Fig. 731 The two Preysing full-thickness skin grafts. After two parallel retroauricular incisions, the skin pedicles are liberated and cleaned of subcutaneous tissue. The dashed lines indicate the position of the mastoid cavity and the tympanic cavity
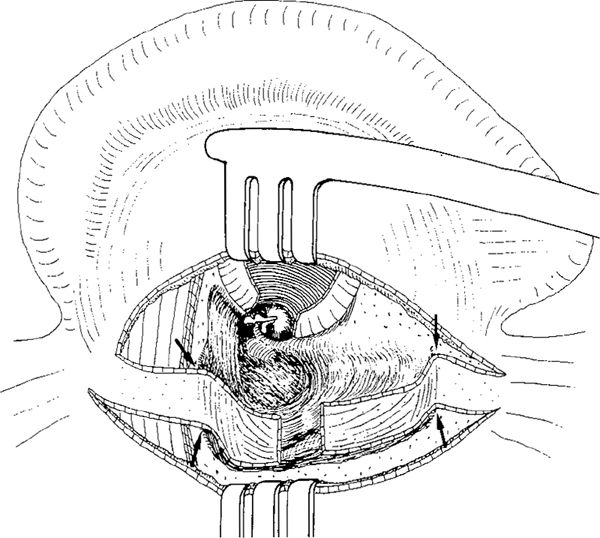
Fig. 732 The canal wall–down mastoidectomy cavity covered with two pedicled skin flaps. The edges of the cavity are rounded (arrows) to avoid disturbance to blood circulation in the flaps
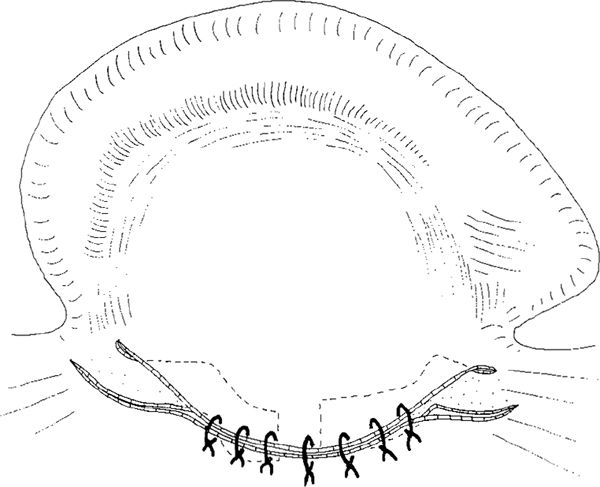
Fig. 733 The postauricular incision is closed, except inferiorly and superiorly. The bases of the flaps will be cut 14 days later, and the wounds sutured secondarily at the same time
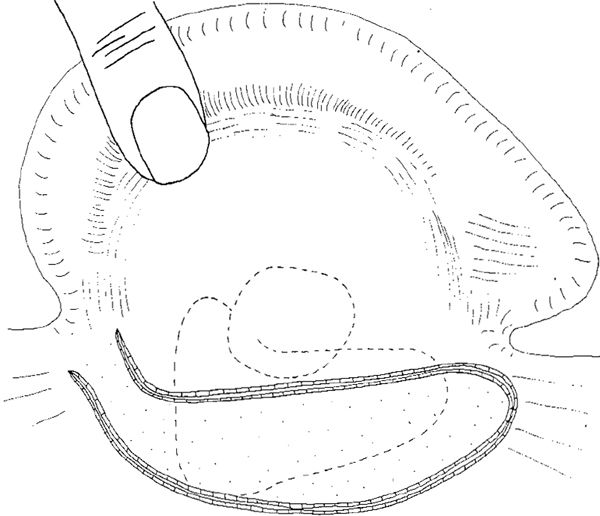
Fig. 734 Incision for a superiorly-based skin flap
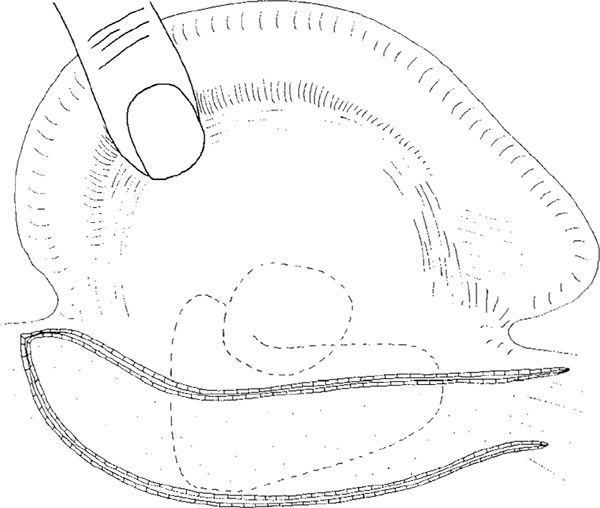
Fig. 735 Incision for an inferiorly-based skin flap
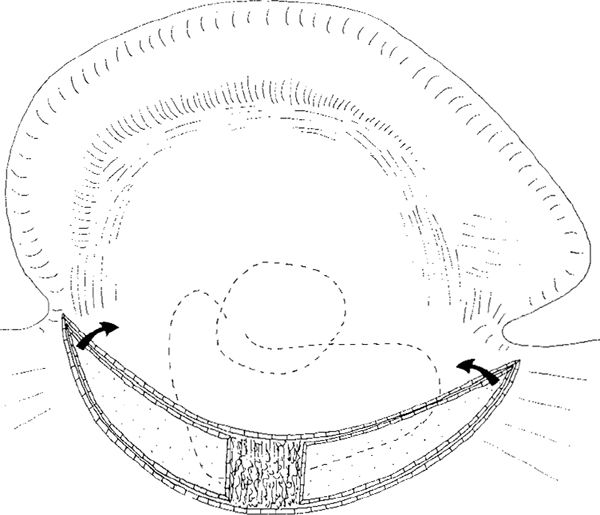
Fig. 736 The original Mayer skin–subcutis pedicled grafts. Two parallel skin incisions are made, going through the skin, subcutaneous tissue, and periosteum. In the central part of the flap, skin is removed. The flaps will be inserted with their conical ends (arrows) into the cavity
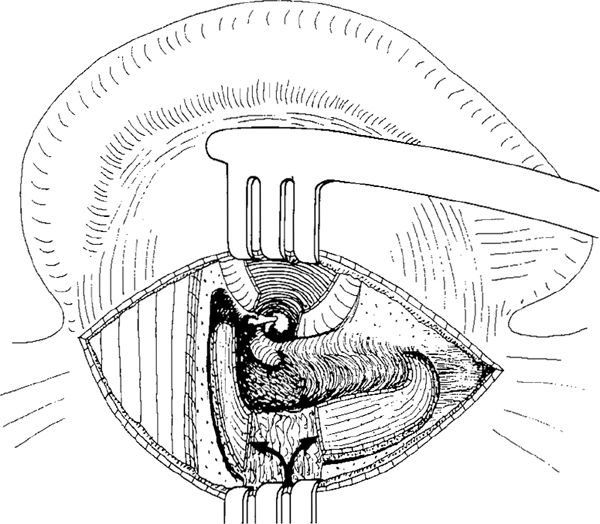
Fig. 737 The skin–subcutis flaps are in position in the cavity. One is covering the superior wall, and the other the posteroinferior wall. The vascular supply to the flaps comes through the pedicled subcutaneous tissue (arrows)

Fig. 738 The Beales and Hynes posteriorly bases skin–subcutis flap. The incision goes through the skin and the subcutaneous tissue down to the perichondrium
Beales and Hynes (1958) published an interesting method using a large, posteriorly-based skin–subcutis flap. After a skin incision on the posterior aspect of the pinna, passing through the subcutis to the surface of the perichondrium (Fig. 738), the flap is elevated and turned backward, exposing the mastoid bone (Fig. 739). After a canal wall–down mastoidectomy, a small Körner flap is created and sutured to the posterior aspect of the ear canal and the pinna. Superiorly and inferiorly, the skin–subcutis flap is sutured to the Körner flap, holding the Körner flap in position (Fig. 740). A thin layer of the epithelium is scraped off the pedicle of the postauricular flap with a knife. This shaved surface is about 0.5 cm wide, and is sutured to the subcutaneous tissue of the concha. These sutures hold the ear canal wide, and keep the Körner flap attached to the posterior border of the cavity. Finally, the posterior surface of the pinna is covered with a large split–skin graft, sutured to the skin edges (Fig. 741). Beales (1959) reported the one–year results in 44 patients using this method. Eighty-four percent of the ears remained dry, with healed cavities, and only five percent of the cavities had small unhealed areas requiring occasional outpatient treatment.
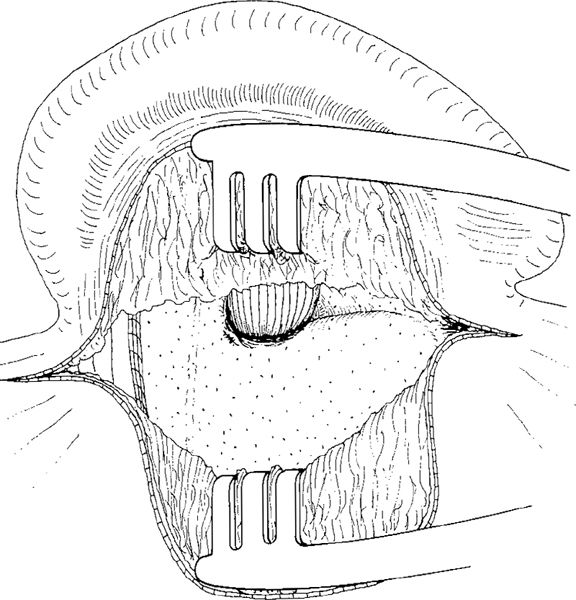
Fig. 739 The subcutis–skin flap is elevated, exposing the cortical bone of the mastoid plane. The ear canal skin is not opened

Fig. 740 After a canal wall–down mastoidectomy, the posteriorly-based subcutis-skin flap is pressed into the cavity. It is sutured to the inferiorly and superiorly-based ear canal skin flaps. A Körner flap from the posterior wall of the ear canal is sutured to the posterior aspect of the ear canal and the pinna. Posteriorly, a 0.5–cm wide strip of skin is excised or scraped using a scalpel, allowing primary suturing of the wound

Fig. 741 The Körner flap, together with the tissue covering the mastoid process, is sutured to the base of the subcutis-skin flap at the region of removal of the epithelium (1). The superior and inferior parts of the skin are sutured (2), the large skin defect of the pinna is covered with a large split-skin graft sutured to the edges of the wound (3), and finally the split–skin graft is adapted to the edge of the skin in the postauricular fold (4)
Some of the pedicled skin–subcutis grafts have also been used to obliterate the cavity. Grahne’s superiorly-based epithelial–subcutis flap (1963), using a similar incision as the Vincencio and Gundersen flaps (Fig. 734), includes all the postauricular subcutaneous tissue and the temporalis muscle. Distally, the flap even includes fibers of the sternocleidomastoid muscle, and if necessary this flap can be made relatively thick. After an endaural canal wall–down mastoidectomy (Fig. 742), the pre-prepared flap is pulled into the cavity, covering and obliterating the upper part of the cavity. The lower part is covered with a inferiorly-pedicled meatal skin flap. The postauricular skin is closed primarily, except at the very top part. The vital pedicle is cut one month after primary surgery, and the upper part of the incision is then closed.
Most methods are based on secondary cutting of the flap after it has healed onto the cavity wall. Some surgeons cut the skin base one month, some two or three months after primary surgery (Charland 1960). In the Beales and Hynes method, a strip of skin is cut at primary surgery, and the incision is closed primarily.
Richtner (1960) used a double inferior pedicled flap (Fig. 743). The anterior flap is a skin flap to cover the tympanic cavity and attic. The posterior flap is a periosteum–muscle–skin flap, covering the inferior part of the cavity behind the facial ridge (Fig. 744).
In the conservative radical operation preserving the bridge, the skin flap covers the facial ridge, the attic, and the tympanic cavity, creating a myringostapediopexy or type 4 tympanoplasty. The muscle flap covers the antrum and the mastoid tip (Fig. 745). The posterior incision is closed primarily.
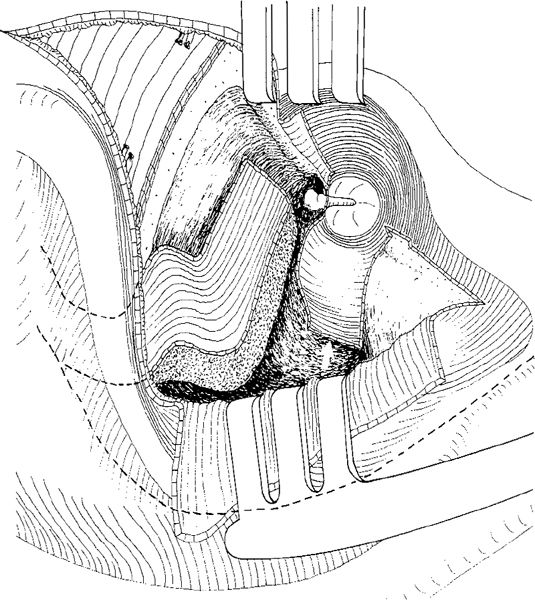
Fig. 742 The Grahne pedicled full–skin subcutis–muscle flap after two postauricular incisions. The flap is elaborated using a postauricular incision. It consists of skin, subcutis, and muscle fibers up to the periosteum. After an endaural canal wall–down mastoidectomy, the flap is pulled into the cavity, covering its superior part. Interiorly, a large ear canal skin flap is covering the cavity and the facial ridge (arrow)

Fig. 743 The Richtner double inferiorly–based flaps. The incisions for the two flaps are made through the skin and subcutaneous tissue

Fig. 744 The anterior flap is cleaned of subcutis. At the base of the flaps, the skin is removed
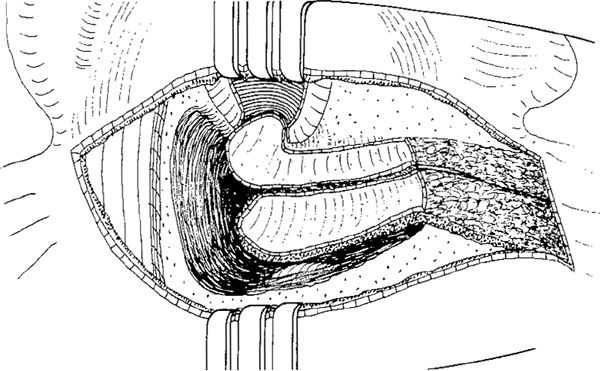
Fig. 745 The skin flap is placed on the drum perforation and on the facial ridge. The posteriorly-positioned skin–subcutis flap is obliterating and covering the inferior part of the cavity. The wound is closed primarily
Pedicled Ear Canal Skin Flaps
The ear canal skin flaps are the most important factors in the healing and epithelialization of an open cavity. Creation of ear canal skin flap has sometimes already occurred during the approach to the ear canal and tympanic cavity. During the approach, the ear surgeon should already have an idea of how to reconstruct the ear canal wall if the mastoidectomy should end up as a canal wall–down mastoidectomy, and flaps are the cornerstone of this reconstruction. In Volume 1, the many types of ear canal skin flap are illustrated for the endaural and retroauricular approaches in myringoplasty and tympanoplasty. Here, only the supplementary surgery of the flaps in relation to a canal wall–down mastoidectomy will be indicated.
Generally, there are three main types of ear canal skin flap. These are:
1. The laterally-based Körner flap (Fig. 659).
2. The medially-based Surdille flap (Figs. 660–662).
3. The inferiorly-based Stacke flap or Panse flap.
The level and location of the various ear canal skin incisions determines the size of the flap.
The Körner Flap
The Körner flap is based laterally, and provides the covering and the source of epithelialization for the posterior aspect of the cavity.
The Körner flap in an endaural approach. In the Heermann B modification of the endaural approach (Fig. 659) the radial incisions are placed at the 12-o’clock and 6-o’clock positions, and a circumferential incision connects the two radial incisions, dividing the posterior ear canal skin into a medial and a lateral flap (Fig. 746). The elevated lateral flap of ear canal skin is the distal part of the Körner flap, which can be extended during the meatoplasty. The medially-based tympanomeatal flap can be of varied size, again depending on the position of the circumferential incision. If the incision is placed laterally, as in Shambaugh’s and Lempert’s modifications, the Körner flap is small but the tympanomeatal flap is large, and in such cases it is called the Surdille flap (Figs. 660, 661).
In the Heermann B incision, the superior ear canal skin flap is small, but it can be enlarged by a separate skin incision placed anteriorly in the ear canal at the 3-o’clock position. This flap is based medially, and can cover the superior wall of the cavity (Fig. 746). Medially, the tympanomeatal flap covers the medial wall of the posterior attic, aditus and antrum and antrum, and part of the facial ridge.
For reconstruction in a canal wall–down mastoidectomy, the Körner flap is created at the end of the procedure, during the meatoplasty. Two radial incisions of about 1 cm each are made through the conchal skin and cartilage from the edge of the ear canal towards the cavum conchae (Fig. 746). The Körner flap is elevated laterally from the conchal cartilage using a pair of scissors, exposing a 0.5 to 1.0 cm–wide strip of the medial part of the conchal cartilage, which is then excised, enlarging the ear canal and elongating the Körner flap (Fig. 747).
The Körner flap is pushed posteriorly into the cavity, covering the posterior aspect of the cavity (Fig. 748). In an endaural approach, it is held in place by a strip of gauze moistened with hydrocortisone and Terramycin ointment. Superiorly, the anterosuperior flap covers the attic and tegmen tympani, and inferiorly, the tympanomeatal flap covers the aditus ad antrum (Figs. 748, 749).
The Körner flap in a retroauricular approach. To achieve a long and rectangular Körner flap in a retroauricular approach, the Wullstein–Kley technique is used, with radial incisions at the 12-o’clock and 6-o’clock positions and a relatively medially placed circumferential incision (Vol. 1, Figs. 96–105, 108–110). The flap is elevated and held in place during canal wall–down mastoidectomy by a self-retaining retractor (Fig. 615). After completion of the canal wall–down mastoidectomy, the meatoplasty is performed, elongating the radial incisions at the 6-o’clock and 12-o’clock positions up to the conchal cartilage (Fig. 750). The selfretaining retractor is then repositioned, the fibrous tissue from the posterior aspect of the conchal cartilage removed, and the cartilage exposed. Using a knife, a 1-cm–broad strip of cartilage is excised and separated from the perichondrium using a rugine (Fig. 751). The Körner flap is thus elongated, and the ear canal widened. Along with the auricle, the Körner flap is then pulled posteriorly and sutured to the subcutaneous tissue at the posterior edge of the cavity. The flap is carefully adapted to the posterior wall of the cavity (Fig. 752). Medially, the meatal skin flaps are replaced posteriorly over the fascia, partly covering the facial nerve, the lateral semicircular canal, and the medial wall of the attic, as well as the tegmen tympani superiorly. The cavity is filled with Gelfoam and moistened with antibiotic, and a strip of gauze moistened with hydrocortisone and Terramycin ointment, is left in place for three weeks.
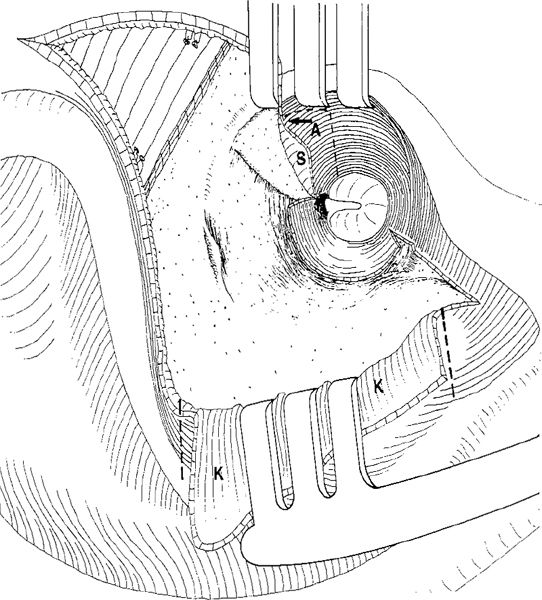
Fig. 746 The Körner flap in an endaural approach. The Heermann B incision, illustrating the laterally-based Körner flap (K), which can be enlarged using incisions through the conchal skin and conchal cartilage (dashed lines). Medially, a tympanomeatal flap is left, and superiorly, a small superior flap (S), which can be enlarged by two separate incisions in the anterior ear canal wall (A) and placed on the tegmen tympani (arrow)
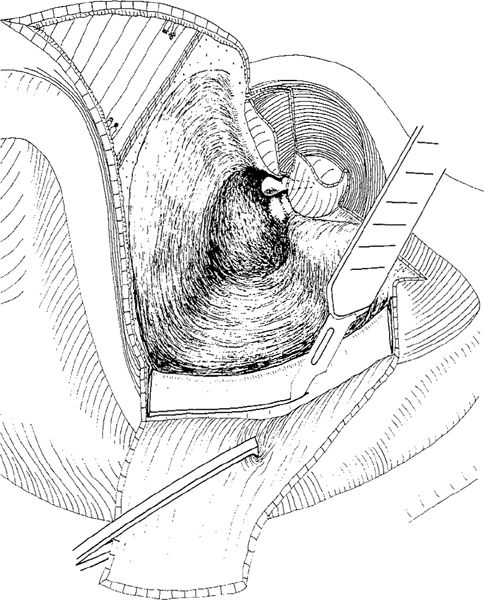
Fig. 747 The meatoplasty in an endaural approach enlarging the Körner flap. The conchal canal skin is elevated, and a 0.5–cm wide strip of the conchal cartilage is excised in a canal wall–down mastoidotomy situation with a preserved malleus head and elevated tympanomeatal flap

Fig. 748 Reconstruction of an endaural canal wall–down mastoidectomy using the Körner flap, which covers the posterior part of the cavity. Superiorly, a superoanterior skin flap is covering the attic (SA), and medially, a tympanomeatal flap (TM) is covering the aditus ad antrum
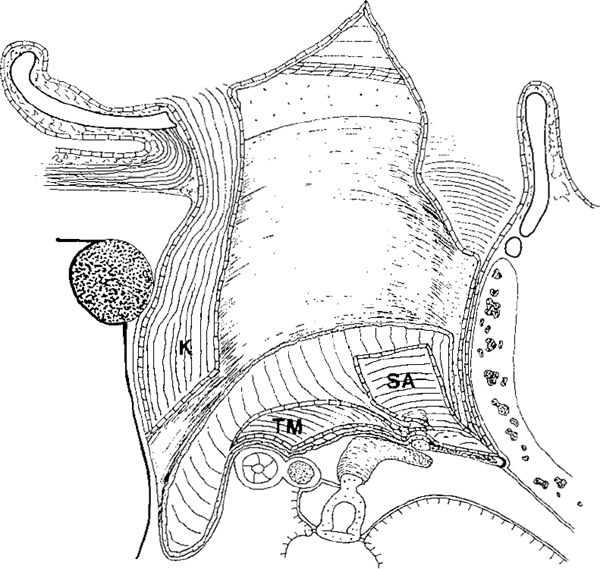
Fig. 749 Side view, with some perspective, of an endaural canal wall–down mastoidectomy, showing the placement of the Körner flap (K) on the posterior wall of the mastoid cavity. The medial wall is covered by fascia and the tympanomeatal flap (TM), as well as the superoanterior flap (SA)

Fig. 750 Creation of the Körner flap in a retroauricular canal wall–down mastoidectomy. The medial part of the Körner flap is elevated, and the radial incisions at the 6-o’clock and 12-o’clock positions are extended into the conchal cartilage

Fig. 751 Meatoplasty in a retroauricular canal wall–down mastoidectomy with preparation of a Körner flap. On the posterior aspect of the ear canal, the fibrous tissue is removed, the conchal cartilage is exposed, and a strip of conchal cartilage 0.5–1.0 cm wide is excised and elevated from the perichondrium using a Freer rugine
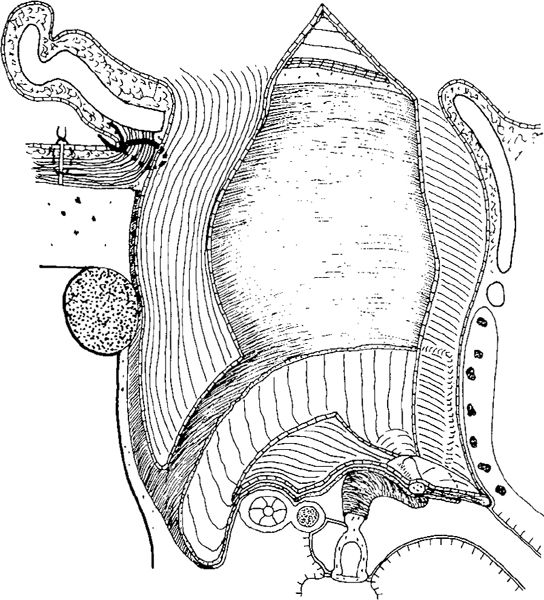
Fig. 752 Side view, with some perspective, of the position of the Körner flap in a retroauricular canal wall–down mastoidectomy. The auricle is pushed posteriorly, and the Körner flap is adapted to the posterior wall of the cavity and sutured to the auricular fibrous tissue with a relatively thick catgut suture
The Surdille Flap
The medially-based Surdille flap is the flap usually used in an endaural approach, and is described in Volume 1, Chapter 3. If a circumferential incision in the Heermann B, Lempert, Shambaugh, or Farrior modifications of the endaural approach is placed laterally, then a large Surdille flap is created, involving the entire posterior ear canal skin (Figs. 659–662). The Shambaugh and Lempert incisions run laterally at the level of the suprameatal spine, and the lateral part of the ear canal skin, the conchal canal skin flap, or the Körner flap, are therefore not present (Figs. 660, 661). In Farrior’s endaural incision, however, the Surdille flap is somewhat smaller (Fig. 662); the conchal canal skin flap, on the other hand, is relatively large. In fact, Farrior performed his meatoplasty by excising a small strip of conchal cartilage at the beginning of the surgery. The Farrior meatoplasty is based on a conchal skin flap (a small Körner flap), which is enlarged by excision of the cartilage and creation of a subcutaneous tissue flap (Vol. 1, Figs. 58–60).
By adding a radial incision, the Surdille flap can be divided into an inferior and a superior half. The superior half covers the attic (Fig. 753), and the inferior half covers the facial ridge.
The Stacke Flap
The Stacke flap is inferiorly based, and consists of posterior ear canal skin and a strip of the conchal cartilage. The Stacke flap is performed using a retroauricular approach, making a radial incision at the 12-o’clock position, a medial circumferential incision 2–3 mm lateral to the drum, and a lateral circumferential incision through the conchal cartilage (Fig. 754). The conchal cartilage is removed, and the Stacke flap covers the entire facial ridge and the inferior part of the cavity (Fig. 755).
In an endaural approach, the Stacke flap does not include the conchal cartilage (Chapter 9, Figs. 533, 537, 539, 541, 543–546). The ear canal skin is thick laterally, and has to be thinned in order to be adapted to the cavity wall.
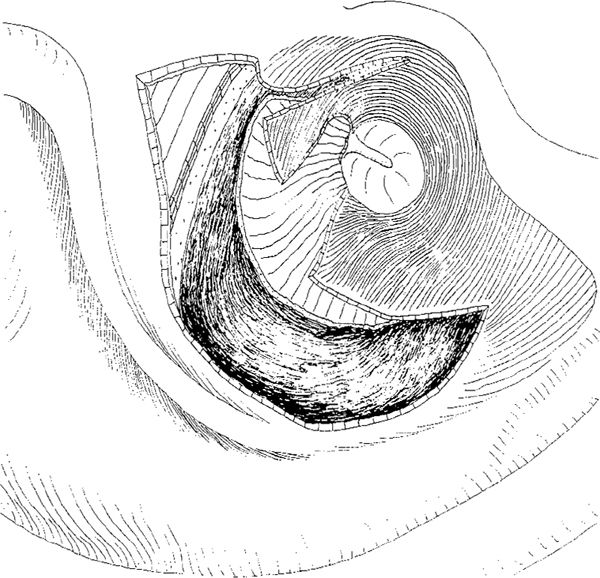
Fig. 753 The Surdille flap divided into two parts in endaural canal wall–down mastoidectomy using a Shambaugh incision. The inferior part of the flap covers the facial ridge, and the superior part covers the anterior attic
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


