, Jacques Magnan3, Hassan Haidar4, Karen Nicolas5, 6 and Stéphane Louryan7
(1)
Hospital Sacre Coeur ORL Chirurgie Cervico – Faciale, Lebanese University, Baabda, Lebanon
(2)
ORL Chirurgie Cervico – Faciale, Hôpital Trad, Beirut, Lebanon
(3)
ORL – Chirurgie Cervico – Faciale, University Aix-Marseille Hôpital Nord, Marseille, France
(4)
ORL – Chirurgie Cervico – Faciale, Hôpital Nord, Marseille, France
(5)
Department of Radiology Middle East Institute of Health, Bsalim Levant Clinics, Fachaerztin fuer Radiologische Diagnostik Lebanese University, Beirut, Lebanon
(6)
Department of Radiology, Levant Clinics, Sinn el Fil, Lebanon
(7)
Laboratoire d` Anatomie Biomécanique et Organogenèse, Université Libre de Bruxelles Faculté de Médecine, Brussels, Belgium
4.1.1 The Saccus Anticus
4.1.2 The Saccus Medius
4.1.3 The Saccus Superior
4.1.4 The Saccus Posticus
4.2.1 Walls of the Protympanum
4.4.1 The Lateral Spaces
4.4.2 The Medial Spaces
4.6 The Mesotympanum
Abstract
The middle ear cavity is anatomically not only a sole chamber, but a space with different compartments. The objective of this chapter is to present a detailed and exhaustive description of these compartments, their frontiers, their relationship, and their connections to improve the understanding of the pathophysiology of the inflammatory and cholesteatomatous middle ear diseases.
The middle ear cavity was divided into five compartments: the mesotympanum in the center, the epitympanum superiorly, the protympanum anteriorly, the hypotympanum inferiorly, and the retrotympanum posteriorly.
The middle ear cavity is anatomically not only a sole chamber, but a space with different compartments. The objective of this chapter is to present a detailed and exhaustive description of these compartments, their frontiers, their relationship, and their connections to improve the understanding of the pathophysiology of the inflammatory and cholesteatomatous middle ear diseases.
The middle ear cavity was divided into five compartments: the mesotympanum in the center, the epitympanum superiorly, the protympanum anteriorly, the hypotympanum inferiorly, and the retrotympanum posteriorly (Fig. 4.1).
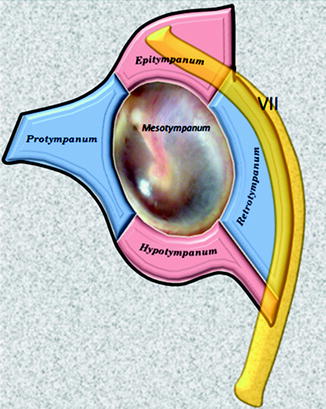
Fig. 4.1
Middle ear compartments; VII facial nerve
In addition, this chapter, based on the description of the anatomy of the middle ear folds in Chap. 3, will describe several anatomo-functional units inside or even beyond the traditional division of the compartments.
The comprehensive knowledge of this detailed anatomy is the key of success in the management of middle ear disorders.
4.1 Embryology of Middle Ear Compartments
In the developing human, the tympanomastoid system appears in the 3rd week of life from an outpouching of the first pharyngeal pouch called the tubotympanic recess. The endodermal tissue of the dorsal end of this pouch becomes the Eustachian tube and the tympanic cavity [1].
By the 7th week, a concomitant growth of the second branchial arch constricts the midportion of the tubotympanic recess, placing the primary tympanic cavity lateral to this constriction and the primordial Eustachian tube medial to this constriction [1]. The future development of the Eustachian tube is marked by lengthening, narrowing, and mesodermal chondrification establishing the fibrocartilaginous Eustachian tube (see Sect. 7.1).
The terminal end of the tubotympanic recess buds into four sacci: the saccus anticus, the saccus medius, the saccus superior, and the saccus posticus [1–3]. These sacci expand progressively to replace middle ear mesenchyme and mastoid mesenchyme (Fig. 4.2). The walls of the expanding sacci envelop the ossicular chain and line the walls of middle ear cavity; the interface between two sacci gives rise to several mesentery-like mucosal folds, transmitting blood vessels and ligaments to middle ear contents.
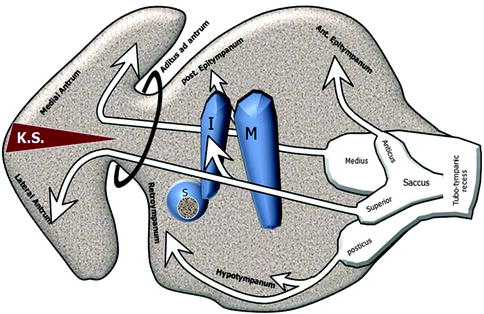
Fig. 4.2
Embryology of middle ear spaces. I incus, M malleus; S, stapes, KS Korner’s septum
4.1.1 The Saccus Anticus
The saccus anticus is the smallest saccus. It extends upward anterior to the tensor tympani tendon to form the anterior epitympanic recess and the anterior pouch of von Tröltsch. At the level of the tensor tympani muscle canal, it fuses with the anterior saccule of the saccus medius to form an important mucosal fold, the tensor tympani fold. The tensor tympani fold separates the anterior epitympanic recess superiorly from the supratubal recess inferiorly [2] (Figs. 4.2 and 4.3).
Fig. 4.3
Table illustrating the origin of the different spaces, recesses, and pouches of the middle ear
4.1.2 The Saccus Medius
The saccus medius forms the attic. It extends upward and divides into three saccules:
1.
Anterior saccule: It develops upward to form the anterior compartment of the attic.
2.
Medial saccule: The medial saccule forms the superior incudal space by its growth over the incudomalleal bodies and the posterior incudal ligament. The medial saccule sends an offshoot forward to form the Prussak’s space.
4.1.3 The Saccus Superior
The saccus superior forms the posterior pouch of von Tröltsch and the inferior incudal space. It extends posteriorly and laterally between the handle of the malleus and the long process of the incus to form the posterior pouch of von Tröltsch, the inferior incudal space, and the lateral part of the antrum which derives from the squamous part of the temporal bone.
The plane of fusion between the posterior saccule of the saccus medius, which forms the medial part of mastoid air cells system, and the saccus superior, which forms the lateral part of mastoid air cells system, usually breaks down. If the breakdown fails, a bony septum persists between the two parts, called the Korner’s septum [2] (Figs. 4.2 and 4.3).
4.1.4 The Saccus Posticus
The saccus posticus extends along the hypotympanum and rises up posteriorly to form the round window niche, the oval window niche, the facial recess, and the sinus tympani.
4.2 Anatomy of the Protympanum
The protympanum is the middle ear compartment that lies anterior to a frontal plane drawn through the anterior margin of the tympanic annulus (Fig. 4.1). This space is widely open posteriorly into the mesotympanum; it leads anteriorly into the Eustachian tube. We included into the protympanum the whole bony portion of the Eustachian tube which is 1 cm long in adults.
4.2.1 Walls of the Protympanum
The lateral wall of the protympanum consists of a thin plate of the tympanic bone called the lateral lamina; this plate separates the protympanum from the mandibular fossa. The medial wall consists of the cochlea posteriorly and the carotid canal anteriorly. The roof is composed of the bony semicanal for the tensor tympani muscle and the tensor tympani fold separating the protympanum from the anterior attic (Fig. 4.4).
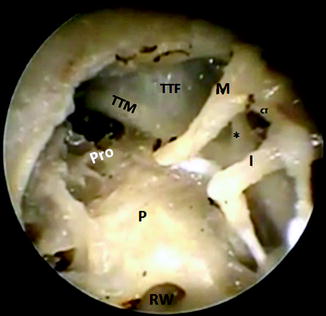
Fig. 4.4
Endoscopic view of a left cadaveric middle ear showing the protympanum (Pro) which is limited superiorly by the canal of the tensor tympani muscle (TTM) and the tensor tympani fold (TTF). (*) cochleariform process, M malleus, I incus, P promontory, RW round window, CT chorda tympani
4.2.2 The Supratubal Recess (STR)
The supratubal recess is the superior extension of the protympanum. It corresponds to the space lying between the superior border of the tympanic orifice of the Eustachian tube and the tensor tympani fold. It lies below the anterior attic from which it is separated by the tensor tympani fold (TTF).
The size of the supratubal recess depends on the anatomy of the TTF (see Sect. 3.6.2.10). The TTF forms the roof of the protympanum and has variable orientations depending on the level of its anterior insertion. For instance, a horizontal TTF results in a small or even absent supratubal recess and a vertical TTF gives place to a large supratubal recess [4–6] (see Fig. 3.38).
4.3 Anatomy of the Hypotympanum
The hypotympanum is a crescent-shaped space located at the bottom of the middle ear. It lies below a horizontal plane starting from the inferior margin of the fibrous annulus to the inferior margin of cochlear promontory; it is surrounded by five walls.
4.3.1 Walls of the Hypotympanum
The anterior wall is formed by the carotid canal medially and by a dense bone laterally.
The posterior wall is formed by the inferior part of the styloid complex and the vertical segment of the facial nerve canal. Frequently, the posterior wall is pneumatized by air cells (retrofacial air cells) which extend from the mastoid antrum to the hypotympanum medial to the facial nerve. The posterior wall corresponds to a vertical plane from the posterior semicircular canal to the junction of the sigmoid sinus with the jugular bulb.
The outer wall is formed by the tympanic bone.
The medial wall is formed by the lower part of the promontory and a part of the petrous bone which extends under the promontory. This wall is usually pneumatized; its air cell system may extend beneath the cochlea to reach the petrous apex air cells. Rarely the medial wall is compact (Fig. 4.5).
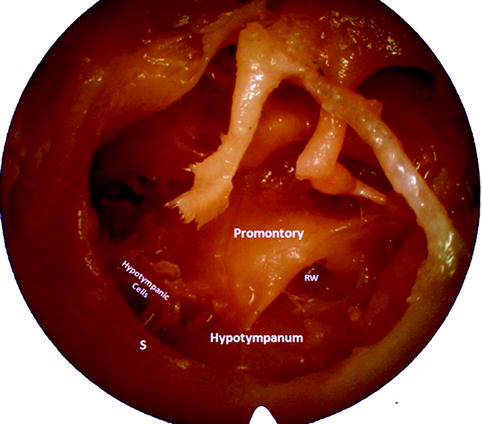
Fig. 4.5
Endoscopic view of a left ear showing the hypotympanum and some hypotympanic cells. Notice that the hypotympanum lies below the level of the tympanic sulcus (S). In this case, the inferior wall of the hypotympanum is smooth and consists of a thin plate of bone separating the middle ear from the jugular bulb. RW round window
The inferior wall corresponds to a thin bony plate separating the hypotympanum from the jugular bulb (Fig. 4.5). In cases of a high jugular bulb, the hypotympanum is significantly reduced, or it could even be missing.
4.3.2 Air Cells in the Hypotympanum
The air cells of the hypotympanum are divided into:
4.3.2.1 Hypotympanic Air Cells
The hypotympanic air cells, present in the medial and inferior wall of the hypotympanum, may extend below the labyrinth to reach the petrous apex cells (infralabyrinthine tract) (Fig. 4.6 and see Fig. 2.12b).
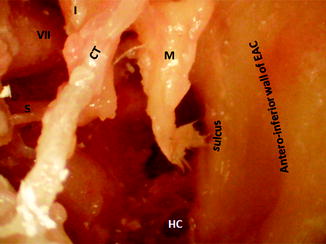
Fig. 4.6
Endoscopic view of a right ear showing hypotympanic cells in the inferior and medial wall of the hypotympanum. M malleus, I incus, S stapes, CT chorda tympani, VII tympanic segment of the facial nerve
Surgical Applications
Infracochlear Approach
4.3.2.2 Retrofacial Cells
The retrofacial cells extend from the central mastoid tract medial to the facial nerve and drain into the hypotympanic space.
Surgical Application
Retrofacial Hypotympanotomy
Dissecting the retrofacial cells medial to the vertical segment of the facial nerve between the jugular bulb inferiorly and the posterior semicircular canal superiorly provides a good access to the hypotympanum and the related structures without transposing the facial nerve or taking down the posterior external auditory canal wall (retrofacial hypotympanotomy) [10]. A high-riding jugular bulb obstructs this approach (see Fig. 2.12) (see Sect. 2.2.2.2).
4.4 Anatomy of the Retrotympanum
The retrotympanum is a complex region. It consists of several separate spaces lying in the posterior aspect of the tympanic cavity medial and posterior to the tympanic annulus (Fig. 4.1). The retrotympanum is the site of the highest incidence of middle ear pathologies especially retraction pockets and cholesteatoma (Fig. 4.7).
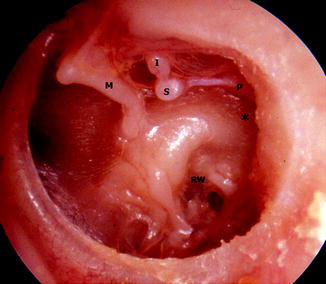
Fig. 4.7
Otoscopic view of a left ear showing adhesive otitis media and a posterior pars tensa retraction pocket into the retrotympanum (*). I incus with lysis of its long process, M malleus, S stapes, Ppyramidal eminence, RW round window
The retrotympanum includes four spaces: two spaces lie medial to the vertical segment of the facial nerve and the pyramidal eminence and two spaces lie lateral to them. These spaces are separated from each other by the bridges and the eminences of the posterior wall of the middle ear cavity. The pyramidal eminence is the fulcrum of the retrotympanum (Fig. 4.8) (see Sect. 2.3.2).
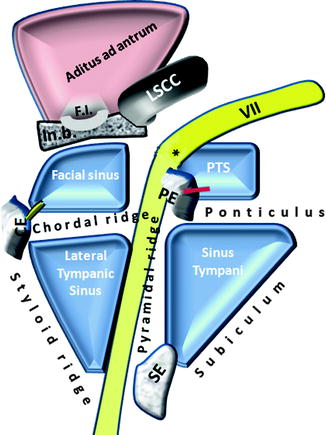
Fig. 4.8
Schematic drawing of the retrotympanum as viewed from the mesotympanum. PE pyramidal eminence, CE chordal eminence, SE styloid eminence, VII tympanic segment of facial nerve, * second genu of facial nerve, FI fossa incudis. In.b. incudal buttress, PTS posterior tympanic sinus, LSCC lateral semicircular canal
4.4.1 The Lateral Spaces
The lateral spaces of the retrotympanum form the facial recess. The facial recess is bordered medially by the facial canal and the pyramidal eminence and laterally by the chorda tympani. Superiorly, the facial recess is bounded by the incudal buttress, bony boundary of the incudal fossa, which lodges the short process of the incus. The incudal buttress separates the facial recess from the aditus ad antrum. Inferiorly, the facial recess is limited by the chordo-facial angle which ranges from 18° to 30°; the distance between the origin of the chorda tympani and the short process of the incus ranges from 5 to 10 mm [11].
The facial recess size is variable among individuals; however, it does not differ between age groups ranging from newborns to adults, indicating that it is near adult size at birth [12–14]. It measures about 2 mm at the level of the round window and 3 mm at the level of the oval window [15, 16].
The chordal ridge, which runs between the pyramidal eminence and the chordal eminence, divides the facial recess into the facial sinus superiorly and the lateral tympanic sinus inferiorly.
4.4.1.1 The Facial Sinus
The facial sinus is the superior part of the facial recess. It is a small pouch that is situated between the incudal buttress superiorly, the chordal ridge inferiorly, and the second genu of the facial nerve medially. There is no connection of the facial sinus with the air cells of the attic or mastoid process.
4.4.1.2 The Lateral Tympanic Sinus
The lateral tympanic sinus is the inferior part of the facial recess and is the most lateral and narrowest sinus of the retrotympanum. It represents the interval among the three eminences of the styloid complex (pyramidal eminence, styloid eminence, chordal eminence). It lies medial to the chordal eminence, inferior and lateral to the pyramidal eminence, and superior to the styloid eminence. The dimensions of the lateral tympanic sinus vary from 1.5 to 2.5 mm [17, 18]; it has no connection with the attic or the antrum.
Surgical Application
The facial recess serves as a posterior window to reach the middle ear from the mastoid cavity, enabling the visualization of the oval window and ponticulus superiorly and the round window and subiculum inferiorly. This important surgical approach is called transmastoid posterior tympanotomy; it is done by a transmastoid drilling of the posterior wall of the facial recess, between the chorda tympani laterally and the facial nerve medially (Fig. 4.9).
Fig. 4.9
Left ear, transmastoid posterior tympanotomy (*). b incudal buttress, LSSC lateral semicircular canal
In cases of narrow facial recess or incomplete exposure of the target middle ear structure, extended facial recess approach could be done. In this technique, the chorda tympani nerve is sacrified and drilling is done between the annulus of the tympanic membrane and the facial nerve. This leads to a wider exposure of the middle ear. The mean width of the extended facial recess is about 5 mm [19, 20].
During posterior tympanotomy, the risk of facial nerve damage and the probability of sacrifying the chorda tympani depend on the dimensions of the facial recess [11, 18, 21, 22], which varies widely in the general population. However, preoperative thin-section CT scans allow surgeons to make a precise assessment of these anatomic structures during preoperative planning (Fig. 4.10).
Fig. 4.10
(a) A transversal computed tomography showing the distance (red line) between the chorda tympani (long white arrow) and the mastoid segment of the facial nerve (VII); the arrowhead shows the annulus. (b) Sagittal reconstruction of a computed tomography showing the emergence of the chorda (black arrow) from the facial nerve (VII) and the bony wall (circle) between the chorda and the VII (facial recess approach). White arrow facial recess, white arrowhead short process of the incus, LSCC lateral semicircular canal, PSCC posterior semicircular canal
4.4.2 The Medial Spaces
The medial spaces of the retrotympanum, called the tympanic sinus, are the depressions in the posterior wall of the middle ear that lie between the facial nerve and pyramidal eminence laterally and the labyrinth medially (Figs. 4.8 and 4.11).
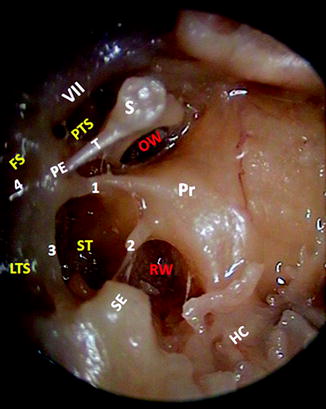
Fig. 4.11
Endoscopic view of a right middle ear showing the different sinuses and recesses of the retrotympanum. PTS posterior tympanic sinus, ST sinus tympani, LTS lateral tympanic sinus, FS facial sinus, PE pyramidal eminence, SE styloid eminence, 1 ponticulus, 2 subiculum, 3 pyramidal ridge, 4 chordal ridge, OW oval window, RW round window, S stapes, T stapedial tendon, Pr promontory, HC hypotympanic cells, VII facial nerve
The ponticulus, which runs from the promontory to the pyramidal eminence, divides the tympanic sinus in two spaces: the posterior tympanic sinus superiorly and the sinus tympani inferiorly.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


