, Jacques Magnan3, Hassan Haidar4, Karen Nicolas5, 6 and Stéphane Louryan7
(1)
Hospital Sacre Coeur ORL Chirurgie Cervico – Faciale, Lebanese University, Baabda, Lebanon
(2)
ORL Chirurgie Cervico – Faciale, Hôpital Trad, Beirut, Lebanon
(3)
ORL – Chirurgie Cervico – Faciale, University Aix-Marseille Hôpital Nord, Marseille, France
(4)
ORL – Chirurgie Cervico – Faciale, Hôpital Nord, Marseille, France
(5)
Department of Radiology Middle East Institute of Health, Bsalim Levant Clinics, Fachaerztin fuer Radiologische Diagnostik Lebanese University, Beirut, Lebanon
(6)
Department of Radiology, Levant Clinics, Sinn el Fil, Lebanon
(7)
Laboratoire d` Anatomie Biomécanique et Organogenèse, Université Libre de Bruxelles Faculté de Médecine, Brussels, Belgium
Abstract
The facial nerve, or cranial nerve (CN VII), is the nerve of facial expression. Due to various developmental events, the trajectory of the facial nerve, from its origin in the brainstem to the muscles of the face, is tortuous and complex. The ingenious pathway of the facial nerve through the middle ear and mastoid adds to the complexity and refinement of middle ear microsurgery. Thus, a thorough knowledge of the facial nerve anatomy along with its multiple landmarks is essential for an accurate, safe, and effective surgical intervention in the middle ear.
A basic understanding of the developmental anatomy is necessary to understand and anticipate the various anatomical situations encountered during ear surgery.
The facial nerve, or cranial nerve (CN VII), is the nerve of facial expression. Due to various developmental events, the trajectory of the facial nerve, from its origin in the brainstem to the muscles of the face, is tortuous and complex. The ingenious pathway of the facial nerve through the middle ear and mastoid adds to the complexity and refinement of middle ear microsurgery. Thus, a thorough knowledge of the facial nerve anatomy along with its multiple landmarks is essential for an accurate, safe, and effective surgical intervention in the middle ear.
A basic understanding of the developmental anatomy is necessary to anticipate the various anatomical situations encountered during ear surgery.
6.1 Facial Nerve Development
The development of the motor root of the facial nerve is independent of the development of the sensory root and the geniculate ganglion.
The facial nerve primordium is first recognized at the 4th week of gestation as a collection of cells at the vicinity of the auditory placode, which will generate the otocyst (Fig. 6.1). These cells are derived from neural crest cells and epibranchial microplacodes of the second branchial arch. Then, the facial nerve primordium extends to the primitive geniculate ganglion region as a narrow band; meanwhile, the acoustic nerve has reached the otocyst [1].
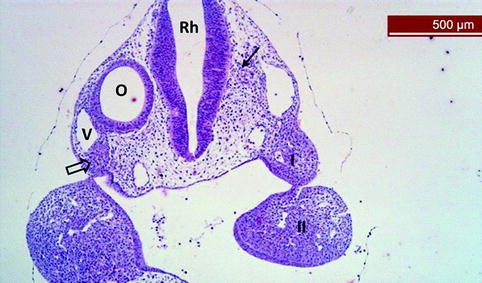
Fig. 6.1
Frontal (asymmetric) section of a head of a E9 mouse embryo. At the right side, we observe facial nerve fibers (arrow) in contact with the rhombencephalon (Rh). At the left side, rudiment of the geniculate ganglion is visible (large arrow) at the vicinity of the otocyst (O) and the anterior cardinal vein (V). I and II, first and second branchial arches
In the 5th week, the facial motor nucleus can be identified in the developing brainstem. Nerve fibers leave the nucleus and pass caudal to the region of the geniculate ganglion. These fibers bend dorsally to give the horizontal segment of the nerve which passes between the developing labyrinth and the upper end of the Reichert’s cartilage. The upper end of the Reichert’s cartilage will become the blastema of the stapes (Fig. 6.2). Finally the facial nerve bends vertically before passing into the substance of the second branchial arch, the laterohyale [1] (Fig. 6.3).
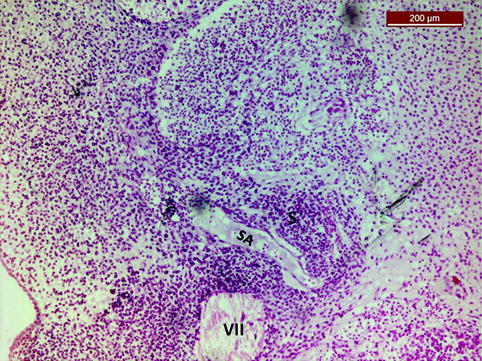
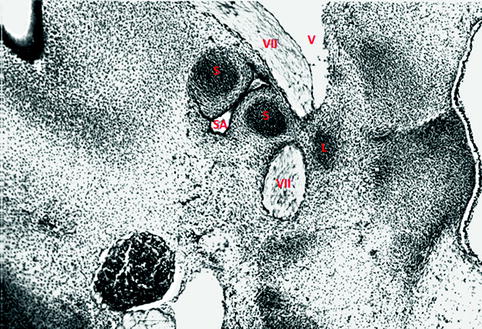
Fig. 6.2
Transverse section of a 13-mm human embryo, showing the close relationship of the facial nerve rudiment (VII) with the stapes (S) anlage, crossed by the stapedial artery (SA). Hematoxylin-eosin staining
Fig. 6.3
frontal section in a 15.5-mm human embryo. The facial nerve rudiment (VII) is partially covered by the laterohyale (L), derived from the Reichert’s cartilage, and crosses the stapes (S), itself traversed by the stapedial artery (SA). The anterior cardinal vein (V) is lateral to the nerve. Hematoxylin-eosin staining
In the 5th week, the chorda tympani is the first branch of the facial nerve to appear. At this time, the chorda tympani nerve and the facial nerve trunk are of approximately equal size; this state could be encountered clinically in adult ears with major atresia [2]. The chorda tympani nerve (Fig. 6.3) dives into the mandibular arch to terminate in the same region as the lingual nerve ends and where the submandibular ganglion develops. The chorda tympani nerve primordium divides the mandibular ossicular blastema into malleus laterally and incus medially. By the 7th week, however, the chorda tympani nerve is smaller than the facial nerve and remains so until adulthood [2] (see Fig. 3.2).
In the 7th week, the sensory root of the facial nerve (nervus intermedius) arises from the geniculate ganglion and runs between the motor root of the facial nerve and the cochleovestibular nerve on its way to the brainstem. At the same time the greater petrosal nerve, which is the second branch of the facial nerve to appear, develops from the anterior aspect of the geniculate ganglion.
The mesenchyme around the facial nerve develops later into the facial nerve canal. The first cartilaginous anlage of the facial canal derives from the laterohyale (Figs. 6.3 and 6.4). The development of the contiguous structures, such as the stapes, the labyrinthine capsule, the mastoid bone, and the tympanic bone, will determine the ultimate trajectory of the facial nerve canal.
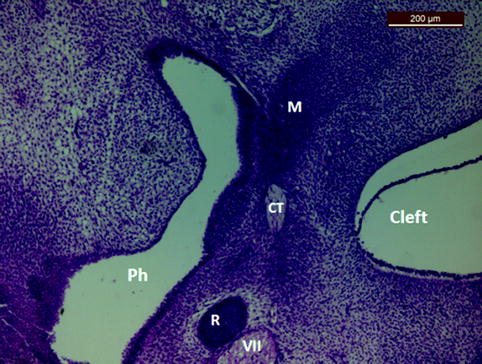
Fig. 6.4
A 15.5-mm human embryo, transverse section. Facial nerve is visible in close relationship with the Reichert’s cartilage (R). Chorda tympani (CT) is more anterior, between first and second arches, in relationship with the malleus (M). Ph first pharyngeal pouch, cleft first branchial cleft. Hematoxylin-eosin staining
Originally, the facial nerve passes in a sulcus in the cartilaginous otic capsule; later this sulcus ossifies and becomes the bony canal of the facial nerve. The process of ossification has two centers:
An anterior center: it develops at the apical cochlear ossification center by the end of the 20th week gestation.
A posterior center: it arises at the pyramidal eminence by the 25th week of gestation [3].
Each ossification center emits two bony projections that ideally encircle progressively the entire length of the facial nerve. At term, about 80 % of the tympanic segment of the Fallopian canal is ossified; the ossification is almost completed around 3 months after birth. Facial nerve dehiscence is related to failure of complete fusion of these two ossification centers [3].
Surgical Pearl
At birth, the facial nerve exits the stylomastoid foramen on the lateral aspect of the skull, just inferior to the tympanic membrane and external ear canal. This makes the facial nerve vulnerable to traumatic injury during difficult delivery. In the second year of life, the growing mastoid process pushes the stylomastoid foramen medially and covers the facial nerve exit. Before the age of 2 years, a retroauricular incision should not be extended inferiorly; otherwise the facial nerve could be injured at its exit from the stylomastoid foramen.
6.1.1 Facial Nerve Connections
At the 7th week, a ventral offshoot from the geniculate ganglion reaches the glossopharyngeal ganglion. This will form the lesser superficial petrosal nerve. At approximately the same time, the branch of the stapedial muscle appears [4].
Between the 12th and 13th week, two twigs from the dorsomedial surface of the facial nerve between the stapedial muscle and the chorda tympani nerve fuse together and reach the superior ganglia of the vagus (CN X) and glossopharyngeal (CN IX) nerves to give Arnold’s nerve or the auricular branch of the vagus nerve. The Arnold’s nerve traverses the primitive tympanomastoid fissure and innervates the subcutaneous tissue of the posterior aspect of the external auditory canal (Ramsay Hunt area) [4].
By the 17th week, the definitive communications of the facial nerve, including those with the second and third cervical nerves, the trigeminal nerve, the vagus nerve, and the glossopharyngeal nerve, are established.
Clinical Applications
Facial Nerve in Aural Atresia
Facial nerve abnormal trajectory is common in major aural ear atresia. This is due to the abnormal development of the tympanic bone, which normally pushes the mastoid segment of the facial nerve posteriorly. The facial nerve may be placed in the middle ear cavity, mostly between the oval and the round windows (Fig. 6.5 ) [ 5 ].
Fig. 6.4
(a) A transversal computed tomographic view of a right ear microtia and complete absence of the external auditory canal, atretic bony plate (white arrows). The mastoid segment of the facial nerve (thick black arrow) is displaced anteriorly, facing the round window (thin black arrow). M microtia. (b) Coronal view of an atretic ear showing the mastoid segment of the facial nerve (arrowheads) displaced anteriorly at the level of the vestibule (V)
6.2 Facial Nerve Anatomy
The facial nerve is the nerve of the second branchial arch. It contains motor and somatosensory components. The somatosensory component of the facial nerve is described under the name of the nervus intermedius, pars intermedia of Wrisberg.
The facial nerve is composed of approximately 10,000 neurons:
7,000 myelinated neurons: to form the motor part of the facial nerve that innervates the expressions muscles of the face and the stapedial muscle.
3,000 neurons: to form the nervus intermedius with secretory and somatosensory components. They include:
1.
The afferent taste fibers from the chorda tympani nerve, coming from the anterior two-thirds of the tongue
2.
The afferent taste fibers from the soft palate via the palatine and greater petrosal nerves
3.
The parasympathetic secretory innervations to the submandibular, sublingual, and lacrimal glands
4.
The cutaneous sensory component from afferent fibers originating from the skin of the auricle and postauricular area or Ramsay Hunt area [6]
The facial nerve exits the brainstem at the pontomedullary junction; it traverses the cerebellopontine angle (CPA) and enters the internal auditory canal (IAC). Then it traverses the temporal bone in a bony canal, the Fallopian canal, until it reaches the stylomastoid foramen where it exits the temporal bone and enters the parotid gland [7, 8].
6.2.1 The Cerebellopontine Angle (CPA) Segment
The facial nerve (CN VII) leaves the brainstem at the pontomedullary junction almost 1.5 mm anterior to the vestibulocochlear nerve (VIII) [9].
The facial nerve then follows a rostro-lateral course through the cerebellopontine cistern for a distance of 15–17 mm, to enter finally the porus of the internal auditory canal (IAC) in the temporal bone.
The CPA segment of the facial nerve is 1.8 mm in diameter and is smaller than the cochleovestibular nerve CN VIII which is of around 3 mm [9]. A third smaller nerve, the nervus intermedius, emerges between CN VII and CN VIII.
Clinical Application
The root exit zone of the facial nerve (REZ) corresponds to a junctional area between central and peripheral myelin. At this level the facial nerve is sensitive to compression from a vascular loop; vascular compression at the REZ of the facial nerve is the most acceptable underlying physiopathology of a hemifacial spasm [10–13].
6.2.2 The Internal Auditory Canal Segment (IAC)
The IAC segment of the facial nerve occupies the anterosuperior quadrant of the IAC and measures 8–10 mm; it lies superior to the cochlear nerve and it passes above the crista falciformis [14]. The nervus intermedius passes between the motor root of the facial nerve and the cochlear nerve.
A crest of bone, the “Bill’s bar” hangs in the vertical plane of the IAC between the superior vestibular nerve and the facial nerve, the later being anterior to the vestibular nerve (Fig. 6.6).
Fig. 6.6
Left ear translabyrinthine approach to the internal auditory canal after cut and reflection of both vestibular nerves (VN), showing the facial nerve (VII) lying superiorly and the cochlear nerve (C) inferiorly (the VII is anterior to the vestibular nerve). Bills bar (BB) is present in the meatus of the internal auditory canal and seperates the facial nerve from the superior vestibular nerve. TC tansverse crest (Courtesy of Tardivet [45])
At the bottom of the IAC, the fundus, the facial nerve enters the Fallopian canal. This transit zone between the IAC and the Fallopian canal is called the meatal segment and is the narrowest zone of bony facial canal; it is around 0.65 mm in diameter [14]. At this zone, the sheath of the nerve is formed only of pia mater and an arachnoid membrane because the dural investment terminates at the fundus of the IAC. This segment of the facial nerve is the most common site of entrapment during inflammatory disorders of the facial nerve, such as Bell’s palsy and Ramsay Hunt syndrome.
6.2.3 The Facial Canal (Fallopian Aqueduct)
The facial nerve enters in a bony canal called the Fallopian canal (after Gabriel Fallopius). It is 25–30 mm in length [7]. No other nerve in the body travels such a long distance through a bony canal.
Clinical Application
In case of an inflammatory swelling of the facial nerve, Bell’s palsy, for example, the bony shell around the nerve may lead to a facial nerve compression. A severe facial nerve compression for a long time may result in nerve ischemia with a resultant worse prognosis for facial paralysis recovery. Facial nerve decompression consists of opening the facial canal in the areas of facial nerve inflammation and swelling. The inflammatory segment could be identified by MRI imaging since it enhances strongly after gadolinium injection.
The Fallopian canal is divided into three distinct anatomic segments separated by two genus:
6.2.3.1 The Labyrinthine Segment (First Segment)
The labyrinthine segment of the facial nerve is 3–5 mm long; it is the shortest and the narrowest segment of the Fallopian canal. The narrowest part is at its entrance, the meatal segment. It lies beneath the middle cranial fossa and extends from the meatal foramen to the geniculate ganglion [15]. It travels anteriorly, superiorly, and laterally, forming an anteromedial angle of 120° with the IAC portion. It lies immediately above the anterior part of the vestibule.
The basal turn of the cochlea is anteroinferior to the labyrinthine segment and is in close relationship to the Fallopian canal.
When the nerve reaches a point just lateral and superior to the cochlea, it angles sharply forward, nearly at a right angles to the long axis of the petrous bone, to reach the geniculate ganglion (Fig. 6.7).
Fig. 6.7
Middle cranial fossa view of a right-side facial nerve after drilling the bone covering the labyrinth, the facial nerve, and the tegmen tympani. IAC internal auditory canal segment of the facial nerve, 1 labyrinthine segment, G geniculate ganglion, GSPN greater superficial petrosal nerve, 2 tympanic segment, Co cochlear area, M malleus, I incus, * cochleariform process LSCC lateral semicircular canal, PSCC posterior semicircular cana, SSCC superior semicircular canall. (Courtesy of Tardivet [45])
Before reaching the geniculate ganglion, both the facial nerve and the nervus intermedius remain distinct entities, and they meet each other just before joining the geniculate ganglion.
6.2.3.2 Geniculate Ganglion
The geniculate ganglion is situated at the lateral end of the labyrinthine segment. The pain fibers of the auricular branch and the taste fibers of the chorda tympani synapse with the second sensory neuron at the level of the geniculate ganglion; the secretomotor fibers to the lacrimal gland pass through the geniculate ganglion and form the greater petrosal superficial nerve.
At the level of the geniculate ganglion, the facial nerve takes an abrupt posterior direction, forming an acute angle 48–86° between the first and the second segment of the facial nerve; this is the “first genu” of the facial nerve [16] (Figs. 6.7 and 6.8). The geniculate ganglion is dehiscent in 15 % of temporal bones, a condition which makes the facial nerve vulnerable to injury during middle cranial fossa surgery.
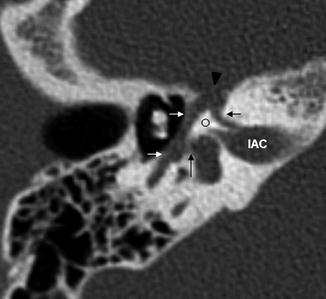
Fig. 6.8
Transversal computed tomographic view on a left ear. Labyrinthine segment (short black arrow), geniculate ganglion (black arrowhead), tympanic segment of the facial nerve (white arrows), oval window niche (long black arrow). Notice the acute angle between the first and second segment of the facial nerve (circle). IAC internal auditory canal
6.2.3.3 The Greater Superficial Petrosal Nerve
The greater superficial petrosal nerve (GPSN) is a secretomotor branch of the facial nerve. It emerges from the anterior upper portion of the ganglion; it carries secretory fibers to the lacrimal glands. This nerve exits the petrous temporal bone in an anterointernal direction through the hiatus of the facial canal to enter the middle cranial fossa (Figs. 6.7 and 6.11).
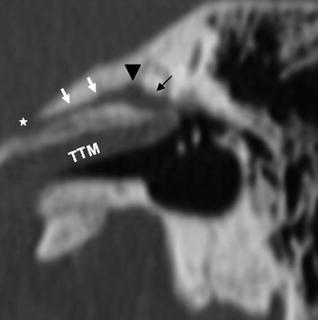
Fig. 6.11




Sagittal reconstruction of a computed tomography. Facial nerve (black arrow), leaving the geniculate ganglion (black arrowhead) posteriorly. Greater superior petrosal nerve (white arrows) leaving the geniculate ganglion anteriorly. Hiatus of the facial canal (*), TTM tensor tympani muscle
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
