aIncludes mucoepidermoid carcinoma, mesenchymal chondrosarcoma, teratocarcinosarcoma, angiosarcoma, osteoma, leiomyosarcoma, fibrovascular polyp, ameloblastic carcinoma, PNET/Ewing sarcoma, high-grade unclassified sarcoma, malignant solitary fibrous tumor, germ cell tumor, myoepithelial carcinoma, liposarcoma, hemangioma.
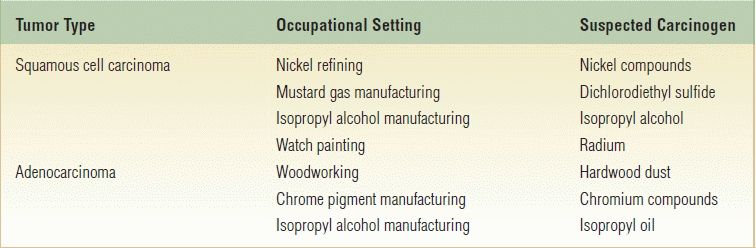
Table 18.2 Occupational Hazards Associated with Paranasal Sinus Tumors
The transcranial approach for anterior craniofacial resection is a technique used to manage these sinonasal malignancies when the neoplasm extends to or through the base of the skull to involve the parameningeal space, the meninges themselves, or the intradural and intracerebral structures. The technique provides excellent visualization, the ability to manage the orbits safely and completely, and the opportunity for robust dural and cranial base repair.
HISTORY
The most common initial symptoms of malignant sinonasal disease are nasal airway obstruction that is frequently unilateral, chronic nasal discharge, and epistaxis. Unfortunately, these early symptoms of malignant disease are identical to those of benign nasal and paranasal sinus disease. Studies have shown a combined physician and patient delay ranging from 3 to 14 months due to this nonspecific symptom complex. The liberal use of imaging studies and early biopsy has lessened the diagnostic delay and increased the percentage of tumors being diagnosed at an earlier stage.
Tumors of the superior aspect of the nasal cavity and ethmoid sinus may be associated with anosmia and headache. Carcinoma of the frontal sinus may present as an acute frontal sinusitis with pain, swelling, and evidence of bone erosion. Nasal obstruction, epistaxis, and nasal discharge may be absent when the tumor is located in the sphenoid sinus, and patients typically suffer from headache, diplopia, and cranial neuropathy.
PHYSICAL EXAMINATION
A thorough examination of the head and neck, including endoscopic evaluation of the sinonasal and nasopharyngeal regions, is an important part of the evaluation of patients suspected of having a malignancy of the sinonasal tract. Middle ear effusion may indicate tumor involvement of the nasopharynx, eustachian tube, pterygoid plates, or tensor veli palatini muscle. The cranial nerves must be evaluated. A full ophthalmologic examination should be completed. Eye movements should be carefully assessed to identify any restriction of movement consistent with involvement of the orbital tissues or ocular motor nerves. Specific attention should be paid to examination of the trigeminal nerve. The not infrequent occurrence of perineural extension of malignancy to the branches of the trigeminal nerve may be identified by areas of hypesthesia associated at times with paresthesia. Biopsy of any suspicious lesions should be performed.
INDICATIONS
Parameters to consider when planning management for a patient with a malignancy of the paranasal sinuses include tumor pathology and biologic aggressiveness, extent of disease, the availability and potential success rates of adjuvant therapies, and the potential for functional impairment and esthetic deformity with extirpative surgery. Currently, most patients are treated with surgery and radiation therapy as a combined treatment modality, but other adjuvant therapies such as chemotherapy and radiosurgery may be indicated (Table 18.3). Optimal patient outcome is only achieved through multidisciplinary assessment and management.
Table 18.3 Management Paradigms and Applicable Malignancies
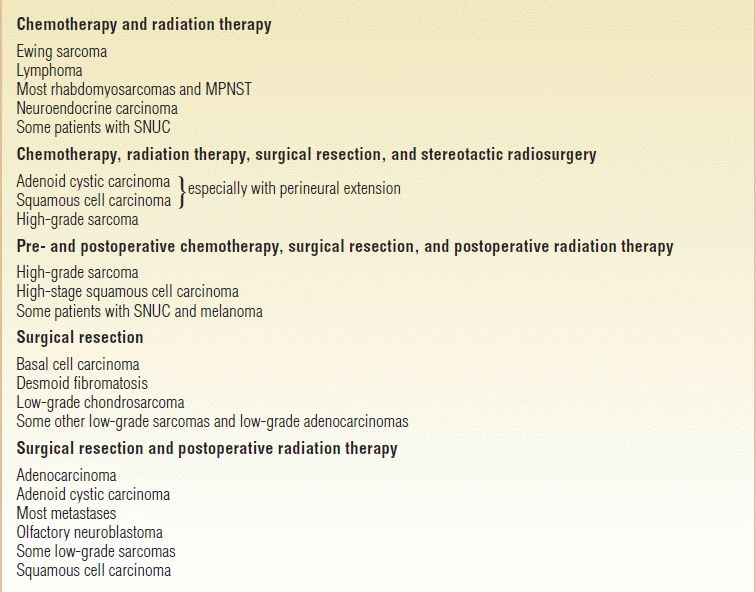
MPNST, malignant peripheral nerve sheath tumor; SNUC, sinonasal undifferentiated carcinoma.
CONTRAINDICATIONS
Patients with comorbidities, such as severe cardiovascular disease; markedly debilitated or demented patients; patients with coagulopathy; or those with end-stage renal or pulmonary disease will probably not benefit by excision of these tumors. Although patients with metastatic disease are usually not candidates for craniofacial resection, those with oligometastatic disease of low- to intermediate-grade tumors are occasionally selected for craniofacial resection for palliation of specific symptoms such as optic neuropathy and pain. I do not recommend craniofacial resection for patients with involvement of the intracranial internal carotid artery by high-grade malignancy.
PREOPERATIVE PLANNING
Computed tomography (CT) and magnetic resonance imaging (MRI) are complementary studies and the imaging methods of choice for assessing sinonasal malignancies. CT imaging is particularly useful for assessing bone changes, especially erosion. Direct coronal CT is best for evaluating the integrity of the anterior skull base including the roof of the orbit, cribriform plate, and planum sphenoidale (Fig. 18.1). The extent of tumor is best assessed with MRI, which can differentiate tumor from inflamed mucosa, blood, or inspissated mucus in most cases (Fig. 18.2). Obliteration of adipose tissue planes in the pterygopalatine fossa, infratemporal fossa, and nasopharynx usually indicates tumor involvement of these regions (Fig. 18.3). Dural thickening and enhancement are usually an indication of tumor invasion (Fig. 18.4). Similarly, thickening and enhancement of cranial nerves indicate perineural spread of the malignancy (Fig. 18.5). The identification by MRI of signal voids within the tumor or proximity of the neoplasm to the internal carotid artery may be an indication for preoperative angiography to assess tumor vascularity and plan surgical treatment. PET–CT along with MRI may help to identify lymph node involvement or distant metastasis. This, however, occurs in less than 10% of patients at initial evaluation.
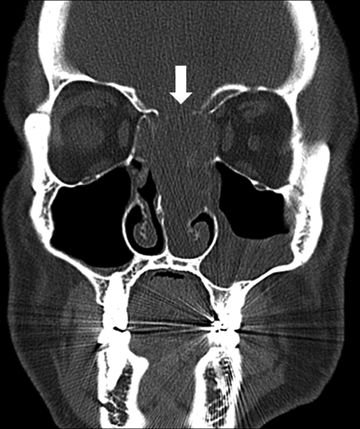
FIGURE 18.1 Coronal CT with bone window algorithm. The arrow identifies erosion of the cribriform plate in this patient with sinonasal neuroendocrine carcinoma. (All figures are property of the Department of Neurosurgery, The University of Texas M.D. Anderson and are used with permission.)
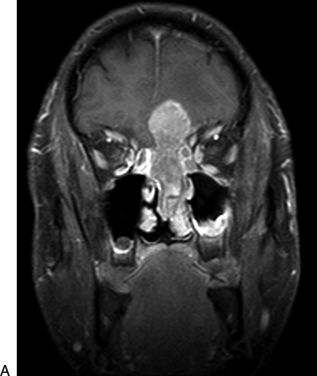
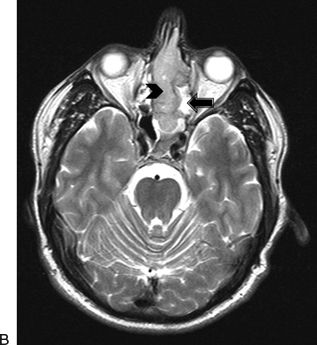
FIGURE 18.2 A. Coronal postcontrast T1-weighted MRI reveals an enhancing tumor of the sinonasal cavity with transcranial extension into the left subfrontal region. (Same patient as in Fig. 18.1) (All figures are property of the Department of Neurosurgery, The University of Texas M.D. Anderson and are used with permission.) B. Axial T2-weighted MRI reveals a tumor of the sinonasal cavity of intermediate signal intensity (arrowhead) and adjacent high T2 signal intensity sinus secretions (arrow) (Same patient as in Fig. 18.1) (All figures are property of the Department of Neurosurgery, The University of Texas M.D. Anderson and are used with permission.)
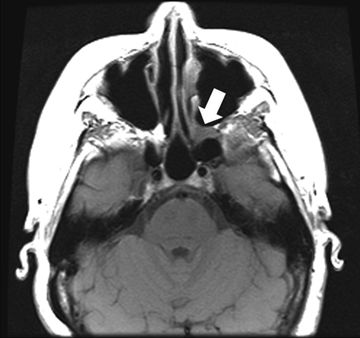
FIGURE 18.3 Axial noncontrast T1-weighted MRI of patient with sinonasal adenoid cystic carcinoma. Note the expansion of the left pterygomaxillary fossa (arrow) with loss of fat hyperintensity. (All figures are property of the Department of Neurosurgery, The University of Texas M.D. Anderson and are used with permission.)

FIGURE 18.4 Sagittal postcontrast T1-weighted MRI identifies dural thickening and nodular enhancement consistent with recurrent sinonasal adenocarcinoma (arrow). (All figures are property of the Department of Neurosurgery, The University of Texas M.D. Anderson and are used with permission.)
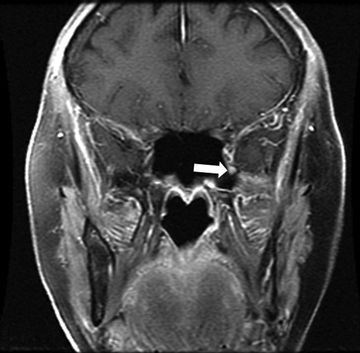
FIGURE 18.5 Coronal postcontrast T1-weighted MRI. The arrow highlights the enlarged and contrast-enhancing left maxillary nerve in this patient with adenoid cystic carcinoma of the maxillary sinus. Pathologic confirmation of perineural extension of malignancy was made at the time of surgery. (All figures are property of the Department of Neurosurgery, The University of Texas M.D. Anderson and are used with permission.)
Optimal management plans can only be constructed with accurate pathologic diagnosis of the neoplasm. Endoscopy permits access to most tumors of the sinonasal cavities. Occasionally, deep-seated lesions can be sampled by CT-guided needle biopsy. The importance of evaluation of the biopsy specimen by an experienced pathologist cannot be overemphasized.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


