 ermoids are solid congenital tumors consisting of mesoblastic tissue covered by ectoderm and invaded by ectodermal derivatives. Dermoids may be small and superficial or large and likely deeper within the tissue. They may be located anywhere along the limbus, but they appear most commonly in the lower temporal quadrant. They are not uncommon. Because they are located on a vital thin corneal–scleral tissue and tend to grow over time, dermoids are best recognized and treated early.
ermoids are solid congenital tumors consisting of mesoblastic tissue covered by ectoderm and invaded by ectodermal derivatives. Dermoids may be small and superficial or large and likely deeper within the tissue. They may be located anywhere along the limbus, but they appear most commonly in the lower temporal quadrant. They are not uncommon. Because they are located on a vital thin corneal–scleral tissue and tend to grow over time, dermoids are best recognized and treated early.
Three approaches to managing dermoids are excision, excision with keratectomy, and excision with lamellar keratoplasty. The choice of surgery depends on the needs of the patient, the surgeon’s armamentarium and experience, and the availability of donor corneas. The aim of excision is total or subtotal removal of the dermoid, and it is done in such a way as to avoid perforating the cornea. The excision should be smooth enough so that the raw tissue can be covered with epithelium fairly quickly. We have been using the Fugo blade as one of the tools in excision. Two methods are described below.
TECHNIQUE
Anesthesia
Administer general anesthesia.
Surgical Technique
- For conjunctival tissue covering the dermoid: Puncture the conjunctiva covering the dermoid near the limbus with a 100-µm Fugo tip. Balloon the subconjunctiva with saline through a thin cannula. (Not using a needle for this purpose prevents subconjunctival hemorrhage.) See Figure 43.1.
- Incise the corneal edge of the dermoid with a 100-µm Fugo blade tip kept parallel to the cornea.
- Continue dissection toward the sclera, removing the middle and anterior bulk of the dermoid.
- Then cautiously remove the deeper layers, removing ever-finer slices each time. The corneal tissues will become visible. Determine the thickness of the underlying cornea by pressing with the tip of a forceps.
- Then remove the last remnants of the dermoid over the cornea as follows. Lift the finest layer with the tip of a needle and carry it toward the corneal edge of the lesion, which is excised along with it.
- Smooth the rough corneal and the scleral edges of the dissection with a 600-µm Fugo blade tip. Keep the activated tip moving under a stream of saline.
- Straighten the edge of the saved conjunctiva and sutured it at the limbus. Leave the raw area of the cornea alone to heal.
- For a dermoid devoid of conjunctival tissue, but with its skin (with or without hair): Balloon the conjunctiva around the dermoid. Incise it with a 100-µm Fugo blade tip and then elevate the conjunctiva with blunt scissors.
- Slice the dermoid with the Fugo blade. When more than half the thickness has been removed, use a scissors to remove the strip along the perimeter of the dermoid, including the strip on the cornea as well as on the sclera.
- Close any bleeding vessels with a 600-µm Fugo blade tip, operating under a stream of saline, finally obtaining a smooth surface on the cornea as well as on the sclera.
- Bring the undermined conjunctiva forward and suture it to the sclera as close to the limbus as possible. In less than 2 weeks, the raw area will be covered by the epithelial tissue (Fig. 43.2).
- For a dermoid devoid of conjunctival tissue, but with its skin (with or without hair): Balloon the conjunctiva around the dermoid. Incise it with a 100-µm Fugo blade tip and then elevate the conjunctiva with blunt scissors.
In our case of a limbal dermoid, scissors and Fugo blade tips were combined to remove the limbal dermoid efficiently and with minimum trauma.
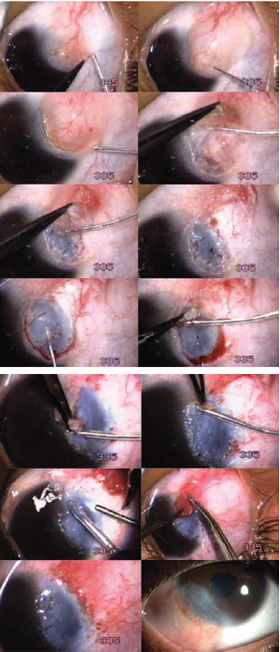
Figure 43.1. Dermoid excision in a 24-year-old patient. The conjunctival covering is ballooned, incised at the corneal end, lifted along with a bulk of the der- moid, and excised with the Fugo blade. The rest of the dermoid mass is excised carefully with the Fugo blade. The base is polished with 600-µm Fugo blade tip under a stream of saline. The conjunctival edge is trimmed, brought forward, and sutured at the limbus. The final image shows the condition of the eye 6 months after surgery.
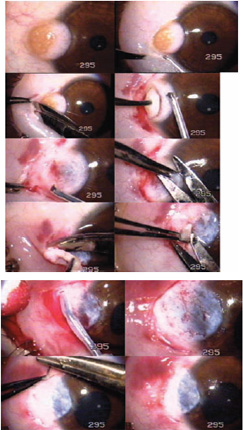
Figure 43.2. Dermoid excision in a 9-month-old patient. The conjunctiva is ballooned with saline and incised along the edge. Slices of the dermoid are removed, followed by excision at the edges with a scissors. The base of the dermoid over the sclera and the cornea is polished by a 600-µm Fugo blade. The conjunctiva is brought forward and sutured close to the limbus.
Postoperative Management
In all cases of dermoid excision, have the patient apply antibiotic–steroid ointment three times a day. The cornea will be covered with epithelium in about 2 weeks.
The final image in Figure 43.1 shows the condition of our patient’s eye 6 months later. There was no change in the best corrected vision of 6/18. The growing lesion is gone. If and when further cosmetic treatment is desired, tattooing or lamellar corneal grafting is available.
Summary
Every effort should be made to remove limbal dermoids completely. The last traces of dermoid tissue can be erased using a 600-µm Fugo blade tip. For those who like to simultaneously graft an amniotic membrane or to do a lamellar keratoplasty, the Fugo blade creates a smooth base for further treatment.
Suggested Reading
Mohan M, Mukherjee G, Panda A. Clinical evaluation and surgical intervention of limbal dermoid. J All India Ophthalmol Soc. 1981;29:69–73.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


