 description of conjunctival lymphatics is important for this book, as some Fugo blade techniques for glaucoma are designed to minimize trauma to the lymphatics.
description of conjunctival lymphatics is important for this book, as some Fugo blade techniques for glaucoma are designed to minimize trauma to the lymphatics.The lymphatics are certainly present under the conjunctiva, because their existence can be demonstrated. They must be present in the orbit too, even if they cannot be seen. If no lymphatics existed in these sites, what would happen to a subconjunctival hematoma or to a large retrobulbar hemorrhage, say, after retrobulbar injection? Extravasated blood may not reenter the circulation through the venous capillaries; only in two ways can the blood return: quick return via lymphatics or a prolonged breakdown of the blood elements into basic elements, which are then absorbed. Venous capillaries cannot open up as lymphatics can.
The conjunctival lymphatics are orphan structures; they have not been adopted for study by most ophthalmologists, including glaucoma specialists. Key texts in the literature offer a narrow spectrum of views on ocular lymphatics, ranging from “the eye contains no lymphatics” to brief comments on ocular lymphatics, usually limited to fewer than a dozen sentences. Confusion stems from the fact that few have seen lymphatics. The ophthalmology community has a kind of “gut feeling” that they do not exist. The pathophysiology of ocular tissues is rarely if ever explained on the basis of the presence of lymphatics.
How can the eye manage fluid imbalance without the lymphatics? Consider the uveoscleral outflow that accounts for more than 50% of the aqueous outflow, and the leakage from the aqueous veins. Which system comes into play when filtration surgery is performed? Which system is to be blamed when a filtration operation fails? What produces large avascular blebs? These and many other questions can be answered if the presence and the function of the lymphatics is recognized.
We have studied lymphatics in trauma cases in the outpatient setting and in the operating room.
Conjunctival Lymphatics in the Outpatient Setting
The easiest way to study lymphatics is to observe the limbus through the high-power magnification of a slit-lamp microscope. The transparent lymphatics can be visualized, although they are hard to see at first. The definition is improved by the presence of pigment at the limbus. The lymphatics are more easily observed in dark-skinned people of all shades than in whites; because the white population generally lacks much pigment in the iris, its absence in the limbal area is to be expected. Acknowledging the presence of the lymphatics is the first step toward considering their role in the transport of aqueous in health and disease.
Raw lymphatics are frequently and easily recognized, once we know what they look like. These fairly large transparent structures run parallel to the limbus and give the conjunctiva a corrugated appearance (Fig. 25.1). The corrugated appearance is enhanced if the cornea is viewed under a slit-lamp.
The lymphatics at the limbus are fine channels running perpendicular to it. They are best visualized if some pigment is near the limbus. The general pattern is very apparent: vertical limbal channels flow into the the circular anastomosing channel network. The corneal ends of the limbal lymphatics seem to disappear and merge into a channel network in the cornea. See Figures 25.2 to 25.5 for examples.
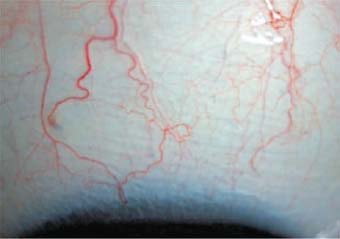
Figure 25.1. The raw lymphatics are visible as transparent channels running parallel to the limbus.
Frequently finds blood appears in the lymphatics as a result of trauma, including surgical trauma. The pattern of blood-filled lymphatics is very different from the pattern of arteries and veins with which we are all familiar (Fig. 25.6).
Conjunctival Lymphatics in the Surgical Setting
In the surgical setting, lymphatics can be demonstrated by injecting trypan blue into the periphery of the cornea. The dye soon spreads to fill the lymphatic network. The network is extensive in every case, but the extent of the network that can be visualized varies from patient to patient. The radial lymphatic vessels close to the limbus are thinner than the network of circular vessels proximally. One or more channels arise from this system and disappear toward the fornices (Fig. 25.7).
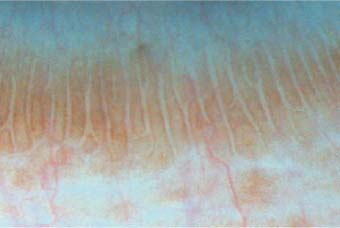
Figure 25.2. This image shows well-defined limbal lymphatics disappearing into the cornea at one end and merging with circularly running channels proximally.

Figure 25.3. A network of lymphatics that has been outlined by the limbal pigment outside the transparent vessels. The finer channels close to the limbus run perpendicularly. Proximally they join each other and the wider circular channels.
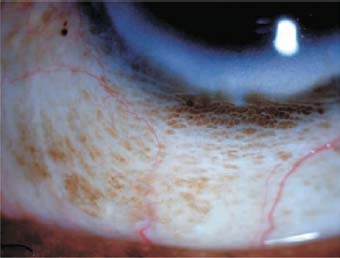
Figure 25.4. An extensive network of lymphatic chan- nels at and around the limbus, reaching toward the fornix.
Figure 25.5. Rivulets of lymphatics are clearly outlined by the pigment around the limbus. The blood vessels appear pale where they are crossed anteriorly by the lymphatics.
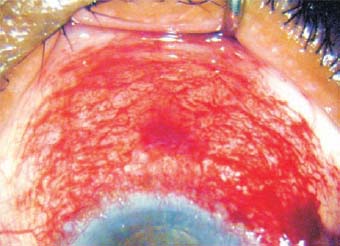
Figure 25.6. A surgical injury to a blood vessel at the 3 o’clock position starting to fill the lymphatics. In less than a minute, a large network of lymphatics became visible.
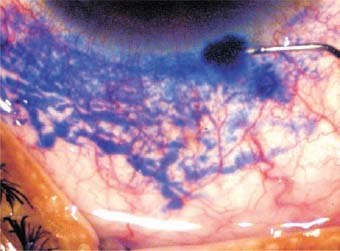
Figure 25.7. A network of lymphatic channels has become visible after injection of trypan blue into the periphery of the cornea.
In cases of failed glaucoma surgery, we have found that scarred areas do not display the lymphatics. Whatever type of surgery has been performed on the globe (e.g., strabismus, glaucoma, or retinal surgery) the lymphatics will be damaged at the incision and bipolar cautery sites. This is one good reason why tissues should be handled as little as possible in all kinds of operations. Glaucoma surgery is doomed if attempts are made to produce a drainage track in a previously handled area (Fig. 25.8).
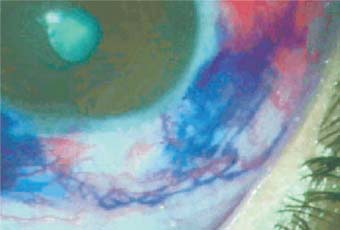
Figure 25.8. In failed surgery cases, the lymphatics are either absent or appear abnormal.
Relationship between Uveoscleral Outflow and Conjunctival Lymphatics
The literature is replete with information on uveoscleral outflow, but does not explain how and where this outflowing fluid is deposited. In one of our studies with trypan blue in a patient who had extensive scarring around the limbus, we found a startling connection between the sclera and subconjunctiva. Dye was injected into the sclera close to the limbus, traveled through the sclera, and appeared at multiple points around the limbus as blue blots and knots, indicating that the dye had traveled through some sort of channels inside the sclera. It also indicated that further connections of these blots were missing. However, when we looked at the conjunctiva proximal to the damaged area, we noticed that the conjunctival lymphatics had received the blue dye. We demonstrated this phenomenon in two more cases. How did an injection in the sclera fill the conjunctival lymphatics at such a distance? The only rational answer is that some form of three-dimensional network connects scleral lymphatics to the conjunctival network. And this raises another question: How does the uveoscleral outflow function? This scleroconjunctival connection suggests that not only mere diffusion but actual transport through normal existing channels may occur. Thus, uveoscleralconjunctival outflow may be as much a secure closed channel transport system as the Schlemm canal-aqueous vein (Fig. 25.9).
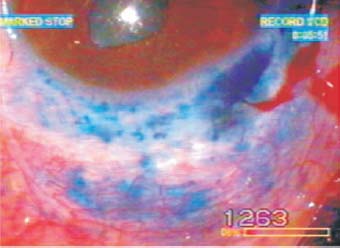
Figure 25.9. Extensive scarring appears around the limbus. Trypan blue injected near the damaged limbus has appeared in multiple blots along the limbus. But it has also filled up the proximal conjunctival lymphatics, proving the existence of channels directly connecting the scleroconjunctival system.
Summary
All evidence collected from our slit-lamp examinations and dye-injection studies indicates that an important three-dimensional lymphatic channel system exists under the conjunctiva and that it is connected to a similar scleral channel system. This lymphatic system is responsible for the drainage of normal outflowing aqueous. It can cope with the excessive fluid that drains after glaucoma filtration operations. Obstruction to free flow through the lymphatics results in the formation of blebs. Damage to the lymphatic system triggers subconjunctival fibrosis, which may become excessive and thereby jeopardize the successful outcome of a filtration operation. We believe that patients with glaucoma can be treated more successfully if the role of conjunctival lymphatics in aqueous drainage is taken into consideration when designing surgical techniques.
Suggested Reading
Bethke WC. A new clue to lymphatic drainage? Rev Ophthalmol. 2002;9:12.
Kent C. Revealed: the eye’s lymphatic system. Ophthalmol Manage. 2002;6:114.
Singh D. Conjunctival lymphatic system. J Cataract Refract Surg. 2003;29:632–633.
Singh D, Singh RSJ, Singh K, et al. The conjunctival lymphatic system. Ann Ophthalmol. 2003;3:99–104.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


