Fig. 240 Antrotomy with drainage of the antrum as an open procedure: The lateral mastoid cells are removed. The antrum is opened with a curette, and the granulation tissue is removed. Inferiorly in the mastoid process, the air cells are not developed
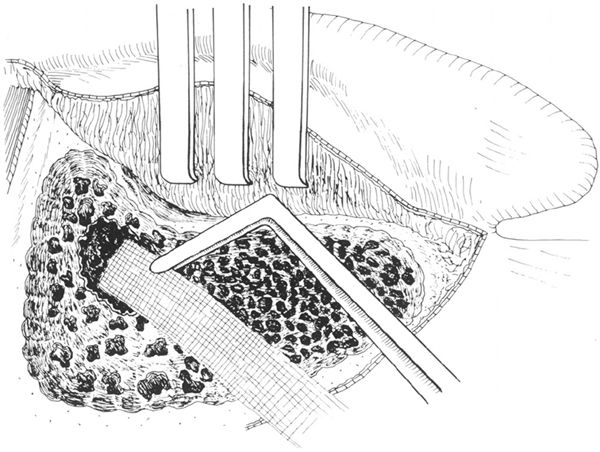
Fig. 241 Iodoform gauze ist placed in the antrum, and covers all the denuded bone. The gauze is changed every three days, and the cavity gradually becomes granulated from inside
Unfortunately, because the indication was wrong and the outcome unfortunate after a mastoidectomy performed on a person close to the Danish royal family, the operation fell out of favor for the following hundred years. The personal physician to the King of Denmark, Baron Bergen, suffering from deafness and tinnitus, asked his friend and colleague Kølping, who was the King’s personal surgeon, to drill out his mastoid process in order to relieve him of tinnitus. The operation was, of course, undertaken without any surgical asepsis, and Bergen died 12 days later. In 1853, Sir William Wilde introduced the famous retroauricular incision for suppuration of the ear with retroauricular abscess, but he advised against opening the bone unless there were life-threatening symptoms, and apparently he never carried out a mastoidectomy. In 1873, Schwartze and Eysell described the indications for, and technique of, the mastoid operation, and by the end of the nineteenth century, the simple mastoidectomy was generally accepted. In 1905, Whiting stated that “as a life-saving measure, few surgical procedures are equal in efficiency to the modern mastoid operation.”
The dread with which a mastoid operation was often accompanied by the laity was not caused by the operation itself, but by the infection often already extending beyond the mastoid process into the petrous apex. The patients died because of the extent of the disease despite the mastoid operation, which was insufficient in petrositis. In the 1930s, several methods were published to deal with petrous apex pathology in connection with simple mastoidectomy (Kopetsky 1929, Eagleton 1931, Kopetsky and Almour 1931, Ramadier 1933, Lempert, 1937). The first use of sulphanilamide in 1935 tremendously reduced the serious complications of acute mastoiditis, especially the potentially fatal meningitis.
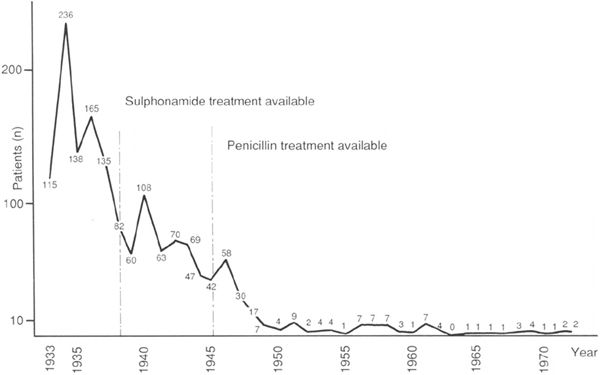
Fig. 242 Annual incidence of simple mastoidectomies for acute mastoiditis from 1933 to 1973 in the ENT department of Sundby Hospital, one of the seven ENT departments in Copenhagen city (courtesy of Dr. C. B. Pedersen, University of Aarhus)
Incidence of Mastoidectomy
The introduction of penicillin after the second world war dramatically reduced the need for surgery, and the incidence of mastoidectomy decreased rapidly during the following years.
In the pre-sulphonamide era, 1–5% of patients suffering from acute suppurative otitis media required a mastoidectomy. The percentage is dependent upon the virulence of the organism, and different figures were seen in different epidemics (Glasscock and Shambaugh 1990). During the period 1947–1981, an annual incidence of 0.004% among cases with acute otitis was found in Finland (Palva et al. 1985). During this period, only 12 mastoidectomies for acute mastoiditis were performed. In one of the seven Copenhagen city Ear, Nose, and Throat departments (the Sundby Hospital), 236 mastoidectomies were performed in 1934, which projected would mean at least 1000 mastoidectomies per year in the Community of Copenhagen City, with 617,000 inhibitants. The decrease in the annual incidence is clearly illustrated in Figure 242, and today in the same area the two Ear, Nose and Throat departments perform about five mastoidectomies per year.
In our department, covering a population of 350,000 inhabitants living in the northern half of Copenhagen County, mastoidectomy for acute mastoiditis is performed three or four times per year, which means that young otologists on duty will have to perform an acute mastoidectomy on children without having seen it before.
Indications for Simple Mastoidectomy in Acute Mastoiditis
Today, there are few absolute indications and several relative indications for simple mastoidectomy. In fact, there is wide disagreement regarding the indications for mastoidectomy in acute mastoiditis. Generally, it can be stated that the simple mastoid operation is indicated for acute suppurative otitis media that fails to respond to antibiotic therapy and proceeds to coalescent mastoiditis. The questions arising from this are: What do we understand by failure of antibiotic treatment, and which clinical signs indicate a coalescent mastoiditis that has to be treated surgically?
Absolute Indications
1. Retroauricular subperiosteal abscess (Fig. 243). Subperiosteal abscess is a result of extension of the coalescent mastoiditis onto the surface of the mastoid process. This extension usually occurs through the cribriform area behind the suprameatal spine. The tissues over the mastoid process are thick and red, due to the thickness of the periosteum and the subcutaneous tissue. Fluctuation is the best sign of an abscess, and although it may or may not be easy to detect initially, fluctuation can be demonstrated as the subperiosteal abscess matures.
2. Zygomatic subperiosteal abscess. Extension can occur, although less often, over the posterior root of the zygoma, producing a zygomatic abscess (Fig. 244), elevating the periosteum under the lower edge of the temporalis muscle. The upper half of the auricle is displaced away from the skull and downward.
A very rare type of extension is from the cells of the root of the zygoma downward and forward into the mandibular fossa (Shambaugh 1941). The abscess appears just in front of the tragus, with displacement of the mandible to the opposite side, creating a malocclusion.
3. Bezold abscess. Extension through the medial aspect of the mastoid tip into the digastric grove produces the Bezold’s abscess, situated deep in the neck, deep to the sternocleidomastoid muscle and the digastric muscle (Bezold 1908). The abscess does not reach the surface, and no fluctuation can be felt. There is moderate swelling around the lower end of the mastoid process. The suppuration can spread in all directions below the fascia of the neck, and may descend down into the superior medi astinum.
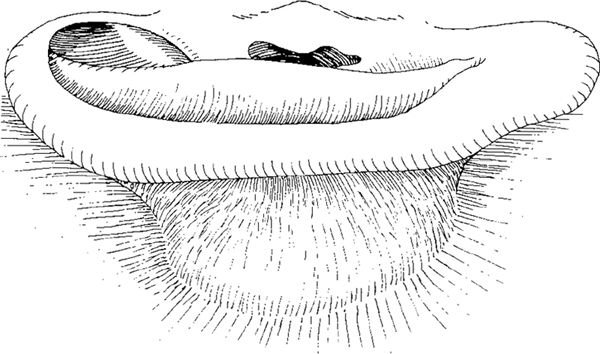
Fig. 243 A retroauricular subperiosteal abscess in acute mastoiditis developed behind the auricle. The abscess has displaced the auricle anteriorly
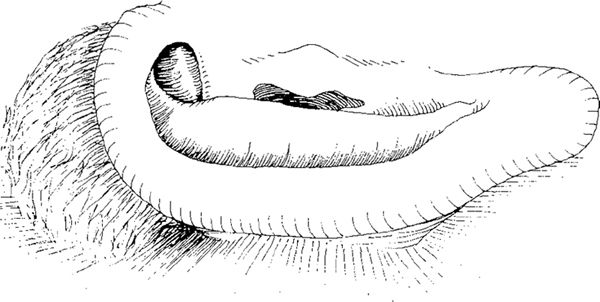
Fig. 244 A zygomatic subperiosteal abscess in acute mastoiditis, arising from the zygomatic cells. The auricle is displaced inferiorly
These various abscesses, even though they are rare, represent absolute indications for simple mastoidectomy.
Relative Indications
1. Persistent pain located behind the ear is a common symptom of coalescent mastoiditis due to the pressure of the inflamed tissue and restricted drainage. The pain increases when the patient is in the horizontal position. Severe pain suggests an extradural abscess, and a location deep behind the eye suggests a coalescent abscess of the petrous apex. Persistence of pain for longer than two weeks after the onset of acute otitis media is a relative indication for surgery, as is recurrent pain occurring several weeks after painless discharge in acute otitis.
2. Persistent tenderness over the mastoid process is the most consistent physical sign of coalescent mastoiditis. Even though tenderness may be considerable in the first few days of acute otitis, it is not an indication for surgery, but if it persists after several weeks, it points toward a coalescing process.
3. Sagging of the posterosuperior meatal wall due to thickening of the periosteum near the antrum. Sagging can occlude the external meatus.
4. Periosteal thickening over the lateral surface of the mastoid process is caused by edema in a mastoid abscess approaching the lateral surface of the mastoid process.
5. Persistence of a profuse, creamy aural discharge for more than four weeks in acute suppurative otitis media is a symptom of a coalescent process in the mastoid, but the author prefers to continue with antibiotics and local treatment in the form of daily cleansing of the ear with saline and instillation of ear drops for some few weeks more before surgery.
Recent studies on acute mastoiditis in children have concluded that, in the absence of subperiosteal abscess or central nervous system involvement, a 48-hour trial of intravenous antibiotic therapy directed against staphylococci is justified before mastoidectomy is considered (Nadal et al. 1990, Prescut and Mallan 1991).
Simple Mastoidectomy Technique in Infants
In infants, the mastoid process is not yet developed, the cortical lamina is thin, and infantile mastoiditis with subperiosteal abscess appears relatively early after the onset of acute otitis. The spread of pus onto the surface of the mastoid process passes along the vessels through the relatively patent cribriform area.
Before the incision, a myringotomy and grommet insertion is performed in the anterosuperior quadrant of the drum. These procedures are carried out through an ear speculum.
The retroauricular incision runs 0.5–1.0 cm behind the retroauricular fold. The incision ends somewhat higher than the usual retroauricular incision, to avoid trauma to the facial nerve and the parotid gland (Fig. 245). Usually, the incision passes through the subperiosteal abscess on the way down to the cortical bone. Passing through the subperiosteal abscess onto the surface, small holes within the cribriform area of the cortical bone are sometimes recognizable, with pus coming out from the depths (Fig. 246). By following these holes, the antrum is found after removal of the soft cortical bone with a sharp curette or a cutting burr.
Before drilling, the granulation tissue and the periosteum surrounding the abscess is removed, and the surface of the mastoid process is cleaned (Fig. 246). The pus is sent for bacterial culture, using either a swab or aspiration. The fibers of the sternocleidomastoid muscle attached to the surface of the mastoid process are cut with a knife, and elevated together with the granulation tissue from the subperiosteal abscess. All the granulation tissue around the abscess is cleared, and the cortical bone is widely exposed (Fig. 247). The ear canal skin is not detached from the bone; only the suprameatal spine and the most lateral border of the ear canal are located.
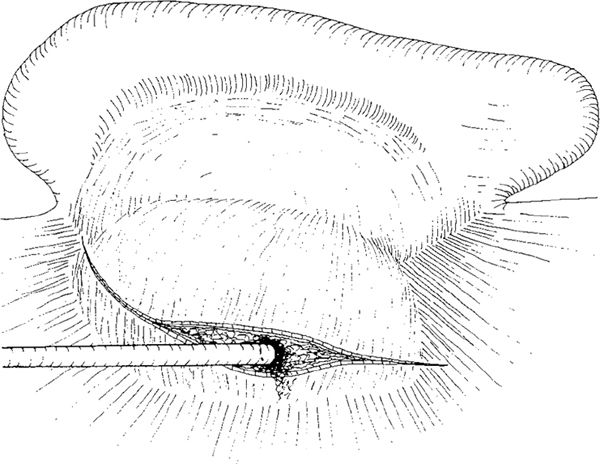
Fig. 245 Simple mastoidectomy in infants. The incision is placed over the top of the subperiosteal abscess, 0.5–1.0 cm behind the postauricular fold. It is directed more posteriorly, avoiding the stylomastoid region, the parotid gland, and the facial nerve. The incision ends at the tip of the mastoid process, which in infants is considerably shorter than in older children. Pus is taken for bacteriological culture and then suctioned away
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


