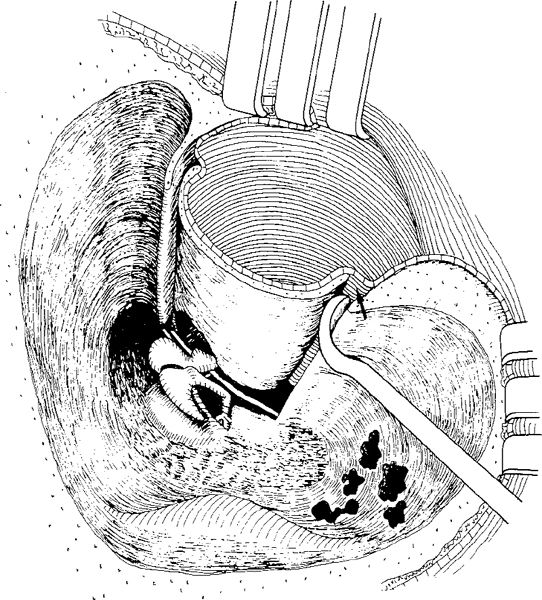
Fig. 496 With a curved rugine, the periosteum and the ear canal skin are carefully elevated along the osteotomies, maintaining the canal skin intact (arrow). Superiorly, the ear canal wall is rotated clockwise, opening the anterior attic
Initially, Schnee (1963, 1964) used an endaural approach with a plastic tube inserted into the mastoid cavity and brought out through the endaural incision. Later, he changed the method, and preferred a retroauricular approach (Schnee 1969) that avoided the transmeatal atticotomy whilst maintaining the attachment of the tympanic membrane and ear canal skin to the mobilized bony ear canal.
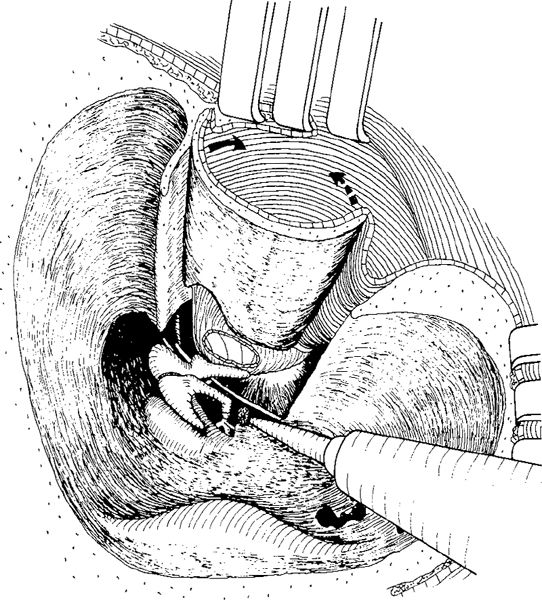
Fig. 497 The entire ear canal wall is displaced anteriorly, exposing the malleus handle and the drum. The ear canal can be rotated clockwise (solid arrow) if a larger space is desired superiorly, or anticlockwise (dashed arrow) if the hypotympanum has to be exposed. The bone from the facial recess, medial to the preserved chorda tympani, is removed to enlarge the exposure of the tympanic sinus
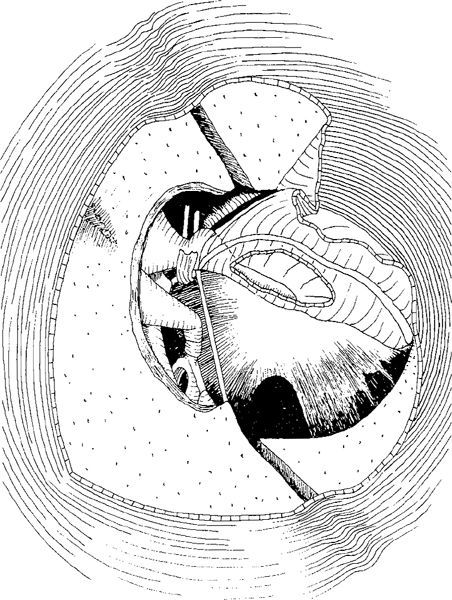
Fig. 498 The transmeatal view of the replaced ear canal wall, illustrating the bone defects caused by drilling and the areas with elevated skin
Posterior Wall Displacement
After transmeatal clearing of cholesteatoma from the tympanic cavity and deepithelialization of the drum remnant, as well as removal of the margins of the perforation, without elevating the canal skin a simple atticomastoidectomy is performed through a retroauricular approach (Lapidot and Brandow 1966). The posterior bony ear canal wall is thinned, and the incus body and the short process of the incus, the posterior buttress, the lateral semicircular canal and the facial nerve are located (Fig. 500). Holes are drilled in the ear canal wall for the superior and inferior osteotomies, using a small cutting burr. The superior vertical osteotomy is made below the level of the superior buttress, starting at the lateral free margin of the bony ear canal. A similar, parallel, inferior osteotomy is made at the level of the floor of the external bony ear canal. These two vertical osteotomies are then connected by a horizontal osteotomy, approximately 1-2 mm lateral to the facial ridge. The isolated bony ear canal wall is carefully elevated and pushed anteriorly, together with its attached ear canal skin and the annulus of the tympanic membrane, leaving the posterior part of the bridge intact (Fig. 501). The ear canal skin and the mobilized bony ear canal wall must be held in place by a selfretaining retractor with a long blade. After the cholesteatoma removal and underlay fascia grafting of the perforation are complete, the bony ear canal wall is replaced and the ear canal is packed.
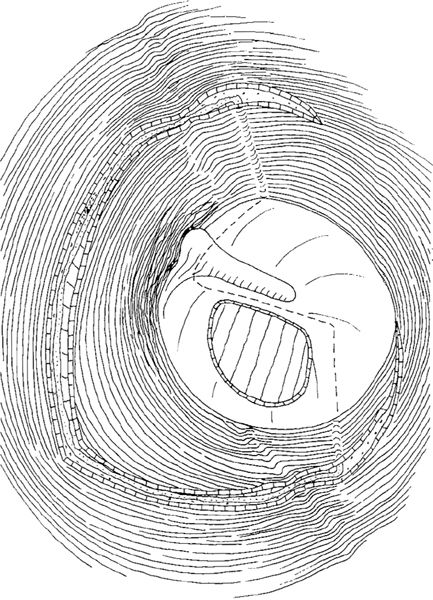
Fig. 499 The fascia or vein covers the perforation, and the exposed bony ear canal wall, with the osteotomy grooves and the ear canal skin flaps are replaced
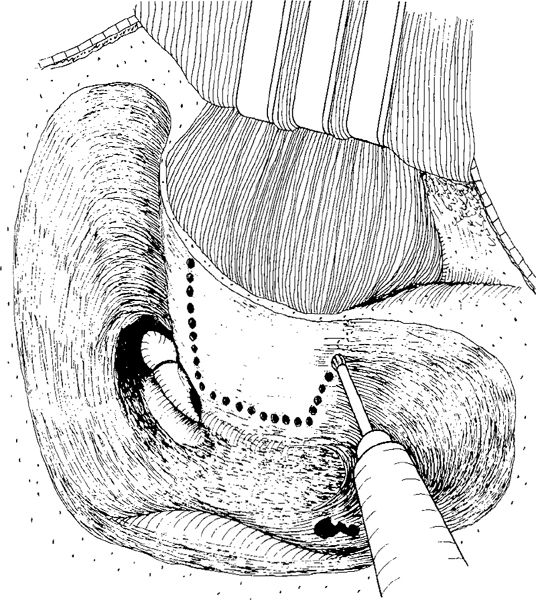
Fig. 500 The posterior wall displacement (Lapidot and Brandow). After an intact canal wall mastoidectomy in a retroauricular approach without opening the ear canal skin, the thinning of the bony ear canal wall, expecially its posterior part, is performed. Small holes are made in the bony ear canal wall, indicating the superior, inferior, and horizontal osteotomies. The superior osteotomy is performed at the level of the posterior buttress, the inferior at the bottom of the ear canal, and the horizontal about 1-2 mm lateral to the facial nerve, which is partly skeletonized

Fig. 501 The osteotomies have been completed, and the posterior ear canal wall has been displaced anteriorly, together with the intact ear canal skin attached to the mobilized bony ear canal wall. Also, the fibrous annulus is displaced anteriorly, exposing the ossicular chain and partly the posterior part of the tympanic cavity. By drilling the bone within the facial recess using a diamond burr, the posterior tympanum can be further exposed
Mobilization of the posterior ear canal wall provides good exposure of the promontory, hypotympanum, and the anterior tympanum, but the posterior tympanum with the tympanic sinuses is not satisfactorily exposed, because the horizontal osteotomy is 1-2 mm lateral to the facial ridge. Further bone removal from the facial recess (Fig. 501) and around the chorda is necessary to obtain a sufficient viev of the tympanic sinuses. The Lapidot method is, in the present author’s opinion, only suitable for sinus cholesteatoma, because the superior osteotomy is made below the posterior buttress, and the superior part of the ear canal is not mobilized at all. In cases of attic cholesteatoma, this method cannot be used, since the anterior attic is not opened. The anterior attic can in fact be approached “transmeatally” after the bony ear canal has been displaced anteriorly (Fig. 501), but then the philosophy of the completely intact ear canal is lost, and a scutumplasty is difficult to perform.
Richards’ Mobile Bridge Technique
Richards (1972) recognized the difficulties of the Schnee technique with the elevation of a large tympanomeatal flap (Figs. 490, 491), which leaves very little of the canal skin attached to the mobilized bony ear canal. For this reason, Richards does not start transmeatally, and keeps all the canal skin attached to the mobilized bony ear canal and bridge. He also performs a posterior atticotympanotomy through the facial recess, as well as a transmastoid anterior atticotympanotomy.
Richards performs the mastoidectomy with a retroauricular approach, thinning the bony ear canal wall anteriorly to expose the extreme anterior portion of the attic. The incus and malleus are located, and the posterior atticotympanotomy is performed in the usual manner, removing the posterior buttress (Fig. 502). After a superior and an inferior osteotomy using a small cutting burr, the bony ear canal with the bridge is mobilized, but the attachment to the ear canal skin anteriorly is retained (Fig. 503). The mobilized bridge is then displaced anteriorly, exposing the middle ear space (Fig. 504).
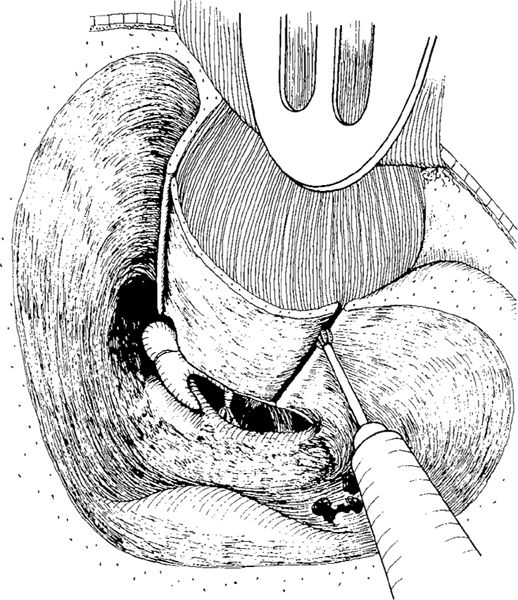
Fig. 502 Richards’ mobile bridge technique. In the retroauricular approach preserving the entire canal skin attached to the bony ear canal wall, an intact canal wall mastoidectomy is performed by thinning the posterior canal wall far anteriorly, exposing the anterior attic, and performing a posterior atticotympanotomy with removal of the posterior buttress. The long process of the incus and the stapes are exposed. The superior osteotomy, starting anterior to the head of the malleus, and the inferior osteotomy, starting at the 8-o’clock position lateral to the chorda tympani, are performed with a small cutting burr
After the tympanic and the mastoid cavities have been cleared of cholesteatoma and after ossicular reconstruction, the perforation is closed with an underlay fascia graft, and the mobilized bridge is replaced and kept in position by a gauze pack placed in the external ear canal (Fig. 505). The reconstructed ossicular chain is inspected through the posterior atticotympanotomy. The posterior end of the fascial graft is brought into the mastoid cavity through the posterior atticotympanotomy, and is then placed on the posterior surface of the bony bridge. In this position, it is supported by Gelfoam balls placed on the mastoid surface of the bony ear canal wall (Fig. 506).
Richards reported the following complications among 76 consecutive cases: two cases with temporary facial palsy, two with bone breakdown, and one with ear canal stenosis. In two ears with extensive spontaneous erosion of the ear canal wall, the mobile bridge technique was not possible. Late results in 40 cases with at least 18 months of observation time showed cholesteatoma in one case, otorrhea in three cases, and retraction pockets in five cases, but none were severe.
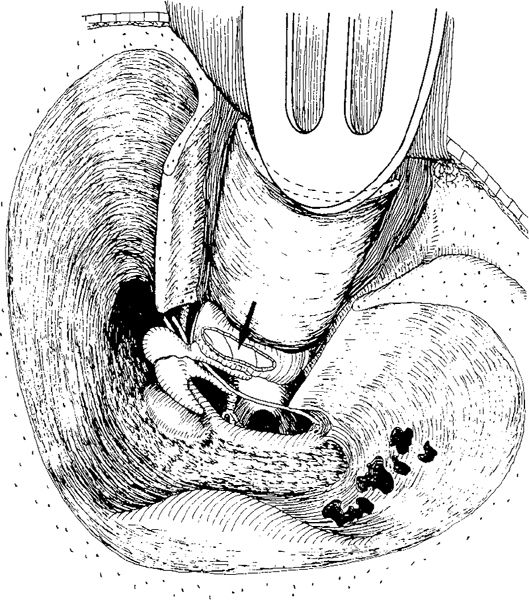
Fig. 503 The bony ear canal wall is mobilized and pushed anteriorly after the canal skin has been detached from the bony ear canal, close to the osteotomies. Together, with the ear canal wall, the fibrous annulus and the drum remnant are also mobilized, exposing the posterior perforation (arrow), the ossicles, the posterior tympanum, and the attic

Fig. 504 Side view of Richards’ mobile bridge technique. The mobilized bony ear canal wall is anterior displaced and held in place with the protective blade of a selfretaining retractor. The medial part of the bony ear canal is connected to the ear canal skin and the drum remnant. Good exposure of the attic and the tympanic cavity is illustrated

Fig. 505 Side view of the repositioned bony ear canal wall, placed back in its original position. The ossiculoplasty is performed with a shaped autogenous incus, placed under the malleus handle and the fascia. The temporalis fascia, as an underlay graft, is placed behind the bony ear canal wall (arrow) and held in place with some Gelfoam balls
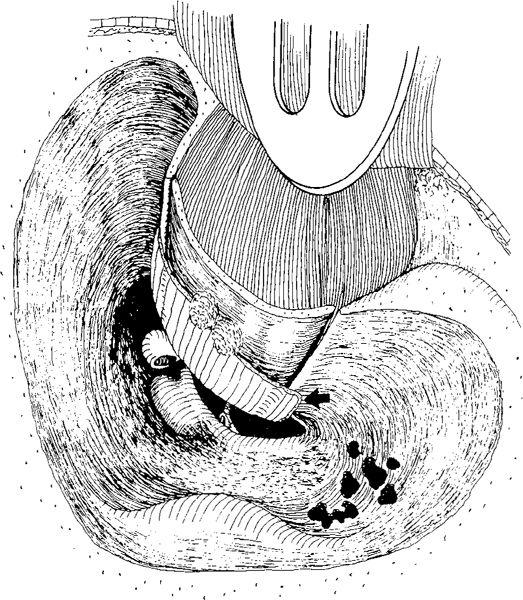
Fig. 506 Replaced bony ear canal wall, supported by the fascia folded around the medial edge of the ear canal and fixed on its mastoid aspect with Gelfoam balls (arrow)
Temporary Removal of the Bony Ear Canal Wall
The methods using temporary removal of the ear canal have partly replaced displacement techniques, because they are easier to perform and can provide better exposure of the anterior part of the tympanic cavity and Eustachian tube orifice. In addition, surgeons are more familiar with the approach, including elevation of the ear canal skin. Lastly, there is the possibility of better fixation of the replaced bone, which contributes to the popularity of these methods.
Temporary Meatotomy
Gerlach (1969a) was the first to remove the bony ear canal wall in cases with extensive cholesteatoma. He called his method “temporary meatotomy.” The ear canal skin, with the fibrous annulus and the drum remnant, were elevated from the bony canal wall. After osteotomies and removal of the bony ear canal wall, an excellent view of the cholesteatoma is achieved, and it can be removed in toto. After replacement, the bony ear canal wall is supported by a superiorly pedicled fascia–muscle flap from the temporalis muscle (Gerlach 1969b) (Fig. 507). Gerlach (1970) fixed the ear canal wall with Histoacryl glue, and homogenous bone paté was placed in the osteotomy grooves. However, in several cases he observed retraction of the replaced canal wall, with formation of defects in the meatal side of the ear canal — a stair-like formation — similar to the complication seen after longitudinal temporal bone fracture with dislocation running through the ear canal.
Osteoplastic Epitympanotomy (S. Wullstein)
With the introduction of osteoplastic epitympanotomy, Sabina Wullstein (1972, 1973, 1974) caused a resurgence of interest in temporary removal of the bony bridge. The principle of this technique has been described here earlier (Vol. I, Chapter 5) together with a description of the superior approach, which is a characteristic feature of the superior epitympanotomy (Vol. 1, Figs. 159–161). Through maximal widening of the superior bony ear canal, a bony plateau is elaborated, extending from the bony annulus inferiorly to the middle fossa dural plate superiorly. With further drilling of the lateral wall of the attic and thinning of the roof of the bony meatus close to the middle fossa dural plate (Vol. 1, Fig. 162), the lateral attic wall is maximally thinned. The drilling is extended further medially and anteriorly at the zygomatic root, making the bony plate that is about to be removed as large as possible and exposing the entire anterior attic. Using a small diamond burr, a groove is created (Vol. 1, Fig. 163), the bony plate is elevated, and the lateral attic as well as the superior and posterior tympanum are thus exposed. Precise surgery in the anterior attic, and especially the creation of a ventilation route through the epitympanic sinus to the Eustachian tube, is possible and easy to perform (Vol. 1, Fig. 166).
Removal of an attic cholesteatoma located in the lateral attic, preserving the ossicular chain intact, can be performed in a similar way to that described in Chapter 7. above with elevation of the cholesteatoma membrane from the lateral aspects of the incus body and head of the malleus, and cleaning of the anterior attic. In cases with a defective long process of the incus, the incus is removed, and the cholesteatoma can be removed from around the malleus head, preserving it intact — of course, as long as there is no invasion of cholesteatoma into the ossicle.
In cases with cholesteatoma extending onto the medial surface of the incus and malleus head, the incus body has to be removed, and sometimes even the malleus head has to be resected, but in the superior approach the chance of cleaning the ossicles in the attic is optimized.
In sinus cholesteatoma, defined as a posterosuperior retraction involving the tympanic sinuses and the stapes, the cholesteatoma removal is relatively easy and safe, because the removal of the posterior bony annulus (otosclerosis drilling) can be extended in order to totally visualize the lateral and the medial sinuses. The view of the stapes and the footplate region is similarly good in the superior approach. In cases with an eroded incus, the cholesteatoma may extend medial to the incus body, but it can be removed safely after removal of the incus body and cleaning of the medial attic.
In tensa retraction cholesteatoma involving the entire tympanic cavity with retraction and adhesion of the entire pars tensa, or a total perforation, there is a good view of the tympanic cavity with the superior approach after the ear canal has been opened (Fig. 508). The cholesteatoma membrane is easily elevated, starting superiorly and continuing down to the annulus.

Fig. 507 Gerlach’s temporary meatotomy. After an intact canal wall mastoidectomy and superior and inferior osteotomies using small burrs, the bony ear canal has been removed and the cholesteatoma has been removed, leaving a total perforation, an intact malleus, and an intact stapes. The bony ear canal wall is replaced in its original position and glued from behind with Histoacryl glue, or nowadays replaced with lonomer cement (dark spots). The bony ear canal is supported by a superiorly pedicled fascia–muscle flap placed behind the ear canal wall. The defects after the osteotomies are filled with homgenous bone paté (arrows)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


