
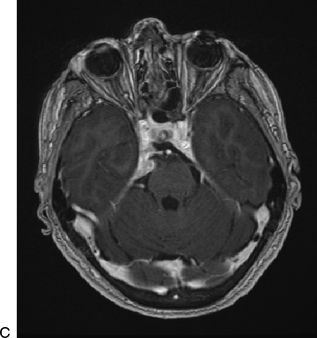
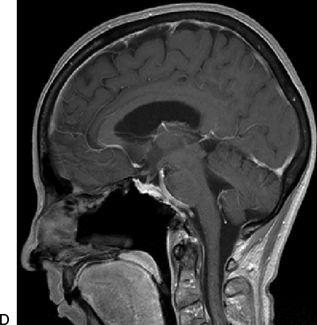
FIGURE 36.1 A. T1-weighted postcontrast axial MRI. B. CT angiogram sagittal reconstruction demonstrating a primarily clival meningioma with midline origin and dural base. Following endoscopic endonasal resection, only a small, paramedian residual is left. C. Postcontrast axial. D. Sagittal T1-weighted MRI.
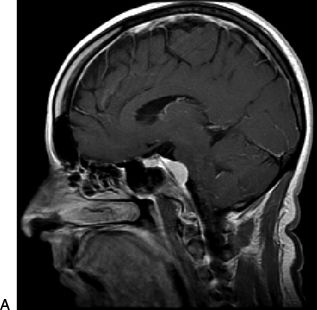
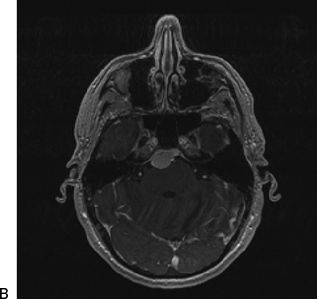
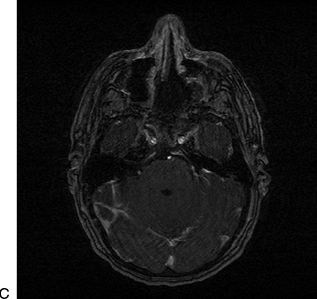
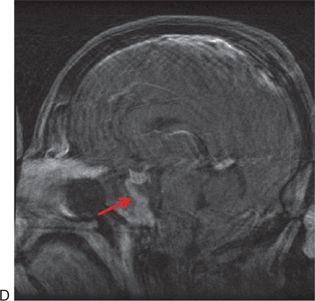
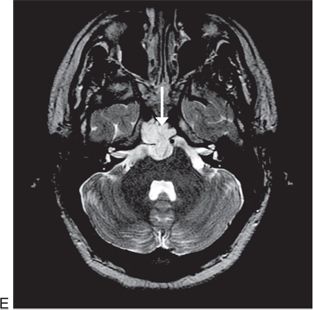
FIGURE 36.2 A. T1-weighted postcontrast sagittal. B. axial MRI demonstrating a primarily clival meningioma with midline origin and dural base. Following endoscopic endonasal resection, the clival location allows for complete resection demonstrated on (C) immediate postoperative postcontrast axial and (D) sagittal T1-weighted MRI. Note enhancing nasoseptal flap used for reconstruction (dashed arrow). E. T2-weighted, axial MRI showing the typical, hyperintense “bubbly” appearance of a clival chordoma (arrow).
Care should be taken to properly define the differential diagnosis of clival lesions. The diagnosis of benign fibro-osseous lesions such as fibrous dysplasia can usually be made radiographically, with their classic “ground glass” appearance, so that intervention can be avoided. Rare exceptions include progression with optic or cranial neuropathy, usually in children or adolescents and associated with cyst formation. Rarely, pituitary adenomas erode into and invade the clivus primarily, rather than extending into the suprasellar space. Extending a sellar exposure into the mid and even inferior clivus is required for complete removal of such tumors.
Nasopharyngeal cancers are usually advanced at the time of presentation and are treated primarily with radiation therapy. The primary role of surgery is biopsy for diagnosis and debulking of tumor to relieve symptoms prior to radiation therapy. Exceptions include small tumors that can be completely resected with adequate margins. For adenoid cystic carcinoma, the goal of surgery is maximal removal with minimal morbidity, followed by radiation therapy. It is not possible to achieve clear resection margins with adenoid cystic carcinoma of the skull base due to perineural spread, and the extent of surgery is limited by the surrounding neural and vascular structures. Surgical salvage of residual tumor following radiation therapy is of potential value for local control and should be considered based on posttreatment functional imaging with PET–CT or the results of biopsies.
CONTRAINDICATIONS
Tumors originating in the lateral skull base but extending medially will displace critical neurovascular structures medially, into the path of a midline approach such as an EEA. This remains the major contraindication to EES. Sinus infection is a transient contraindication to intradural (or potentially intradural) surgery that should be treated with antibiotics with or without surgical drainage as indicated before proceeding.
PREOPERATIVE PLANNING
Magnetic resonance imaging (MRI) and computed tomographic angiography (CTA) are complementary, and it is important to obtain both to help determine preoperative differential diagnosis. For example, MRI illustrates the typical heterogeneously hyperintense T2 “bubbles” of a chordoma or chondrosarcoma (Fig. 36.2), while CTA illustrates bony erosion, ICA stenosis, or occlusion and identifies benign fibro-osseous lesions such as fibrous dysplasia (that can appear very ominous on MRI). With meningiomas, MRI will show the dural tail while CTA illustrates the vascular relationships and degree of bony involvement or hyperostosis (Figs. 36.1 and 36.2).
SURGICAL TECHNIQUE (VIDEO 36.1)
All surgeries are performed by a team consisting of an otolaryngologist and a neurosurgeon performing a two-surgeon, three- or four-hand technique. This allows for appropriate care of both sinonasal and neural structures as well as critical dynamic endoscopy and bimanual microsurgical techniques. Additional benefits include improved problem solving (“copilot”) and efficiency.
Most patients are placed in three-pin head fixation with the head in a neutral or slightly extended position and rotated toward the side where the surgeons stand. This allows for precise positioning to optimize surgical ergonomics as well as prevent movement during critical portions of the operation. Registration of the navigation system is performed, and nasal decongestion with topical oxymetazoline (0.05%) is achieved. The external nose and nasal vestibule are prepped with an iodine solution, and perioperative antibiotic prophylaxis is provided with a third-generation cephalosporin.
Nasal endoscopy is performed with a 0-degree endoscope, and the turbinates are lateralized to provide greater access to the nasopharynx. The inferior portion of the middle turbinate is typically resected to provide room for endoscopy. If a dural defect is anticipated, a septal mucosal flap is elevated on the side contralateral to the bulk of the tumor and is placed into the maxillary sinus through a middle meatal antrostomy for storage during the surgery. The posterior septum is detached from the sphenoid rostrum, and the rostrum is resected to provide binarial access to the sphenoid sinus. The sphenoidotomy is maximized to provide full access from the sella to the floor of the sinus and lateral to both internal carotid arteries. Sphenoid septations are removed with bone rongeurs and drilling, and landmarks are identified with special attention to the course of the paraclival carotid arteries.
Fascia is elevated from the inferior margin of the sphenoidotomy, and the medial pterygoid plates are exposed bilaterally. The inferior portion of the clivus is exposed by resecting the nasopharyngeal mucosa and basopharyngeal fascia. This can be done either with a microdebrider or with monopolar electrocautery (needle tip or suction). Care should be taken to evaluate the course of the parapharyngeal ICA as it can become ectatic and loop medially at its most inferior (proximal) aspect. This is rarely an issue, but when it is, dissection of the fascia from the bone should occur in the subperiosteal plane, deep to the artery. Laterally, the supracondylar groove should be identified. This is a ridge of bone to which the fascia of the rectus capitis anterior muscle attaches; it reliably predicts the location of the hypoglossal canal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


