Fig. 991 Harvesting strips of cancellous bone from the iliac crest (Schiller): a After incision along the iliac crest, a lid of the iliac crest is chiseled and lifted. Cancellous bone is visible. Using a chisel, two vertical cuts are made along the outer cortical layer. b Cortical bone from the posterior side of the iliac crest is chiseled and pulled down, exposing the cancellous bone layer
The harvested cancellous pieces of bone are stored in a solution containing antibiotics during the operation. After a canal wall–down mastoidectomy with preservation of as much of the ear canal skin as possible and creation of superior and inferior ear canal skin flaps, the strips of iliac bone are trimmed and adapted to the size of the cavity (Fig. 994). The strips of cancellous bone are placed either vertically or horizontally in the depths of the cavity. The first level of strips is placed over the lateral semicircular canal, behind the facial ridge. The second level of strips is arranged in a similar way (Fig. 995), and placed first meatally, creating a bony ear canal wall, and then in the remaining cavity. Further obliteration is carried out using either horizontal or vertical bone strips (Fig. 996). The tympanomeatal skin flaps are placed on the attic wall superiorly and inferiorly, to encourage further epithelialization of the posterior ear canal wall. A modified Körner flap hangs down in a curtain-like manner to cover the lateral part of the posterior bony ear canal wall. Inserting too many strips of bone should be avoided, since it may result in narrowing of the external auditory canal.
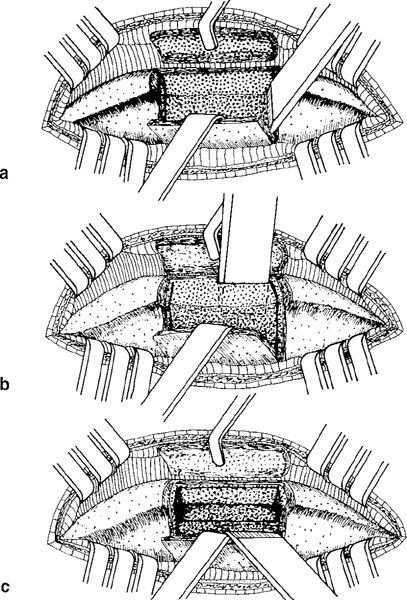
Fig. 992 a, b Removal of the strips of cancellous bone using a sharp, flat chisel. c Several strips of bone are removed

Fig. 993 The lid is replaced, and the incision is sutured
Initially, covering the bone with fascia was not generally performed. Currently, this technique can be performed by placing fascia as an underlay graft covering the meatal part of the new ear canal, or even using tragal cartilage. For lateral covering, a Palva flap can be used (Fig. 997). Larger interstices between the bone strips can be filled with autogenous bone paté.
This obliteration method was used by Schiller in the fenestration operation, and in such cases, of course, the bony strips have to be placed posterior to the fenestrated lateral semicircular canal. In 32 cases observed for a period of 8–12 months postoperatively, 22 proved completely successful with total obliteration of the cavity. In one case, the skin covering was incomplete. It was shown that the cancellous bone graft had been replaced by new bone, i. e., it had integrated with the mastoid bone. Schiller described the following advantages of his technique: 1) complete obliteration, 2) restoration of the contour of the mastoid bone and the external auditory canal, and 3) reduction of postoperative treatment to a minimum.
The only fair criticism of Schiller’s technique is the need to harvest bone from the iliac crest, resulting in pain and morbidity. The fact that the patient needs to remain in bed for 14 days is probably the reason why this procedure has never become popular worldwide.

Fig. 994 Mastoid osteoplasty with iliac crest cancellous bone (Schiller). After canal wall–down mastoidectomy, four strips of cancellous bone of various sizes are placed vertically on the medial wall of the cavity

Fig. 995 The second layer of cancellous bone strips is placed vertically on the first layer
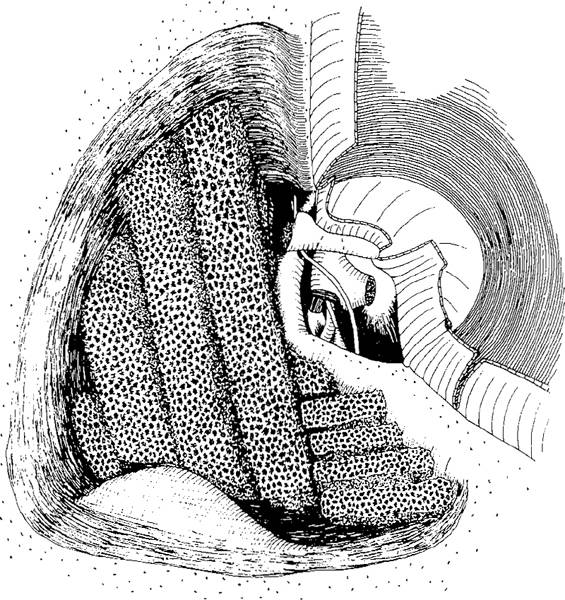
Fig. 996 The third and the fourth layers of bone are placed in the lateral part of the cavity. Some strips are placed in a vertical direction, some in a horizontal one

Fig. 997 Side view of the obliteration with iliac crest cancellous bone, showing the position of the bony strips. The fascia covers the meatal side of the strips, and laterally Gelfoam, a subcutis–muscle flap, and the periosteum cover the bone. The ear canal is somewhat widened. The fascia goes down onto the facial eminence, but it could also run directly onto the bone (dashed), leaving more of the attic ventilated. The incus is interposed
Tibial Crest Cancellous Bone
Filipo and Barbara (1986, 1988) have used autogenous cancellous bone taken from the tibial crest using a trocar (Fig. 998). After reconstruction of the tympanic cavity and packing of the ear canal, the tympanic cavity is separated from the mastoid cavity by a large roll of Silastic. Spongioform bone from the tibia mixed with fibrin glue is placed behind the roll. The spongy bone is covered with fascia, and the epithelial flaps from the radical cavity are replaced.
Additional reconstruction of the ear canal with autogenous cartilage and a Palva flap is needed in this method in order to separate the bone chips from the canal skin.
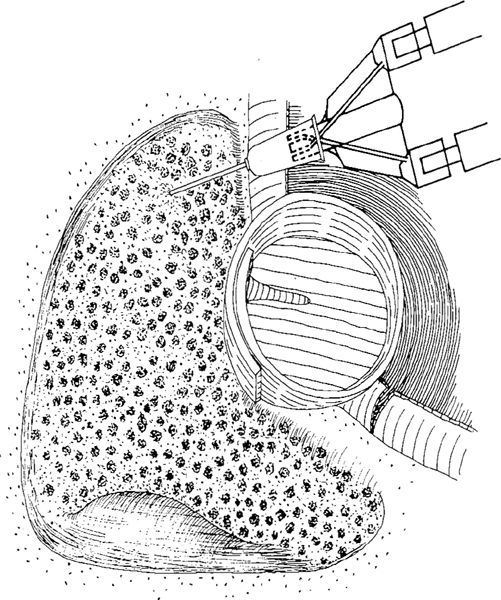
Fig. 998 Obliteration with autogenous cancellous bone chips from the tibial crest (Fillipo and Barbara). The tympanic cavity is separated from the mastoid cavity with a roll of Silastic. The mastoid cavity is filled with cancellous bone chips and fibrin glue
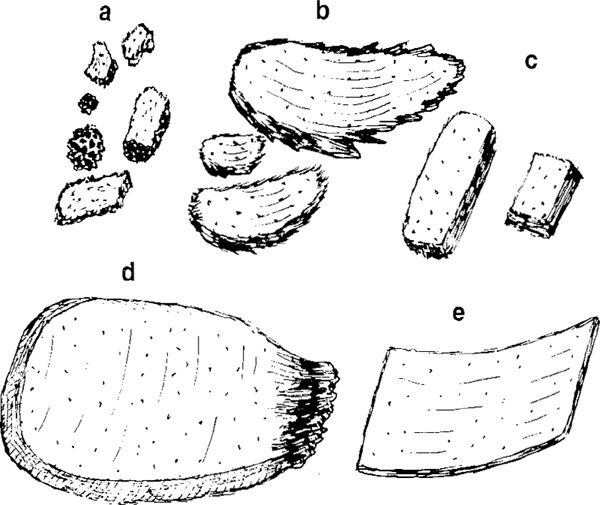
Fig. 999 Various pieces of orthotopic autogenous bone from the mastoid process. a Bone chips of various sizes, of cancellous bone and of cortical bone. b Curled pieces of cortical bone harvested with curved chisels of various sizes. c Bony plates harvested with straight, thin chisels, mainly from the edges of the cavity. d A large piece of cortical bone harvested as the first piece from the cortex of the tip of the mastoid process. e Thin cortical slices harvested with a very thin, straight chisel
Orthotopic Mastoid Bone
Bone from the mastoid process is easily harvested. The present author starts every cortical mastoidectomy by chiseling the mastoid cortex, partly to harvest pieces of bone of various sizes and shape in case they may be needed for ossiculoplasty or obliteration, and partly because using the chisel at this stage is a rapid and efficient way of starting the procedure. If a curved chisel is placed tangentially in relation to the mastoid bone, there is no danger of damaging the sigmoid sinus. Theoretically, the mastoid bone is cancellous and cortical, but practically, very little cancellous bone can be harvested from the mastoid process, especially since bone in contact with cholesteatoma and mucous membrane must not be used. Only cortical bone from the mastoid process is therefore used.
Autogenous cortical bone can be used in various shapes and for various purposes.
1. Bone chips, usually cut with a rongeur from larger bone pieces, are especially suitable for obliteration of deeper parts of the cavity (Fig. 999a). The term “bone chips” is usually used for cancellous bone in orthopedic surgery, but in otologic literature the term “bone chips” is used for any small piece of bone, or even for larger pieces, which are usually cortical.
2. Curled bone pieces are produced at the beginning of the mastoidectomy using a 4-mm curved rhinoplasty chisel (Pou 1977). The graft is cut fairly thin, so that it curls as it is cut and thus has the contour of the ear canal (Fig. 999b). The curled bone pieces can be small or large, depending on the size of the curved chisel used. The chisels are placed more or less tangentially to the cortical bone of the mastoid plane. Because the method results in many fractures of the bone, it can easily be divided into smaller pieces.
3. Bone plates are produced with straight chisels of various size, usually along the edges of the cavity. The chisel is placed more or less perpendicular to the cortical bone. The plates can be cut to various sizes and placed in the cavity. The plates are also used for special purposes, e. g., in the attic, to close the communication with the tympanic cavity, or in scutumplasty, as well as in reconstruction of the bridge, attic, or ear canal wall, and also in ossiculoplasty (Fig. 999c).
4. Large pieces of bone are harvested at the start of the mastoidectomy, usually from the tip of the mastoid process, especially in cases with extensive pneumatization (Fig. 999d). The large pieces can be shaped for use in reconstruction of the ear canal wall (Fig. 837, 838), or placed on the medial wall of the attic as the most meatal part in obliteration.
5. Slices of bone are produced by careful chiseling with an extremely thin chisel (Fig. 999e), for use in Nakano’s reconstruction of the ear canal wall (1993).
6. Bone paté can be harvested by drilling the mastoid process before reaching the mucosa or other pathology within the cells. Bone paté can be collected in many ways using a bone collector, e. g., the Perkins type (Fig. 842), or industrially-made small bone collectors. The paté can also be harvested without collectors, applying slow-speed drilling on the surface of the bone with very little water. In this way, the bone paté is retained around the site of drilling, and it can then be collected with a spoon-like instrument.
Obliteration with Bone Chips
Bone chips, small bony plates, or small curled pieces of bone, are usually used in combined-graft obliteration (Tos 1977), behind cartilage (Figs. 979, 980), and in obliteration of a cavity behind an intact ear canal wall (Figs. 381–383). Palva (1989), however, has used bone chips for reconstruction of the attic wall in obliteration with bone paté (Fig. 1000). After a canal wall–down procedure for attic cholesteatoma, the ear canal skin remains as an intact tube in Palva techniques. At the end of the operation, the ossicular chain is reconstructed, and the defect in the drum and the ear canal skin adjacent to what was Shrapnell’s membrane are covered with an underlay fascial graft extending laterally. The ear canal is then carefully packed with Gelfoam and gauze to maintain its original size. The medial part of the cavity is filled with bone paté. The bone chips and small bony plates mainly obliterate the attic, and are arranged in such a way that they represent the medial wall of the new ear canal. A Palva flap is replaced behind the fascia, and the cavity is filled with bone paté.
Obliteration with Bone Plates
Obliteration with bone plates, curled bone pieces, and bone chips (Shinkawa and Sakai 1990, 1992) involves using large bony plates placed on the medial wall of the attic, posterior to the facial nerve, tightly closing off the connection between the attic and the tympanic cavity (Fig. 1001). Behind the bony plate, the cavity is obliterated with bone chips and small, curled bone pieces of various sizes. The technique exclusively uses autogenous bone, but a musculoperiosteal flap is placed laterally. Comparing the results in 313 cases treated by obliteration of various types, Shinkawa and Sakai (1990) concluded that use of a muscle flap alone leads to postoperative dilation of the auditory canal. Use of bone paté may aggravate postoperative infection, and this material appeared, in their opinion, to be a poor choice for obliteration when compared to bone chips and small bone plates, which were favored as obliteration materials.

Fig. 1000 Obliteration with bone chips, curled bone pieces, bone paté, and a Palva flap (Palva). Bone chips and bone plates are placed medially on the attic wall, forming the medial part of the ear canal wall. The laterai part of the ear canal wall is reconstructed with a large Palva flap and a piece of fascia. Behind the ear canal, bone paté obliterates the cavity. Some Gelfoam covers the bone paté laterally
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


