 ysticercus cellulosae, the larval form of the pork tapeworm Taenia solium, is the causative organism of cysticercosis. Humans are the intermediate hosts in this organism’s life cycle. Cysticercus cellulosae may become encysted in various tissues, usually the eyes, central nervous system, and subcutaneous tissues. An immunologic reaction with fairly intense inflammatory signs and symptoms may be produced, and the surrounding structures may be compressed. This disorder is common in countries with people living in conditions of poor hygiene.
ysticercus cellulosae, the larval form of the pork tapeworm Taenia solium, is the causative organism of cysticercosis. Humans are the intermediate hosts in this organism’s life cycle. Cysticercus cellulosae may become encysted in various tissues, usually the eyes, central nervous system, and subcutaneous tissues. An immunologic reaction with fairly intense inflammatory signs and symptoms may be produced, and the surrounding structures may be compressed. This disorder is common in countries with people living in conditions of poor hygiene.
Ocular cysticercosis may be extra-ocular or intraocular. Depending on the location, different symptoms and signs arise. Cysticercosis of the subconjunctival or extraocular muscle presents as a painful, yellowish, nodular subconjunctival mass with surrounding conjunctival congestion. The tissue reaction creates a fibrous wall around the cyst, which becomes thicker over time.
Only the accessible subconjunctival or extraocular muscle cysticercus can be surgically removed. Because the cyst usually adheres to surrounding tissues, including the extraocular muscles, excision is difficult. And because the goal is to completely remove the parasite along with the cyst wall, bleeding and trauma to the tissues, including the extraocular muscle, are unavoidable. The extent of tissue trauma depends on the surgical tools used and the complexity of the case.
We have operated on four cases of cysticercus that were visible as subconjunctival swellings. Two case examples are described below.
CASE STUDIES
Case 1
The patient was a 10-year-old child who had increasing swelling and redness toward the medical canthus for over 2 weeks. The swelling was circumscribed and tender to the touch. The clinical diagnosis was cysticercus. Oral steroids were prescribed for 2 days before surgery.
TECHNIQUE
Anesthesia
The surgery was done under general anesthesia.
Surgical Technique
- Use the Fugo blade capsulotomy tip at the lowest energy settings. Hold the conjunctiva over the most prominent part of the cyst with a forceps. Make a tiny exploratory incision close to the forceps. The conjunctiva separate without any resistance or bleeding.
- Extend the incision cautiously into the cyst wall, up and down, going slightly deeper every time (Fig. 16.1) until the cyst eventually appears at the incision line. Very cautiously enlarge the incision further, until the cyst begins to extrude spontaneously from the incision. Make no attempt to grasp the cyst at this stage. When most of the cyst is out, hold it at the scolex with a plane forceps and remove it completely. No sutures are needed.
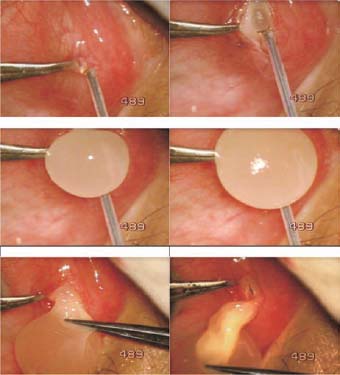
Figure 16.1. A 100-µm Fugo blade tip ablates the cyst wall, through which the cyst spontaneously extrudes. The final portion of the cyst containing the scolex is pulled out with a plain forceps.
As expected, our patient made a quick recovery. It could not be determined whether the cyst was connected with the extraocular muscle underneath. There was no way to know, since the surgery was performed right into the visible cyst wall.
Case 2
A 41-year-old patient presented with swelling in the eye for a year. He had a history of an episode of acute inflammation followed by swelling, for which he received some treatment. The acute inflammation recovered, but the swelling had remained. The patient was concerned because the swelling was unsightly.
TECHNIQUE
Anesthesia
Administer subconjunctival lignocaine 2%.
Surgical Technique
- In our case, the swelling was located toward the medical canthus. Because of the severe fibrotic reaction, we could not correctly locate the center of the cyst, so we made an incision parallel to the limbus and about 10 mm away from it failed to reveal the cyst. Clearly we had missed the cyst. We decided to cut the conjunctiva and look underneath.
- A large Fugo blade incision was made close to the limbus and the conjunctival edges were separated. We could now frankly palpate the cyst. An incision was made over it perpendicular to the limbus. The incision was right on the correct spot, because the cyst began to extrude, but it was firmly attached to the sclera and had to be removed in pieces.
- No adjacent tissue was excised and the conjunctiva was closed with sutures (Fig. 16.2).

Figure 16.2. The first vertical incision failed to expose the cyst. A large conjunctival incision was then made that located the cyst. The cyst was opened with a horizontal incision.
Postoperative Management
Our patient had an uneventful recovery.
Summary
The Fugo blade incises without causing bleeding. Its ablative cutting action is precise and allows the cystic balloon to extrude without rupturing. If further maneuvers to remove the cyst lead to rupture, the cyst can be easily removed in pieces.
Suggested Reading
Bansal RK, Gupta A, Grewal SP, et al. Spontaneous extrusion of cysticercosis: report of three cases. Indian J Ophthalmol. 1992;40:59–60.
Kapoor S, Kapoor MS. Ocular cysticercosis. J Pediatr Ophthalmol Strabismus. 1978;15:170–173.
Mohan K, Saroha V, Sharma A, et al. Extraocular muscle cysticercosis: clinical presentations and outcome of treatment. J Pediatr Ophthalmol Strabismus. 2005;42:28–33.
Murthy GR, Rao AV. Sub-conjunctival cysticercosis. Indian J Ophthalmol. 1980;28:77–78.
Sundaram PM, Jayakumar N, Noronha V. Extraocular muscle cysticercosis—a clinical challenge to the ophthalmologists. Orbit. 2004;23:255–262.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


