 arcinoma in situ represents the malignant end of the spectrum of conjunctival dysplasias. The lesion may undergo spontaneous regression. It may start anywhere in the conjunctiva and cornea, but often starts at the limbus as an opaque, white, shiny, fleshy mass arising from the epithelium of the conjunctiva. It may present as a leukoplakia, a papilloma, or a complication of pterygium or pinguecula. The mass is similar to squamous epithelial lesions found elsewhere in the mucous membrane.
arcinoma in situ represents the malignant end of the spectrum of conjunctival dysplasias. The lesion may undergo spontaneous regression. It may start anywhere in the conjunctiva and cornea, but often starts at the limbus as an opaque, white, shiny, fleshy mass arising from the epithelium of the conjunctiva. It may present as a leukoplakia, a papilloma, or a complication of pterygium or pinguecula. The mass is similar to squamous epithelial lesions found elsewhere in the mucous membrane.
The basal membrane of the epithelium remains intact, and the subepithelial tissue is not invaded. Only infrequently does the lesion becomes invasive. Features include acanthosis, total loss of normal cellular maturation and cytologic atypia affecting the full thickness of the epithelium large and elongated tumor cells with the long axis of the cells oriented perpendicular to the basal lamina, and parakeratosis and mitotic activity in all layers.
Between 1999 and the present my colleagues and I have operated on three cases of carcinoma in situ, using the ablative properties of the Fugo blade to eradicate the last vestiges of diseased tissue. In one of these cases, the surgery had to be repeated.
CASE STUDY
The patient was 67 years of age. The lesion involved most of the limbus and the adjoining conjunctiva and cornea. The lower medial, upper medial, and lateral areas were particularly involved.
TECHNIQUE
Anesthesia
Administer surface anesthesia. Then puncture the conjunctiva with a 100-µm Fugo blade tip and inject 2% lignocaine with epinephrine through it using a blunt cannula to avoid possible subconjunctival hemorrhage from a needle prick. Balloon the conjunctiva with anesthetic fluid.
Surgical Technique
- Incise the conjunctiva 0.5 mm beyond the visible limit of the pathologic area using a 100-µm tip, to ensure that the incision does not go deeper than the conjunctiva. Lift the conjunctiva and also incise the subconjunctival tissue carrying the blood vessels. Ablating the blood vessels in the path of the incision ensures that no malignant cells are carried away. Lift the conjunctiva toward the limbus.
- Life the visible corneal presence of the lesion with a hockey-stick knife. After removing the diseased tissue, the base is ready to be cleaned.
- Smooth and clean the base using a 600-µm Fugo blade tip like an eraser. Set the energy at medium power and intensity. Apply the blade under a continuous saline stream, so that ablation and the clearing process are under greater control. Glide the activated tip over the surface of the sclera, the limbus, and the cornea, without pressing. Continue the process until a satisfactory surface appearance is achieved.
- Undermine the conjunctiva around the cut edge and bring it forward and suture it to the sclera, leaving the perilimbal area bare.
- Apply a bandage contact lens to reduce postoperative pain as well as to improve the efficacy of the local antimitotic drops (Figs. 13.1–13.3).
- Undermine the conjunctiva around the cut edge and bring it forward and suture it to the sclera, leaving the perilimbal area bare.
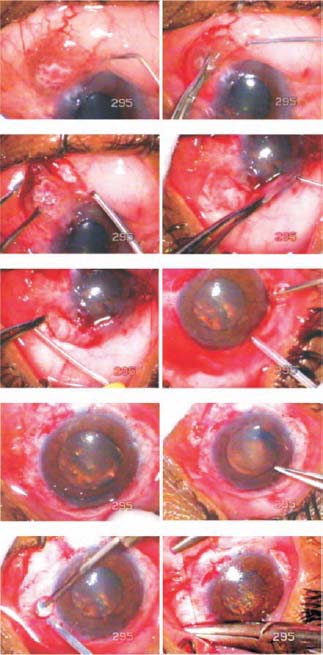
Figure 13.1. The conjunctiva is ballooned with local anesthetic. Incision is made with a 100-µm Fugo blade in the conjunctiva and excision is carried toward the limbus. Remaining tissue is ablated with a 600-µm Fugo blade tip under a stream of saline. The conjunctiva is brought forward and sutured some distance from the limbus.
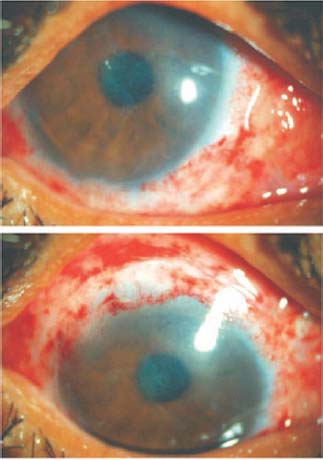
Figure 13.2. The appearance of the eye 4 days after surgery. The bandage contact lens is visible.
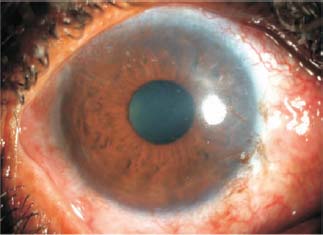
Figure 13.3. The same patient 1.5 years after surgery. The appearance of the eye is satisfactory.
Postoperative Management
Instruct the patient to instill local mitomycin drops 0.04% seven to eight times a day. These drops should be kept in a refrigerator and prepared fresh every third day. Continue the mitomycin treatment for 15 days. Concurrently, use local antibiotic–steroid ointment twice a day.
Summary
Using the Fugo blade to manage carcinoma in situ offers some advantages over the use of traditional instruments such as forceps, scissors, and cautery.
Tissue removal by ablation with the Fugo blade rather than raw cutting ensures that no pathologic cells escape via the blood vessels or the lymphatics. Furthermore, the finest remnants of the tumor on the sclera, limbus, and cornea are removed with greater confidence.
Suggested Reading
Kellan R, Fugo RJ. Device increases safety, efficiency of cataract surgery. Ophthalmol Times. 2000;25:7–9.
Roy FH. Course for Fugo blade is enlightening, surgeon says. Ocular Surg News. 2001;19:35–38.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


