, Jacques Magnan3, Hassan Haidar4, Karen Nicolas5, 6 and Stéphane Louryan7
(1)
Hospital Sacre Coeur ORL Chirurgie Cervico – Faciale, Lebanese University, Baabda, Lebanon
(2)
ORL Chirurgie Cervico – Faciale, Hôpital Trad, Beirut, Lebanon
(3)
ORL – Chirurgie Cervico – Faciale, University Aix-Marseille Hôpital Nord, Marseille, France
(4)
ORL – Chirurgie Cervico – Faciale, Hôpital Nord, Marseille, France
(5)
Department of Radiology Middle East Institute of Health, Bsalim Levant Clinics, Fachaerztin fuer Radiologische Diagnostik Lebanese University, Beirut, Lebanon
(6)
Department of Radiology, Levant Clinics, Sinn el Fil, Lebanon
(7)
Laboratoire d` Anatomie Biomécanique et Organogenèse, Université Libre de Bruxelles Faculté de Médecine, Brussels, Belgium
1.1.3 The Viscerocranium
1.4.1 The Petrous Bone
1.4.2 The Squamous Bone
1.4.3 The Tympanic Bone
1.4.4 The Styloid Bone
1.4.5 Temporal Bone Fissures
1.4.6 Temporal Bone Surfaces
Abstract
Due to its multiple embryological origins and its adverse developmental aspects, the temporal bone is considered as one of the most complex anatomical structures of the human body. Since the middle ear lodges inside the temporal bone, this chapter will be mostly oriented, not to study the temporal bone as such, but to address it in a specific and restricted scope aiming to describe precisely the developmental and anatomical environment in which the middle ear achieves its final architecture.
The temporal bone houses various cranial nerves and inhabits different important vascular structures and many sensorineural organs in close contacts. Our target will be to demonstrate the richness of such critical structures along with their relationships around and inside the middle ear.
Due to its multiple embryological origins and its adverse developmental aspects, the temporal bone is considered as one of the most complex anatomical structures of the human body. Since the middle ear lodges inside the temporal bone, this chapter will be mostly oriented, not to study the temporal bone as such, but to address it in a specific and restricted scope aiming to describe precisely the developmental and anatomical environment in which the middle ear achieves its final architecture.
The temporal bone houses various cranial nerves and inhabits different important vascular structures and many sensorineural organs in close contacts. Our target will be to demonstrate the richness of such critical structures along with their relationships around and inside the middle ear.
1.1 Embryology of the Temporal Bone
Temporal bone formation results from the fusion and growth of four bones: the squamous, the petrous, the tympanic bones, and the styloid bones. These bones interact to build up the final temporal bone.
Being a part of the skull, temporal bone development is an integral part in the process of skull development. Human skull is developed from three components:
1.
The cartilaginous neurocranium or chondrocranium is the part of the skull formed by endochondral ossification; it constitutes the majority of the skull base (ethmoid bone and portions of the occipital, temporal, and sphenoid bones). Endochondral ossification takes place in a cartilaginous anlage; chondroblasts become hypertrophied and progressively change into osteoblasts, which elaborate the bony matrix. The corresponding area is the “ossification center.”
2.
The membranous neurocranium or neuroskull is the part of the skull formed by intramembranous ossification; it constitutes the vault of the skull (frontal, parietal portions of the temporal, occipital, and sphenoid bones). Intramembranous ossification happens when a cluster of mesenchymal cells in a membranous structure gives rise to osteoblasts, in the absence of any cartilaginous matrix.
3.
The viscerocranium or visceroskull is the part of skull derived from the branchial arches and is suspended to the rest of the cranium [1]. It includes the facial bones.
These three components of the skull contribute actively in the formation of the temporal bone in the following way:
The deep part of the petrous bone is derived from the cartilaginous neurocranium, but the more superficial parts are derived from the membranous neurocranium. The squamous bone is derived from the membranous neurocranium, and the tympanic bone is a part of the visceral skull [2].
1.1.1 Cartilaginous Neurocranium
The majority of the skull base develops from the cartilaginous neurocranium. The formation of the human skull base is a complex process that begins during the fourth week of fetal development. Neural crest cells and paraxial mesoderm derived from occipital somites migrate to sit between the emerging brain and foregut. These cells migrate around and in front of the notochord to form condensations accumulating within the emerging cranial base. The chondrocranium begins to form when these cells condense into cartilage early in the seventh week; these cells are named parachordal cartilages and contribute to the creation of the basal plate.
These parachordal cartilages give rise to the body, greater and lesser wings of the sphenoid bones as well as the perpendicular plate of the ethmoid and the crista galli. These embryonic cartilages fuse around the existing cranial nerves and blood vessels to create the primordia of neural foramina [3].
1.1.1.1 The Cartilaginous Otic Capsule
Between the eighth and ninth week of gestation, the cartilaginous otic capsule appears as budge in the base of the cartilaginous cranium. It develops from the mesenchymal tissue that surrounds the otic vesicle. Later the otic capsule becomes surrounded by membranous layers (internal and external periosteal layers); these layers will become the extracapsular part of the petrous bone [3] (Fig. 1.1).
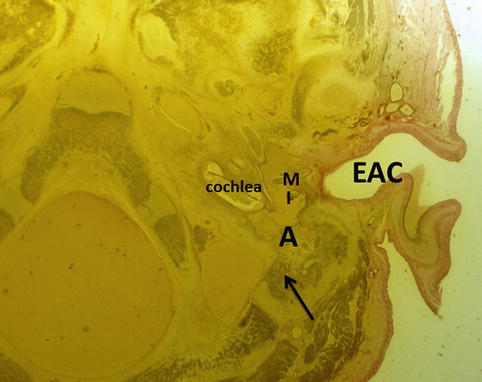
Fig. 1.1
The left temporal bone in a 6 months human fetus. The mastoid area contains external periosteal layer bone (arrow), will transform into mastoid bone. Notice that the mastoid antrum (A) and the cochlea are already developed. M malleus, I incus, EAC external auditory canal
Shortly after this process, the lateral and superior boundaries of the otic capsule begin to appear with the earliest development of the mastoid process and tegmen tympani [4]. A cartilaginous flange grows from the lateral and superior part of the otic capsule and goes downwards and outwards superior to the tubotympanic recess and above the Meckel’s cartilage to form the tegmen tympani and the lateral wall of the eustachian tube (ET) (Fig. 1.2) (see Sect. 2.4.1). Thus, the tympanic cavity and the bony part of the ET originate from the petrous bone. Furthermore, from the lateral and inferior part of the cartilaginous otic capsule, another flange grows below the tubotympanic recess to form the jugular plate and the floor of the tympanic cavity. Anteromedially, another periosteal layer grows to form the petrous apex (Fig. 1.2).
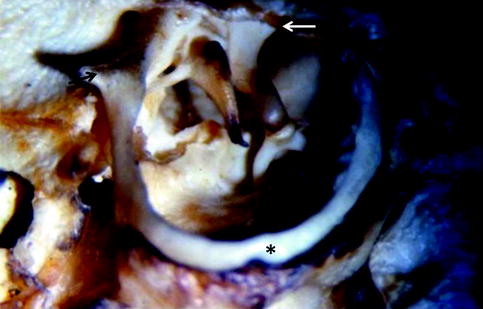
Fig. 1.2
Schematic drawing, frontal plane (34-week-old fetus). Schema showing the cartilaginous flanges running out from the otic capsule: (1) lateral and superior flange or the tegmental plate growing from the otic capsule superior to the tubotympanic recess (TR) to form part of the tegmen tympani and the walls of the Eustachian tube; (2) lateral and inferior cartilage flange, growing from the otic capsule to form the jugular plate and the floor of the tympanic cavity; (3) anteromedial flange growing from the otic capsule anteromedially to form the petrous apex. The inferior wall of the middle ear is built up by the inferior plate of the petrous bone (2) which runs laterally to join the tympanic bone (T); the plane of fusion constitutes the hypotympanic fissure(*). The tympanic bone (T) and the tympanic membrane (TM) form the lateral wall of the middle ear cavity. The tegmen tympani is formed by fusion of the tegmental process of the petrous bone (2) and the transverse plate of the squamous bone (4). M malleus, I incus, S stapes
By the 16th week, the labyrinth reaches its adult size. Only at this time, the first part of the petrous bone starts to ossify by the endochondral ossification process. There are 14 different ossification centers in the otic capsule, which progressively fuse during the fetal period [4].
The ossification proceeds and continues in the remaining part of the petrous bone to gain its final aspect by about midterm. By the 23rd week of gestation, the rest of the ossification process of the extracapsular parts of the temporal bone continues by extension of the surrounding periosteum forming the mastoid process, the tegmen tympani, middle ear floor, and the walls of the Eustachian tube (Figs. 1.2 and 1.3). The floor of the middle ear ossifies between the 24th and 29th week from an extension of the jugular plate ossification center [5]. Ossification of the otic capsule is completed only shortly before birth [5].
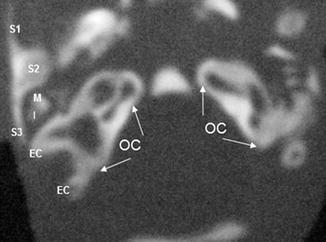
Fig. 1.3
Transversal CT scan of a 22-week-old fetus, showing ossification of the otic capsule (OC) and beginning of the ossification process in the extracapsular parts of the petrous bone (EC) extending to form the mastoid process. The inferior part of the squamous bone with its three parts: S1 anterior part forming the zygomatic process, S2 middle part forming the roof of the EAC and part of the tegmen, S3 the posterior part forming the anterior part of the mastoid process. Also notice that the petrous bone and the squamous bone are not yet fused. M malleus, I incus
1.1.2 Membranous Neurocranium and the Squamous Bone
The squamous part of the temporal bone develops from intramembranous ossification; it is formed from one ossification center that appears during the eighth week of gestation [8]. The development of the upper and lower halves of the bone primordium differs:
The upper part is flat and thin and will become the vertical portion.
The lower part, due to the presence of the tympanic bone by the 16th week, bulges and grows rapidly into three directions (Fig. 1.2):
1.
The anterior part extends anteriorly around the tympanic ring towards the zygomatic bone primordium. It is fixed to the anterosuperior part of the tympanic bone. It forms the zygomatic process of the squamous bone and is involved in the formation of the roof of the temporomandibular joint.
2.
The middle part sinks medially above the tympanic ring to form the superior wall of the external auditory canal, the attic outer wall, and the lateral part of the tegmen tympani [9].
3.
The posterior part extends posteriorly behind the tympanic ring to cover a major part of the base of the petrous bone. It forms the anterior portion of the mastoid process.
1.1.3 The Viscerocranium
1.1.3.1 The Styloid Process
The styloid process derives directly from the Reichert’s cartilage of the second branchial arch. It develops from two parts:
The proximal part or the base, also named the tympanohyale, is situated close to the tympanic bone. Its ossification center appears before birth and continues to grow until the age of 4 years. It fuses with the petromastoid component during the first year of life [10].
The distal part, the stylohyale, starts its ossification only after birth. It fuses with the proximal part only after puberty.
1.1.3.2 The Tympanic Bone
The tympanic ring is a C-shaped bone that provides physical support to the tympanic membrane. It is formed by intramembranous ossification (Fig. 1.4).
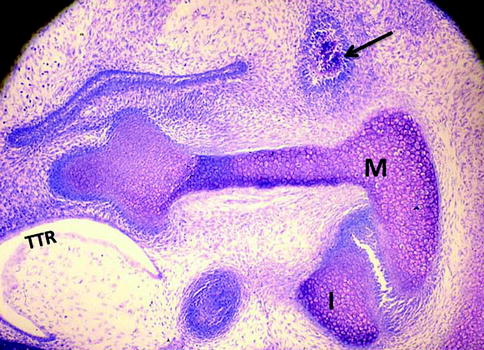
Fig. 1.4
An intramembranous area of ossification (arrow) corresponding to the tympanic bone in an E17 mouse embryo (sagittal section, toluidine blue). The cartilaginous primordial of the malleus (M) and incus (I) are also visible. Tubotympanic recess (TTR). Toluidine blue staining at pH4
At the eighth week of gestation, the tympanic ring appears as a condensation in the cephalic part of the mandibular part of the first branchial arch, which is situated ventral to the first pharyngeal cleft and lateral to Meckel’s cartilage. This condensation will extend in a circumferential fashion around the first pharyngeal cleft resulting in the C-shaped structure [11]. Within 2 weeks, the ossification is first detected in the part of the condensation adjacent to Meckel’s cartilage; then it progresses through the rest of the condensation to form a fully developed tympanic ring that is well recognized by the 11th week of gestation (Fig. 1.5).
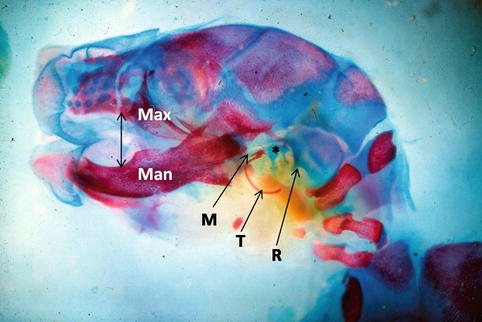
Fig. 1.5
Skeletal staining of a mouse E 16 embryo. In blue, the Meckel’s (M) and Reichert’s (R) cartilages appear in close relationship with the ossicles rudiment (*). In red, we can see maxillary (Max) and mandibular (Man) bones around the oral cavity (double arrow). The tympanic ring (T) is also red and ossifies following intramembranous process
At 12th week, growth of the tympanic ring proceeds rapidly with a consequent increase in its overall size. The tympanic ring is never closed superiorly, giving rise to the incisura tympanica (Rivinus notch) where the pars flaccida of the tympanic membrane will make insertion.
Fusion of the tympanic ring with the other components of the temporal bone starts first at 31st week in the posterior part. The anteromedial segment of the tympanic bone does not join the temporal bone until 37th week. Its fixation to the temporal bone is complete at birth.
The tympanic bone is 9 mm in diameter at birth, almost its definitive size. At this time, it is ring shaped and is open superiorly [12–16].
The formation of the external auditory meatus and the formation of the manubrium are in close association with the tympanic ring formation [11]. The tympanic ring plays an instructive role for the external auditory canal development. Very likely aural atresia results from the failure of the tympanic ring to develop [17]. In addition, the formation of the tympanic ring is essential for the insertion of the manubrium of the malleus into the tympanic membrane [18]. Several experimental conditions leading to a lack of external auditory meatus formation also result in a severe underdevelopment of the manubrium with a normal aspect of the rest of the malleus. This fact is confirmed in cases of major aural atresia, showing an absence of the manubrium with otherwise normal looking of the rest of the malleus [18, 19].
1.2 Perinatal Changes of the Temporal Bone
By the time the fetus has reached the perinatal period, the squamous and tympanic bones have already fused together; but the resultant segment is still separated from the petrous segment [20]. Early in the perinatal period, these two segments begin to fuse. The fusion of the two segments takes place simultaneously at several locations, beginning with the medial surface of the squamous part to the lateral edge of the tegmental process of the petrous bone. This zone of fusion becomes the internal petrosquamous suture [7]. The fusion continues posteriorly between the petrous and squamous parts of the mastoid process; failure of complete fusion of the two parts leads to formation of a bony septum inside the mastoid process, called Korner’s septum [21] (see Sect. 5.1.1). The external petrosquamous suture present on the outer surface of the mastoid process marks the plane of fusion between these two parts.
Finally, the inferior portion of the tympanic ring fuses medially to the inferior process of the petrous bone, thus forming the inferior wall of the tympanic cavity.
1.3 Postnatal Changes of the Temporal Bone
Expansion pressures and antagonist forces exerted by the cephalic neuroskull and the muscular visceroskull, in addition to the pneumatization process, are the main factors for the remodeling process and postnatal changes of the temporal bone.
Bone growth around the tympanic ring following its fusion to the petrous bone proceeds laterally around its circumference. This results in the development of the bony external auditory canal [22]. This lateral extension of the tympanic ring results from the growth of two tympanic tubercles, one from the anterior aspect of the ring and the second from the posterior aspect (Fig. 1.6). These projections grow laterally and then towards each other inferiorly to form the inferior wall of the external auditory canal. By doing so, these projections delimit two openings: the first is in the upper part, the notch of Rivinus, and the second is inferior, the foramen of Huschke [23].