 he objective of this chapter is to present a filtration procedure capable of achieving pressure stability without the need for medication or daily monitoring, while minimizing the incidence of complications such as shallow anterior chamber, hyphema, hypotony, and the concomitant use of antimetabolites. In our attempts to maintain the technical ease of the Singh filtration procedure and minimizing the incidence of complications and failure, the best outcome occurred when combining transciliary filtration (TCF) and microtrabeculectomy into one procedure while using Fugo blade technology. Previous attempts at microtrabeculectomy with Holmium lasers and minishunts were riddled with complications such as a flat or shallow chamber. When combining TCF with microtrabeculectomy, microfiltration is achieved with revolutionary success and no impediments.
he objective of this chapter is to present a filtration procedure capable of achieving pressure stability without the need for medication or daily monitoring, while minimizing the incidence of complications such as shallow anterior chamber, hyphema, hypotony, and the concomitant use of antimetabolites. In our attempts to maintain the technical ease of the Singh filtration procedure and minimizing the incidence of complications and failure, the best outcome occurred when combining transciliary filtration (TCF) and microtrabeculectomy into one procedure while using Fugo blade technology. Previous attempts at microtrabeculectomy with Holmium lasers and minishunts were riddled with complications such as a flat or shallow chamber. When combining TCF with microtrabeculectomy, microfiltration is achieved with revolutionary success and no impediments.
The key to the procedure is that aqueous drainage from the posterior chamber of the eye changes the force vector dynamics of the aqueous such that minimal force pushes the iris forward, thus preventing an anterior chamber collapse. Furthermore, the TCF pore is placed behind the iris root through the pars plicata. As the eye pressure increases, the pars plicata is stretched, thereby opening the TCF pore and increasing aqueous flow. When the intra-ocular pressure (IOP) decreases, the pars plicata tissue becomes flaccid and partially collapses over the TCF ostomy opening, thereby slowing aqueous outflow. Thus, the posterior chamber TCF ostomy acts as an autoregulatory valve.
Our approach (the Atwal balanced approach, or ABA) can be performed in patients with phakia or pseudophakia. The best results were obtained with phaco-emulsification and subsequent ABA filtration in a combined procedure; this combination comprised the bulk of our study.
The benefits of finding a procedure that can effectively eliminate the need for glaucoma medications are numerous. It is estimated that 25% of patients with glaucoma do not take their medications at all, and a large percentage do not adhere to their entire prescription regimen or do not follow their course of therapy properly. It has been suggested that this noncompliance is a leading cause of blindness from glaucoma. Eliminating medication entirely or getting ocular pressure under control greatly improves the prognosis. This is especially true in the enormous third world nations, where even the cheapest medication is often not affordable.
Reasons for noncompliance with topical medications for glaucoma are numerous and include cost, poor memory, difficulty with lifestyle, the patient “giving up,” poor finger dexterity, difficulty in mobility to gain access to medication, low intellect, and depression. The incidence of glaucoma is age-related. As our population ages, the incidence of glaucoma increases. The cost of eye drops is rather substantial, and when patients are on multiple-drop therapy, the regimen becomes such an encumbrance that they are often caught between paying for their eye drops or paying the rest of their bills. Such economic challenges along with issues of physical dexterity and other limitations present a major encumbrance for long-term compliance with an eye drop regimen. Glaucoma is the leading cause of blindness worldwide, with an incidence of 4.5 million patients per year.1 For this reason, the World Health Organization has placed a major emphasis on a global effort to combat loss of vision caused by glaucoma.1
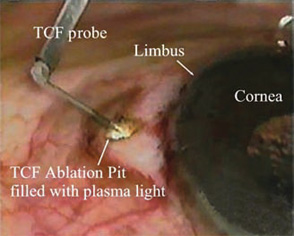
Figure 28.1. A standard TCF ablation pit is being created through sclera and pars plicata into the posterior chamber of the eye. Notice the light generated at the TCF ablation site by the Fugo blade plasma cloud. This ablation takes just seconds to perform.
The ABA procedure is a modification of the U.S. Food and Drug Administration’s (FDA) approved filtration procedure named after Dr. Daljit Singh of Amritsar, India, also called “Singh filtration” or “transciliary filtration” (TCF)2,3 (Fig. 28.1). In this procedure, Dr. Singh used the eximer-laser–like qualities of the Fugo blade to ablate tissue with minimal energy (less than 3 W) while leaving pristine ablation incision walls.4 TCF had been performed at our facility, and it was our opinion that TCF was successful in reducing eye pressure while eliminating flat anterior chambers because the aqueous fluid was drained from the posterior chamber of the eye, thereby relieving force vectors on the posterior surface of the iris. For this reason, it became clear that TCF was successful because it balanced the pressures between the posterior chamber and the anterior chamber better than the trabeculectomy procedure, which still suffers from flat anterior chambers. We modified the TCF procedure to create the ABA in an attempt to refine and improve the balance of pressure between the posterior and anterior chambers of the eye and achieve a higher and longer-term success rate.3 The ABA procedure uses the standard TCF procedure followed by a Fugo blade ablation minitrabeculectomy/minitrabeculostomy into the anterior chamber angle, under a standard scleral flap. The entire surgical procedure takes less than 5 minutes and produces minimal tissue trauma. And because minimal tissue is traumatized, minimal eye inflammation is produced.
Materials and Methods
We evaluated whether the ABA procedure could provide IOPs equal to or lower than the those achieved when maximal medical therapy was indeed being practiced by patients. These patients had documented poor compliance during the previous year, with subsequent progression of glaucoma damage. Also all patients are non-compliant with drops at one time or another.
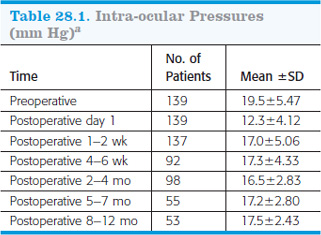
Patients were evaluated preoperatively and 1 day, 1 to 2 weeks, 4 to 6 weeks, 2 to 4 months, 5 to 7 months, and 8 to 12 months postoperatively. Surgical complications as well as postoperative complications were documented.
Statistical analysis was performed by obtaining p values. A test statistic was generated by comparing the group arithmetic mean divided by the sum of the group standard error values. The test statistic achieved was then plotted on a standard normal Z distribution curve, wherein a p value was calculated.
The ABA procedure was performed using the FDA-approved Fugo blade unit manufactured by Medisurg, Ltd. of Norristown, PA (Fig. 28.2). The Fugo blade is currently FDA-approved for capsulotomy, TCF for glaucoma, iridotomy formation for glaucoma, anterior chamber intra-ocular lenses, and the implantable contact lens. The Fugo blade is a low-powered monopolar electrosurgical unit that ablates tissue much like a mini-eximer laser rather than producing a cautery action.4 The unit produces a 100- µm thick plasma cloud on a blunt hair-thin cutting filament (Fig. 28.3).
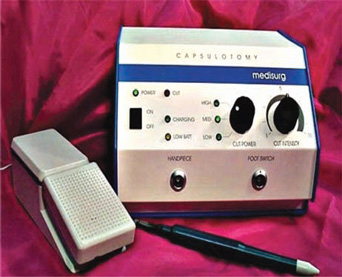
Figure 28.2. The Fugo blade unit consists of an electronic console, an ergonomic handpiece, and an activation foot switch.
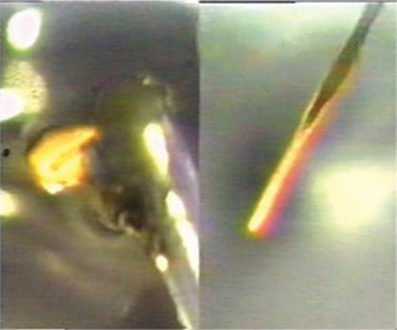
Figure 28.3. This image demonstrates an activated Fugo blade ablation tip. The tip is blunt and as thin as a human hair. The image on the left demonstrates light being emitted from the 100- µm thick plasma cloud. The image on the right filters out the light, thereby exposing the 100- µm thin plasma cloud that coats the blunt cutting filament. This plasma is nonarcing, but rather has a calm nature.
TECHNIQUE
Surgical Technique
- Make a 600- µm-diameter ablation pit 1 to 2 mm behind the limbus until the darker ciliary body is seen (Fig. 28.4).
- With the thin Fugo blade tip, enter the posterior chamber through the pars plicata. This creates a 200- µm ablation path through which aqueous percolates (Fig. 28.5).
- At this stage, with the same thin Fugo tip, create a microtrabeculectomy anterior to the TCF from the base of the scleral flap and through the trabeculum in the anterior chamber (Fig. 28.6). Aqueous percolates much faster through the microtrabeculectomy site.
- Then push the scleral flap back into position without sutures.
- Suture back the conjunctival peritomy with two 10-0 nylon sutures or just cauterize at either end.
- Patch the eye overnight.
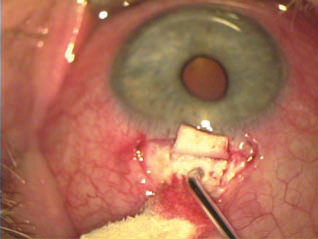
Figure 28.4. Creation of scleral ablation pit with activated Fugo blade tip.
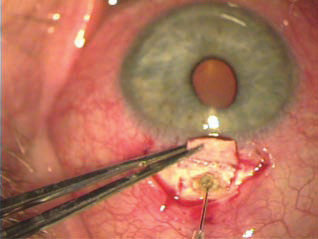
Figure 28.5. Fugo blade tip ablating through sclera and pars plicata into the posterior chamber.
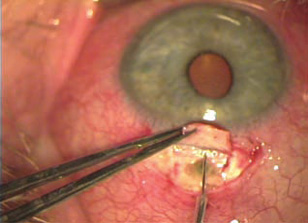
Figure 28.6. Fugo blade tip ablating through trabeculum into the anterior chamber.
Postoperative Management
Postoperative management is no different than that for cataract/intra-ocular lens procedures not using ABA.
Results
The mean (±SD) IOP on the first day after operation in the ABA group on no medical treatment was 12.3± 4.12 mm Hg. An important clinical observation in this group was the lack of anterior chamber collapse. In several of the patients, there was mild shallowing of the anterior chamber; however, this was not significant enough to elicit peripheral anterior synechia or endothelial touch. All chambers had deepened by 1 week after surgery. In five patients, we had a small amount of anterior chamber blood that produced less than a 1-mm hyphema. This resolved with conservative therapy and without incidence. Spaeth et al.5 demonstrated that trabeculectomy IOPs stabilized by 1 month after surgery. In actuality, the data from Spaeth et al. documented IOPs at 3 days and then at 1 month after surgery. Here, we document results 1 day, 1 to 2 weeks, 4 to 6 weeks, 2 to 4 months, 5 to 7 months, and 8 to 12 months after surgery (Fig. 28.7 and Table 28.1). We found that the ABA pressure stabilized at 1 to 2 weeks postoperatively. Our 1-to-2 week postoperative IOP mean was 17.0 ±5.06 mm Hg. When the Spaeth et al. data were compared with the present study, we found that there was no statistically significant difference between the primary glaucoma group treated with trabeculectomy in the Spaeth study at 1 year after surgery as compared with the ABA study at 8 to 12 months after surgery (p > 0.05). On the other hand, when we compared the primary glaucoma group and the secondary glaucoma group treated with trabeculectomy in the Spaeth study and the present ABA study, we found that the Spaeth study demonstrated a statistically significantly higher 1-year IOP, with an arithmetic mean of 21.2 ± 9.8 mm Hg (p < 0.01).
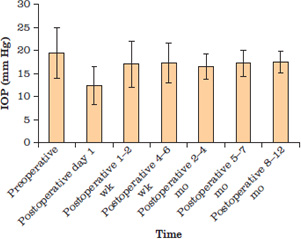
Figure 28.7. Average IOPs after ABA (arithmetic mean±SD) preoperatively and at various intervals postoperatively.
Complications in our study included five <1-mm hyphemas; these resolved with conservative therapy. In two eyes, small choroidal effusion occurred, which resolved spontaneously. Several patients had only minor anterior chamber shallowing, which resolved over the first postoperative week. During the course of the year, 9 of the 139 eyes needed topical eye drops added to their course of treatment in order to further reduce the IOP. To a large extent, these eye drops were added in eyes that had extremely advanced glaucomatous disc changes.
As with the Singh procedure, ABA places a precise TCF ablation pore through sclera into the posterior chamber of the eye. It should be noted that anatomic landmarks were initially used to locate the exact spot immediately behind the iris to ablate an ablation pore, although some may find it useful to locate the exact spot of the ablation site by using anterior chamber transillumination. The secret of TCF is that it decompresses aqueous from the posterior chamber of the eye through the pars plicata and the sclera. In this way, the force vectors are better equalized in the anterior and posterior chambers of the eye based on Bernoulli’s principle of fluid dynamics. The idea of modifying TCF to create the ABA procedure was based on the observation that this balancing of pressure produced fewer complications, since aqueous force vectors were no longer directed exclusively at the TCF pore but were now divided and balanced between the TCF pore in the posterior chamber and the microtrabeculectomy in the anterior chamber. Therefore, it was hypothesized that an even more precise balancing of these pressures could potentially offer a higher success rate with a lower complication rate. For this reason, we decided to place the TCF pore immediately behind the iris under a standard trabeculectomy flap. The TCF pore ablation takes from 30 seconds to a minute to perform. Following the decompressive Fugo blade ablation ostomy into the posterior chamber of the eye, you take a standard 100- µm-diameter Fugo blade probe and position it at the base of the scleral flap. Then, you aim the ablation tip at the anterior chamber angle. You activate the Fugo blade and then perform a quick in-and-out maneuver to create a precise minitrabeculectomy ostomy into the anterior chamber. This procedure takes several seconds to perform.
After the TCF ablation into the posterior chamber, a fulminant ooze of aqueous is seen to exit through the TCF pore. Likewise, the minitrabeculectomy placed at the base of the scleral flap and into the anterior chamber angle produces fulminant flow from the anterior chamber of the eye. Thereby, ABA produces flow from both anterior and posterior chamber ostomy openings. This dual flow creates an ultimate balancing of pressures between the anterior and posterior chambers of the eye and produces pressure stabilization with little complication. Total surgical time is less than 5 minutes, and the procedure has been found to be minimally traumatic to the patient, largely because the size of the surgical site is so small. Unlike trabeculectomy, no sutures are used on the scleral flap.
The maximal ideal medical therapeutic baseline was found to be 19.5±5.5 mm Hg preoperatively. The IOP on postoperative day 1 was 12.3±4.12 mm Hg. This was comparable to the postoperative day 1 pressure in a standard trabeculectomy studies. For example, the classic study of Blondeau and Phelps demonstrated a postoperative day 1 trabeculectomy pressure of 12.1±11.6 mm Hg.6 The standard deviation in the trabeculectomy in the study of Blondeau and Phelps was higher because there was a much wider range of eye pressures in this group as compared with the ABA postoperative day 1 group. Sixty-eight percent of the Blondeau and Phelps group had an eye pressures from 0.6 to 23.8 mm Hg, whereas 68% of the ABA group had eye pressures from 8.1 to 16.5 mm Hg. Again, this demonstrates the control that is achievable when the pressures are balanced between the anterior and posterior chambers of the eye and substantially adds to the efficacy of the procedure. This demonstrates much higher hypotony in the trabeculectomy study group. The significance of the mean IOPs on postoperative day 1—12.2 mm Hg in the Blondeau and Phelps group versus 12.3 mm Hg in the ABA group—demonstrates a comparable overall effect of the procedures. However, a closer look at the standard deviation demonstrates that more precise control is achievable with the ABA procedure, which may be a factor in the relatively low incidence of postoperative complications. Unlike the Scheie procedure, which has been reported5 to have over a 50% flattening of the anterior chamber, not a single patient who underwent ABA had a flat anterior chamber after the procedure—139 prospective cases in this study. At the time of writing, we have yet to experience a flat anterior chamber with either pure TCF or the ABA procedure. It should be noted that only one case of a flat anterior chamber after TCF has been reported in large TCF series being conducted by Thomas Dow, Daljit Singh, and Richard Fugo (personal correspondence).
Postoperative stabilization of the IOP was shown to occur between 1 and 2 weeks postoperatively using the ABA procedure. This is essentially comparable to the works of Blondeau and Phelps6 as well as the classic work of Spaeth et al.,5 in which it was demonstrated that stabilization of IOP occurred between 1 and 3 months postoperatively.
The preoperative ABA data were then compared with the postoperative ABA data, including data for 1 to 2 weeks, 4 to 6 weeks, 2 to 4 months, 5 to 7 months, and 8 to 12 months postoperatively. Statistical analysis for all ABA data groups was performed using p values by correlating the test statistic to the corresponding Z distribution curve. This demonstrated that there was no statistical significance (p > 0.05) between the 1-to-2-week, the 4-to-6-week the 2-to-4-month, the 5-to-7-month, and the 8-to-12-month postoperative ABA data. This essentially agrees with published trabeculectomy and thermosclerostomy results.6 The 8-to-12-month data demonstrated a mean IOP of 17.5±2.4 mm Hg. This was comparable to the 1-year trabeculectomy data of Blondeau and Phelps, which was 17.1±7.4 mm Hg. The ABA results also corresponded well with the 1-year postoperative results of the Spaeth et al. group with primary glaucoma treatment with trabeculectomy, which was 16.1±4.5 mm Hg. In both cases, the ABA data were statistically compared using p values correlating the test statistic to the corresponding Z distribution chart for 1-year data. The IOPs were found to be equivocal and statistically nonsignificant (p > 0.05). It should be emphasized, however, that both trabeculectomy studies demonstrated significantly higher standard deviations; therefore, there was a subsequent increase in variability on the high side and the low side for both trabeculectomy groups. This results in more patients with elevated IOPs as well as more hypotony. We believe that the lower standard deviation for ABA is based on the balanced-pressure dynamics established between the anterior and posterior chambers due to the dual filtration system created during the ABA procedure.
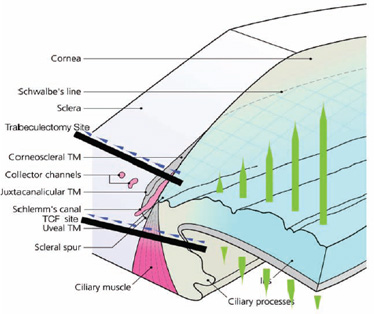
Figure 28.8. By performing trabeculectomy with TCF, we balance out the opposing forces, and obtain the benefits of both procedures.
The preoperative maximal ideal medical therapeutic baseline and standard deviation for the ABA procedure was compared with all of the postoperative categories that were tabulated for the ABA group. It was found that the values for all of the postoperative groups were statistically lower than the preoperative groups. Deriving these results from our data pool was based mainly on the relatively large sample size as well as the low standard deviations that were achieved. It should be emphasized that this demonstrates that the ABA procedure produced consistently lower eye pressures than were achieved by preoperative maximum medical therapy, which was strictly enforced preoperatively. In some cases, eye pressures may drop after cataract surgery for reasons such as low-grade iritis. However, a consistent drop of IOP after ABA with such tight standard deviation values is most unlikely as a secondary consequence of cataract surgery, especially with the relatively large sample size that was evaluated. Therefore, it is almost certain that the positive effects experienced and measured statistically are based on the positive effects of the pressure balances achieved with the ABA procedure (Fig. 28.8). Nine of the 139 patients had topical medications instituted during the course of a 1-year follow-up. This represents only 6.5% of the total test group; 3 of the patients had two eye drops added, and the remaining 6 had one eye drop added. It is likely that these patients will continue on the path of noncompliance. If significant progression in glaucoma is observed in this eye drop group, the patients will probably be considered for a repeat ABA procedure based on therapeutic noncompliance.
A point of interest to practitioners is the through-and-through ostomy created with the ABA procedure. One might hypothesize that such through-and-through openings would produce intractable hypotony. This is not the case. As a matter of fact, as we explained with the 1-day postoperative data, we have mean values comparable to those obtained with trabeculectomy; however, less hypotony was measured based on the lower standard deviation in the ABA study.6
The TCF ostomy is an opening through the pars plicata of the eye. As the eye pressure increases, the eye becomes tense, thereby causing stretching of the tissue, which results in the TCF pore opening more widely and allowing more aqueous fluid to escape. As the eye pressure decreases, the eye wall becomes more flaccid and the dynamics of the pars plicata come into play. The pars plicata actually droops or herniates into the ostomy opening, thereby reducing the aperture size of the ABA/TCF pore. Therefore, these ablation pores are not static, as would be seen if the eyeball were fabricated from material such as plastic. Rather, the eyeball is living tissue that has dynamics based on the physiologic characteristics of the eye, thereby producing the autoregulatory mechanism that controls and regulates the outflow of aqueous fluid. This effect is demonstrated in our postoperative day 1 data, which shows mean IOPs comparable to those for trabeculectomy studies, but with a lower standard deviation and therefore more IOP stability with less hypotony.6 This autoregulatory mechanism has been substantiated by Dr. Steven Gross, a veterinary ophthalmologist in Philadelphia. Gross has performed numerous TCF procedures in dogs with glaucoma. (Dogs have much thicker ciliary bodies than humans.) Gross places a 600- µm pore through the ciliary body and has not reported hypotony as a significant problem in his surgeries because of the herniation of the ciliary body into the 600- µm TCF pore when the IOP decreases.
It should be emphasized that a very delicate handling of the conjunctiva is imperative in order to minimize trauma to the conjunctiva. In this way, the conjunctiva remains healthy and effective in aqueous removal into the circulatory system. Therefore, the postoperative bleb will not be bullous, but rather will be low and smooth, thereby creating an excellent barrier to infection and a nontraumatized, comfortable bleb that may work efficiently for many years.
Two eyes in our study group had small choroidal effusions, which resolved spontaneously. Five had a 10 to 15% hyphema, which also resolved without consequence. In retrospect, some patients abuse aspirin and nonsteroidal anti-inflammatory drugs (or NSAIDs) for pain such as arthritis. Furthermore, many popular homeopathic herbs and remedies—such as fish oil, flax oil, ginkgo, green tea, beta carotene, vitamin A, vitamin C, vitamin E, and garlic—reduce blood coagulation. Three filters were complete failures (i.e., no bleb formation with IOP elevation >25 mm Hg) in eyes that underwent ABA for uncontrolled pressure under maximum medical therapy.
Simplicity is the ABA procedure’s true asset. We have been able to eliminate or minimize medications for the majority of our patients using a procedure that effectively takes only minutes to perform and is truly cost-effective.
Summary
Our study provides a step-by-step outline on how the ABA procedure is performed and demonstrates statistically the safety and efficacy of the ABA procedure. This prospective study demonstrates that a procedure that takes <5 minutes and has low postoperative complications has the ability to lower the IOP more than maximum medical therapy. The ABA procedure also demonstrates eye pressure control that is comparable to that achieved with trabeculectomy. The difference between ABA and trabeculectomy is that the ABA procedure can be performed much more quickly, has relatively few side effects, and has a lower IOP standard deviation than has been cited in classic trabeculectomy studies. The basis of this excellent eye pressure control, low postoperative complication rate, and lower standard deviation in eye pressure is the precise balancing of IOP forces between the anterior and posterior chambers of the eye while achieving an overall lower IOP. For these reasons, we believe that the ABA procedure is a realistic candidate for the management of glaucoma worldwide.
References
1. World Health Organization. Socio economic aspects of blindness and visual impairment. Geneva, Switzerland: World Health Organization. Accessed January 9, 2007, at http://www.who.int/blindness/economy/en.
2. Singh D, Singh K. Transciliary filtration using the Fugo blade. Ann Ophthalmol. 2002;34:183–187.
3. Atwal A. “Atwal’s balanced approach” for glaucoma filtration surgery presented. Ocular Surg News. 2005;19: 64–66.
4. Fine IH, Hoffman RS, Packer M. Highlights of the 2002 ASCRS Symposium, Part I. Eyeworld. 2002;7:38.
5. Spaeth GL, Joseph NH, Fernandes E. Trabeculectomy: a reevaluation after three years and a comparison with Scheie’s procedure. Trans Am Acad Ophthalmol Otolaryngol 1975;79:349–361.
6. Blondeau P, Phelps CD. Trabeculectomy vs thermosclerostomy: a randomized prospective clinical trial. Arch Ophthalmol. 1981;99:810–816.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


