 urgical management of thick iridocapsular membranes is difficult. At times, these membranes may be so tough that it becomes difficult if not impossible to cut them with a capsulotomy needle, a small scissors, or a vitrectomy cutter. Although originally designed as a capsulotomy device, the Fugo blade is an invaluable cutting device for the management of thick iridocapsular membranes. In cases of ocular trauma, persistent hyaloid vasculature, or membranes thickened as a result of postoperative complications, the use of the Fugo blade is amply justified.
urgical management of thick iridocapsular membranes is difficult. At times, these membranes may be so tough that it becomes difficult if not impossible to cut them with a capsulotomy needle, a small scissors, or a vitrectomy cutter. Although originally designed as a capsulotomy device, the Fugo blade is an invaluable cutting device for the management of thick iridocapsular membranes. In cases of ocular trauma, persistent hyaloid vasculature, or membranes thickened as a result of postoperative complications, the use of the Fugo blade is amply justified.
We have successfully used the Fugo blade to perform membranectomy inside the anterior chamber.
TECHNIQUE
Anesthesia
Inject topical drops or lidocaine under the conjunctiva.
Surgical Technique
- Make a 2.8-mm keratome incision at the limbus and a paracentesis incision at 90 degrees from this incision.
- Deepen the anterior chamber with hydroxypropy-lmethylcellulose (HPMC). Introduced the plasma knife tip at the 2.8-mm incision.
- Use the paracentesis incision to continuously inject methyl cellulose into the anterior chamber while the knife is cutting. This helps keep the anterior chamber deep and aids in pushing the cavitation bubbles away from the working field. To this end, a 26-gauge cannula connected via a silicone tube to an HPMC syringe is used, operated by an assistant on instruction from the surgeon. This method offers more control than having the surgeon alone trying to inject the HPMC. In addition, the HPMC cannula helps to stabilize the globe while the Fugo blade is in action.
- Once the HPMC irrigating cannula is in place and the tip of the plasma knife is positioned inside the anterior chamber, calculate the size of the opening. Usually one pass is enough to cut the membrane through its entire thickness. Cut any bridges of uncut tissue with a second pass.
- Stain the anterior capsule or the membrane with trypan blue to provide extra visibility. Pupil-dilating hooks may be needed in certain cases to achieve suitable exposure of the surgical field.
Case 1: Posttraumatic Thick Pupillary Membrane
A 22-year-old man suffered an injury in a road accident 6 months prior. The left eye was lost and the right eye suffered severe injuries. The cornea had been repaired. The ruptured cataract had absorbed, leaving behind a thick membrane in the pupil formed by the fusion of the anterior and posterior capsules and imprisoned lens material. We planned to clear the visual axis with the plasma knife and implant an iris claw lens, if possible.
After making the usual entry points the plasma knife tip was introduced into the anterior chamber through a 2.8-mm keratome incision while the HPMC cannula was introduced from the left paracentesis to deliver continuous methylcellulose irrigation (Fig. 17.1).
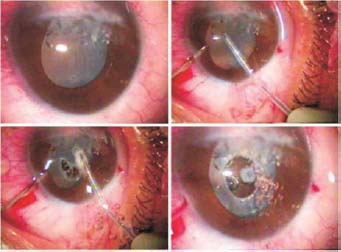
Figure 17.1. Thick posttraumatic pupillary membrane (Case 1) is cut with the Fugo blade.
The Fugo blade was activated and a round circle was traced and cut in the optical axis of the dense membrane, followed by a small anterior vitrectomy.

Figure 17.2. The same patient as in Figure 17.1 at the end of surgery (left) and 10 months later (right).
An iris claw lens was implanted (Fig. 17.2) and fixed to the anterior surface of the iris.
Case 2: Capsulotomy for Congenital Cataract
A 9-year-old patient had had surgery for congenital cataract and posterior chamber lens 4 years before. We used the Fugo blade to perform capsulotomy.
The pupil was pulled in one direction and then dilated with iris hooks. The intra-ocular lens was found to be encapsulated with thick membrane on both sides. Membranectomy of the dense membranes on both sides was performed with great ease, using the Fugo blade at medium settings (Figs. 17.3 and 17.4).
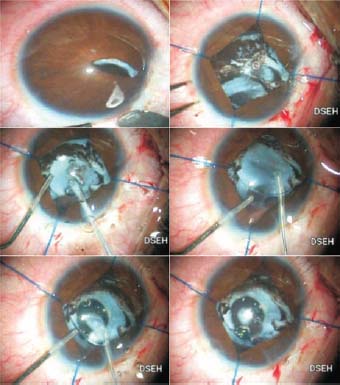
Figure 17.3. Postcataract surgery as a complicated case (Case 2). The iris is retracted and the Fugo blade is taken under the optic of the posterior chamber lens and a round membranectomy is done.

Figure 17.4. The same patient as in Figure 17.3, showing the appearance at the end of surgery (left) and 4 months later (right).
Case 3: Pupilloplasty
We performed a pupilloplasty on a 12-year-old patient who had a traumatic cataract with a posterior chamber lens.
As a result of surgery to correct a congenital cataract 4 years earlier, the patient showed pupil capture, a dense membrane, and pupil shrinkage and deformation. There was only one loop of the lens; the other was missing. We first attempted to remove the membrane using a vitrector, but were not successful. We also tried using a capsulotomy needle, but this too failed, and the tissue began to bleed. Finally, the intimidating vascularized iridocapsular membrane in the pupillary area was managed with the Fugo blade. A perfect pupilloplasty was performed, followed by a small anterior vitrectomy. The appearance and recovery were good (Fig. 17.5).
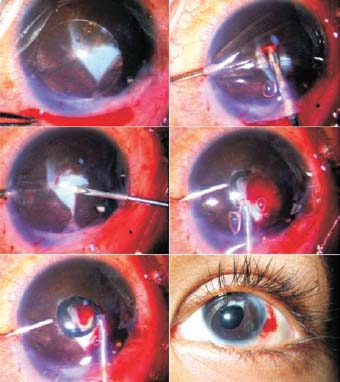
Figure 17.5. Pupil capture and dense membrane formation. First a vitrector was tried and then capsulotomy was attempted with a needle, but both failed. Finally, the Fugo blade was used to do a clean membranectomy and pupilloplasty. The final photo was taken 20 days after surgery.
Case 4: Thick Congenital Vascularized Membrane
One of the toughest challenges in cataract surgery is the management of vascular membranes. These vascular membranes are not only tough to cut but also notorious for bleeding.
Figure 17.6 is the B-scan ultrasound of a 7-monthold patient with a unilateral cataract. The child did not allow detailed examination in the outpatient department but the B-scan revealed the presence of a thick oblique band extending from the back of the lens to the area of the disc. Undoubtedly this was a case of persistent hyaloid vasculature leading to opacification of the lenticular tissue. Based on our previous experience, we expected to encounter some vascularization.
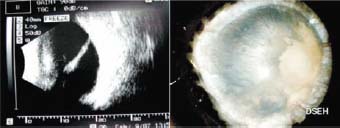
Figure 17.6. A profusely vascularized congenital cataract B-scan showed a thick oblique band from the lens to the retina.
In surgery, we encountered a dense white cataract that was heavily vascularized (Fig. 17.7). The anterior capsule of the cataract was stained with trypan blue and a combination of a capsulotome and a capsularexsis (Utrata) forceps was used to do an irregular capsulotomy. Part fluffy and part stony-type cortex was removed with an irrigation/aspiration (I/A) cannula and a forceps.
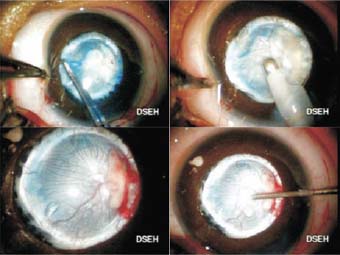
Figure 17.7. Anterior capsulotomy is done, followed by irrigation with aspiration. The thick vascularized posterior capsule is exposed.
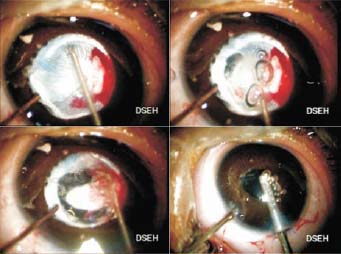
Figure 17.8. The capsulotomy of the vascularized membrane was done with the Fugo blade, followed by clearance with a vitrector.
Once the cortex was removed, the real picture emerged. The posterior capsule was very thick and profusely vascularized, and all the blood vessels appeared to emerge from a single point, presumably at the point of attachment of the persistent hyaloid vessels (Fig. 17.8).
When the Fugo blade was activated, the cutting was instantaneous; however, at places the membrane was so thick than the full length of the cutting tip was unable to penetrate it, so a second pass was needed to incise it all the way. We were surprised to note that despite the number of blood vessels cut, there was minimal bleeding from the tissues. The portion of the membrane that was the node of all the blood vessels bled a bit more than the rest. The cord of persistent hyaloid vasculature could be clearly visualized attached to the back of the posterior capsule.
Finally, the last part of the membrane was cleared away with a vitreous cutter.
Summary
The Fugo blade has proven to be a capable cutting instrument. Its impeccable cutting ability along with its hemostatic properties makes it an excellent choice for the treatment of thick pupillary membranes.
Suggested Reading
Fugo RJ. Fugo blade to enlarge phimotic capsulorrhexis. J Cataract Refract Surg. 2006;32:1900.
Samalonis LB. Improving capsulotomies. Eyeworld. 2001; 6:42–44.
Singh SK. Fugo blade capsulotomy: a new tech cutting technology. Trop Ophthalmol. 2001;1:14–16.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


