 he Fugo blade is a novel electrosurgical device that was designed for ophthalmologic use. Its principles of operation are based on the applied photon bath theory of plasma ablation. Using carbon-based tissue in its path as a fuel source to generate a “cool” cloud of high-intensity plasma energy, the Fugo blade can create a pristine incision in the various tissues of the eye while simultaneously achieving hemostasis in highly vascular fields. At this time, a commercial plasma-based cutting device such as the Fugo blade does not exist for extra-ocular use. The current state of the art in general surgery is the handheld electrocautery, otherwise known as the Bovie. Unfortunately, the Bovie lacks thermal efficiency, often rendering tissues charred and burned as the surrounding tissues at the point of contact act as a heat sink for its extreme high-temperature cutting and coagulation. Although several attempts have been made to harness the laserlike energy deployed by the Fugo blade and apply it for wide application in general surgical procedures, these devices suffer from many limitations and risks. Most notably, surgical lasers based on energy similar to plasma are expensive, bulky, and fraught with dangerous complications such as past pointing and the potential to blind operative staff inadvertently.
he Fugo blade is a novel electrosurgical device that was designed for ophthalmologic use. Its principles of operation are based on the applied photon bath theory of plasma ablation. Using carbon-based tissue in its path as a fuel source to generate a “cool” cloud of high-intensity plasma energy, the Fugo blade can create a pristine incision in the various tissues of the eye while simultaneously achieving hemostasis in highly vascular fields. At this time, a commercial plasma-based cutting device such as the Fugo blade does not exist for extra-ocular use. The current state of the art in general surgery is the handheld electrocautery, otherwise known as the Bovie. Unfortunately, the Bovie lacks thermal efficiency, often rendering tissues charred and burned as the surrounding tissues at the point of contact act as a heat sink for its extreme high-temperature cutting and coagulation. Although several attempts have been made to harness the laserlike energy deployed by the Fugo blade and apply it for wide application in general surgical procedures, these devices suffer from many limitations and risks. Most notably, surgical lasers based on energy similar to plasma are expensive, bulky, and fraught with dangerous complications such as past pointing and the potential to blind operative staff inadvertently.
Based on the Fugo blade’s reported mechanism of operation we hypothesized that the Fugo blade M100 unit could be used for surgical incision of nonocular tissues. To test this hypothesis, we performed several nonocular operations on both rodent and nonrodent species.
Equipment
Workstation
Our standard surgical workstation for small animals consists of a stainless steel surgical cart specially designed for small animal surgery. On this cart, we have an anesthesia machine and heated induction chamber, which can deliver oxygen, isoflurane volatile anesthetic, or a mixture of the two. Other components of the operative theater include a small animal respirator for experiments requiring mechanical ventilation, a warming unit for the operating stage, a high-intensity fiber-optic light source, an operating microscope and various microsurgical instruments. The M100 unit fits nicely on the workstation, with the foot pedal easily positioned under the surgical stool and the handpiece placed on the operative field, making it accessible for use throughout the entire procedure (Fig. 49.1).
__________
*This manuscript is the result of work supported with resources from and the use of facilities at the George E. Wahlen VA Medical Center and by a grant from the Western Institute for Biomedical Research.

Figure 49.1. Experimental workstation featuring the Fugo blade M100 unit.
Fugo Blade M100 Unit
Because the surgical fields in operations pertaining to the eye are quite small and confined, the original Fugo blade M100 unit developed for ophthalmology uses very low power (3 W). Our initial benchtop experiments indicated that this standard M100 unit was underpowered for small animal surgery in nonocular tissues. We therefore had MediSurg, Ltd. modify the Fugo blade circuitry to allow a modest increase in power output without changing the characteristics of the plasma profile generated from the device. This minor modification proved to be sufficient for initial proof-of-concept studies.
Tips
The Fugo blade’s traditional cutting tips are quite fine and are available in right-angled 100-µm and straight 400-µm filaments. We found that these standard tips were quite delicate even for small animal surgery, especially the 100-µm version. We therefore elected not to use the 100-µm filament for macro tissue cutting, such as skin incisions, and evaluated its use for only the most delicate of procedures. We modified the straight 400-µm tip by excising a small portion of the insulating sheath approximately 4 mm back from the terminal end (Fig. 49.2). In addition, we also had MediSurg, Ltd. design a specialized, more durable tip for cutting thicker tissues, such as skin and muscle (Fig. 49.3). The result of these modifications allowed the surgeon to quickly move about the surgical field, which was not afforded with the standard tips.
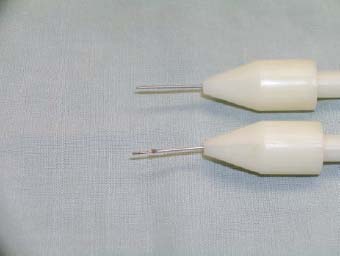
Figure 49.2. Modified 400-µm Fugo blade tip.

Figure 49.3. Custom Fugo blade tip for nonophthalmic surgery.
Materials and Methods
Animals
Prior to investigation we obtained approval from the George E. Wahlen VA Institutional Animal Care and Use Committee for all procedures. We purchased specific pathogen-free animals from established vendors known to the VA.
Initial Benchtop Testing
Before embarking on survival surgeries, benchtop cutting was performed and evaluated on euthanized animals to calibrate the level of power needed for various tissues in rats and rabbits. In these nonsurvival surgeries, complete autopsy and vivisection was performed using various levels of cut power and cut intensity. These power and intensity adjustments were easily performed by manipulating the two large dials on the front of the M100 unit.
Rodent Studies
After completing a series of benchtop evaluations, we performed multiple survival procedures on animals that would otherwise have undergone surgery using scalpels, scissors, and standard monopolar electrocautery. These procedures included both laparotomies with abdominal exploration and thoracotomies, including mediastinal procedures on the heart. In two separate experimental groups, six 250-g, female, Sprague Dawley rats were operated on. In the first set of animals, we performed survival abdominal surgery by performing a paramedian laparotomy. Skin incision was performed using the Fugo blade tip made specifically for our lab (Fig. 49.4). Once through the skin, this tip was exchanged for the modified 400-µm tip to continue further dissection (Fig. 49.5). Although a full-thickness incision could have been performed in one fell swoop, we elected to carefully dissect and divide the abdominal wall in layers following the natural planes of dissection.
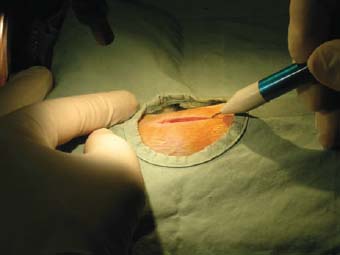
Figure 49.4. Skin incision using a custom Fugo blade tip.
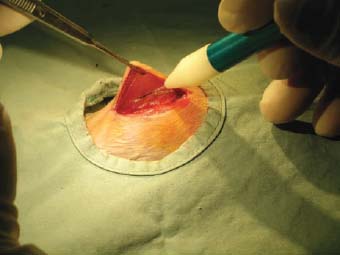
Figure 49.5. Tissue dissection using a modified 400-µm Fugo blade tip.
In the second group of rodents, a left anterolateral thoracotomy was performed using a midline, chest skin incision. Again, after using the customized tip for the skin, the rest of the operation was performed with the modified straight 400-µm tip. With this operation, it is imperative to have complete control over the depth and intensity of the energy produced at the cutting interface, as the small rodent lungs and pleura are extremely delicate and highly susceptible to injury as one enters the left chest. Normally, the left chest would be entered only with cold-instrument, blunt dissection, as the risk of puncturing the visceral pleura on the lung surface is too great. However, the 400-µm tip set on high cut power with a low-to-moderate cut intensity setting was used to enter the thoracic cage for all procedures. In both groups of animals, incisions were closed in layers using running absorbable suture. Animals were allowed to recover in a dedicated, warm postoperative cage and then returned to the animal facility for routine postoperative care and husbandry.
Nonrodent Studies
Our lab also routinely performs thoracotomies in New Zealand white rabbits for an established coronary ligation model. After completion of rodent studies with the Fugo blade, we evaluated the M100 unit for its cutting and dissection properties in six of this much larger animal. Again, using the customized tip for skin incision, a left lateral thoracotomy was performed through a left anterior lateral chest-wall incision. The underlying latissimus dorsi and serratus anterior muscles were dissected and divided in layers and the thoracic cage was entered through the seventh intercostal space using the modified, 400-µm straight tip. Once the interthoracic procedure was complete, the chest cage and chest wall muscles and the skin were closed in layers using running absorbable sutures. Animals were allowed to recover in a dedicated, warm postoperative cage and then returned to the animal facility for routine postoperative care and husbandry.
Results
In all animal experiments the Fugo blade provided clean, precise, cutting and tissue ablation. All animals, both rodent and nonrodent, survived the operations and made a complete recovery. At 2 weeks, after surgery all animals were killed and underwent autopsy. The skin incisions were excised and evaluated for tissue integrity and completeness of wound healing. There was excellent tissue recovery and integrity at 14 days in all animals with histology revealing only moderate inflammatory response in the areas of suture placement. In the rodent experiments, which are notably less sanguinous than larger animals, bleeding control was excellent, with virtually no hemorrhage noted or attributable to the Fugo blade. With regard to tissue incision, the Fugo blade was much superior to cold-instrument, blunt dissection, as it allowed exacting control over division of tissue planes without tearing. Upon entering the chest cavity proper, the fine 400-µm tip with the M100 set on the lower cut intensity setting allowed reproducible surgical entrance to the thorax without risk of injury to the underlying lung. In the rabbit experiments, the M100 unit performed very well for cutting and ablation but was unable to provide the same level of complete hemostasis as seen with the rodents. This was particularly true when dividing the larger diameter (>1 mm) crossing vessels and muscle perforators. However, this limitation did not pose any risk or threat to the animals or impede the success of the operations, as these vessels are easily controlled with the crush-clamp technique using a fine hemostat.
Summary
Not since the introduction of the Bovie by Dr. Harvey Cushing in 1926, has there been a widely applicable, safe, and efficient advance in electrosurgical technology such as the Fugo blade. As clearly demonstrated in the above preliminary experiments, the Fugo Blade is a scalable technology that can be used for surgical cutting and ablation in virtually any tissue and in any cavity of the body. The less-than-complete hemostasis seen in the rabbit model can be attributed to our use of a slightly modified M100 unit that was originally designed for the much smaller ocular space and for much finer and more delicate surgery. Had MediSurg, Ltd. made available a larger more powerful unit, we feel strongly that this larger vessel control would not have been an issue. In spite of this minor limitation, the “turbocharged” version of the M100 Fugo blade allowed precision cutting and ablation that is not otherwise available to the general or thoracic surgeon at this time. Probably the most promising aspect of the Fugo blade is found in its unique ability to cut effortlessly through tissues while minimizing the surrounding thermal injury. By design, the Fugo blade cuts only in the most focused part of the plasma cloud that is generated mere micrometers from the activated tip surface. This is quite a contrast from standard electrosurgical units that are based on diathermy, and trade off what can sometimes be extensive thermal injury for cutting and hemostasis. In summary, these proof-of-concept small animal studies demonstrate that the Fugo blade can be successfully scaled for use in nonocular applications in general and thoracic surgery.
Suggested Reading
Fugo RJ, Singh D, Fine IH. Automated Fugo blade capsulotomy: a new technique and a new instrument. Eyeworld. 2002;7:49–54.
Massarweh NN, Cosgriff N, Slakey DP. Electrosurgery: history, principles, and current and future uses. J Am Coll Surg. 2006;202:520–530.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


