 o avoid complications of trabeculectomy, such as hypotony, flat anterior chamber, and choroidal detachment, Fyodorov et al.1 introduced an equivalent of deep sclerectomy. Kozov et al.2 proposed a similar operation plus a collagen drain to improve external filtration. In 1991, Stegmann3 proposed viscocanalostomy, which encompassed the injection of hyaluronic acid in both ends of the unroofed Schlemm canal. Since then numerous studies have been done, and nonperforating glaucoma surgery has become an important surgical technique for controlling glaucoma.
o avoid complications of trabeculectomy, such as hypotony, flat anterior chamber, and choroidal detachment, Fyodorov et al.1 introduced an equivalent of deep sclerectomy. Kozov et al.2 proposed a similar operation plus a collagen drain to improve external filtration. In 1991, Stegmann3 proposed viscocanalostomy, which encompassed the injection of hyaluronic acid in both ends of the unroofed Schlemm canal. Since then numerous studies have been done, and nonperforating glaucoma surgery has become an important surgical technique for controlling glaucoma.
Nonperforating glaucoma surgery (NPGS) is done under the highest magnification of the microscope. A steep learning curve to performing the surgery exists. Currently, all nonperforating procedures which does not allow the blade to enter the eye are guarded. Two scleral flaps are fashioned, the deeper of which is removed to expose the Schlemm canal to remove its lateral wall. The dissection is carried forward so that only the Descemet membrane separates the anterior chamber from the external drainage chamber.
My colleagues and I first performed nonperforating surgery with the Fugo blade on a 30-year-old woman who was 8 months pregnant. She had high myopia and pseudophakia, and her intra-ocular pressure was uncontrolled at 38 mm Hg. Surgical and postoperative complications were to be avoided at all costs.
The surgery was done with an 8X operating loupe (Zeiss) and illuminated with the operating microscope. The conjunctiva was detached from the limbus. The limbal tissue over the Schlemm canal was slowly ablated with a 600- µm Fugo blade tip until a fluid ooze was seen.
The conjunctiva was then sutured back in place. Five years later, the patient retains a thin bleb, and her intraocular pressure is 14 mm Hg. Figure 26.1 is a three- dimensional image of the patient’s present condition.
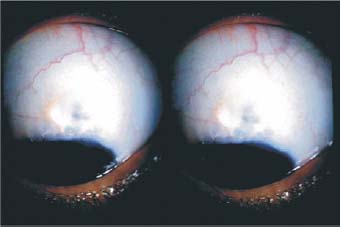
Figure 26.1. Three-dimensional image of an NPGS patient 5 years after surgery. The patient retains a thin bleb, and her intra-ocular pressure was reduced by more than 50% after surgery.
Since performing this procedure we have done numerous nonperforating operations in selected cases. Our surgical technique involves opening the Schlemm canal to the tissues under the conjunctiva. Success depends on the outflowing aqueous making its way to the subconjunctival drainage system. The following cases show how Fugo blade ablation can remove tissue to reach the desired depths accurately. This can be done without manual dissection, which requires high magnification.
Case 1: Blunt Trauma with Lens Subluxation
A 23-year-old patient presented several days after suffering a blunt injury that caused subluxation of the lens and an intra-ocular pressure >50 mm Hg (Fig. 26.2).
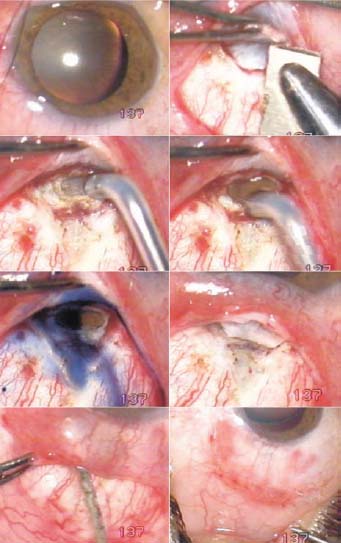
Figure 26.2. Trauma with lens subluxation (Case 1). A limbal-based conjunctival flap under which a triangular scleral flap reaches the limbus is seen. Ablation of limbus with a 600- µm Fugo blade tip opens the Schlemm canal. Aqueous movement is confirmed with a drop of trypan blue, the apex of the scleral flap is cut, the subconjunctival tissues are hydrated, and tenon capsule and conjunctiva are sutured separately.
Surgical Technique
- Under a limbus-based flap, make a triangular scleral flap that exposes the limbal area.
- Pass a 600- µm Fugo blade tip, set at low power and high intensity, lightly over the expected site of the Schlemm canal.
- After a few passes of the Fugo blade, the outer wall of the Schlemm canal is breached, as indicated by aqueous oozing. A drop of trypan blue will be washed away, proving aqueous flow.
- Remove part of the scleral flap. Hydrate the tenon capsule with saline before suturing it and the conjunctiva in separate layers.
Case 2: Uveitis and Glaucoma
A 40-year-old patient suffered chronic uveitis and secondary glaucoma that remained uncontrolled with medication (Fig. 26.3).
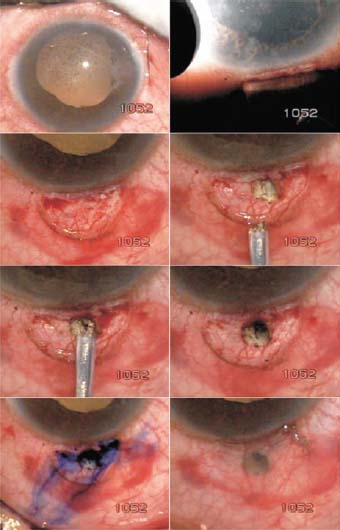
Figure 26.3. Chronic uveitis with uncontrolled glaucoma (Case 2). A fornix-based conjunctival flap is seen. Ablation of the limbus removes the lateral wall of the Schlemm canal. The aqueous flow is confirmed with the injection of trypan blue and the conjunctival flap is sutured.
- Transilluminate the limbal area to judge the location of the angle and the Schlemm canal.
- Make a 5-mm fornix-based flap to expose the limbal area.
- Perform ablation by sweeping a 600- µm Fugo blade tip from the limbus upward until the aqueous flows from the Schlemm canal. Confirm aqueous flow with a drop of trypan blue.
- Suture the conjunctival flap back in place.
Case 3: Open-Angle Glaucoma
To treat a patient with open-angle glaucoma, we used a spatulate form of the Fugo blade tip to do open ablation of the lateral wall of the Schlemm canal (Fig. 26.4), as in Case 2. Minimal dissection was required in this case. This case demonstrates how the Fugo blade can remove tissue without burning or charring.
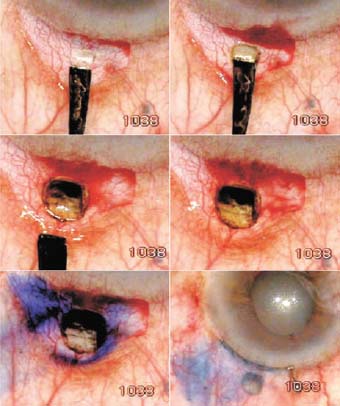
Figure 26.4. Open-angle glaucoma (Case 3). The lat- eral wall of the Schlemm canal is removed without making a scleral flap. The aqueous movement is confirmed with the injection of trypan blue, and the conjunctiva is sutured back.
Nonperforating Filtration Combined with Microtrack Filtration or Transciliary Filtration
If the aqueous ooze in NPGS appears less than satisfactory, or in the judgment of the surgeon the eye needs greater outflow of the aqueous, additional filtration routes can be added.
The limbus anterior to the nonperforating track can be undermined with a 600- µm Fugo blade tip, stopping just short of entering the anterior chamber. Creating this filtration area allows for filtration enhancement if necessary, by creating an opening using an yttrium–aluminum–garnet (YAG) laser. Or a track can be made right then and there with a 100-µm Fugo blade tip.
The area proximal to the area of nonperforating ooze can be thinned with a 600-m Fugo blade to reach the ciliary body. A 100-µm tip is used to make a track through the ciliary body into the posterior chamber (Fig. 26.5).
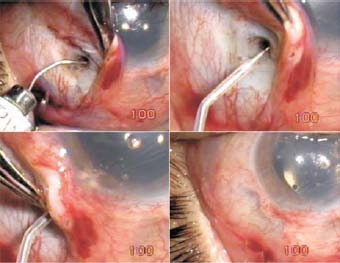
Figure 26.5. A fine cannula was introduced in the Schlemm canal, but fluid seepage was unsatisfactory. A 100-µm Fugo blade is directed toward the anterior chamber.
Summary
Nonperforating glaucoma surgery is not easy, and it has its complication. When manually removing fine tissues, perforations cannot be totally avoided. Successful NPGS depends on a number of factors, the most important being tissue reaction and scarring. However, the technique certainly has its merits. In some situations, any kind of perforating surgery, either in the anterior or the posterior chamber, is beset with risks. In these cases, NPGS is the best option. Use of the Fugo blade in NPGS allows the surgeon to ablate tissues in microscopic amounts in any standard or innovative manner to meet the needs of the case at hand.
Reference
1. Fyodorov SN, Kozlov VI, Timoshkina NT, et al. Nonpenetrating deep sclerectomy in open angle glaucoma. Ophthalmosurgery. 1990;3:52–55.
2. Kozlov VI, Bagarov SN, Anisimoba SY, et al. Nonpenetrating deep sclerectomy with collagen. Ophthalmosurgery. 1990;3:44–46.
3. Stegmann RC. Visco-canalostomy: a new surgical technique for open angle glaucoma. An Inst Barraquer. 1995;25:229–232.
Suggested Reading
Singh D, Fugo RJ. Glaucoma surgery techniques with the Fugo blade. In: Garg A, Fine IH, Pallikaris IG, et al., eds. Innovative techniques in ophthalmology. New Delhi, India: Jaypee, 2006:418–420.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


