, Jacques Magnan3, Hassan Haidar4, Karen Nicolas5, 6 and Stéphane Louryan7
(1)
Hospital Sacre Coeur ORL Chirurgie Cervico – Faciale, Lebanese University, Baabda, Lebanon
(2)
ORL Chirurgie Cervico – Faciale, Hôpital Trad, Beirut, Lebanon
(3)
ORL – Chirurgie Cervico – Faciale, University Aix-Marseille Hôpital Nord, Marseille, France
(4)
ORL – Chirurgie Cervico – Faciale, Hôpital Nord, Marseille, France
(5)
Department of Radiology Middle East Institute of Health, Bsalim Levant Clinics, Fachaerztin fuer Radiologische Diagnostik Lebanese University, Beirut, Lebanon
(6)
Department of Radiology, Levant Clinics, Sinn el Fil, Lebanon
(7)
Laboratoire d` Anatomie Biomécanique et Organogenèse, Université Libre de Bruxelles Faculté de Médecine, Brussels, Belgium
Abstract
The term “mastoid” is derived from the Greek word mastós, meaning “breast,” in reference to the shape of this bone. The mastoid process projects from the base of the skull and is situated behind the external auditory meatus at the inferior part of the outer surface of the temporal bone.
The mastoid process houses several important structures such as the facial nerve, the sigmoid sinus, and the labyrinth; it neighbors the middle and the posterior cranial fossa. Therefore, a good knowledge of the mastoid process anatomy is essential to approach it surgically and to avoid pitfalls.
Furthermore, the mastoid process is the site of numerous air-filled cavities known as mastoid air cells which play an important role in middle ear aeration.
The term “mastoid” is derived from the Greek word mastós, meaning breast, in reference to the shape of this bone. The mastoid process projects from the base of the skull and is situated behind the external auditory meatus at the inferior part of the outer surface of the temporal bone.
The mastoid process houses several important structures such as the facial nerve, the sigmoid sinus, and the labyrinth; it neighbors the middle and the posterior cranial fossa. Therefore, a good knowledge of the mastoid process anatomy is essential to approach it surgically and to avoid pitfalls.
Furthermore, the mastoid process is the site of numerous air-filled cavities known as mastoid air cells which play an important role in middle ear aeration.
5.1 Embryology of the Mastoid
The mastoid process appears at the 29th week of gestation as a result of the fusion of the periosteal layers of the otic capsule and the tympanic process of the squamous bone (see Figs. 1.1 and 1.3).
At birth, the mastoid process is underdeveloped; it becomes prominent by the age of 2 years and continues to grow until the age of 6 years. The expansion of the mastoid process is an active phenomenon and is secondary to the pneumatization process taking place inside it.
The pneumatization is a process in which the mastoid process, initially containing bone marrow, is invaded by the expanding air filled sacci. Thereafter, the mastoid becomes the site of an air-containing cavity called the mastoid air cells. The residual dense bone which did not pneumatize forms the septations between the mastoid air cells [1–12].
5.1.1 Embryology of the Mastoid Antrum
The antrum, which is the biggest of all mastoid air cells, starts its development between the 22nd and the 24th week of fetal life. It reaches its adult size on the 35th week [1, 13, 14].
The antrum develops at the center of the mastoid process on both sides of the petrosquamous fissure. The medial part of the antrum, the petrous part, develops from the saccus medius and the lateral part, the squamous part, develops from the saccus superior (Figs. 4.2 and 4.3) (see Chap. 4). The fusion plane between the petrous part and the squamous part gives the petrosquamous fissure. Failure of complete fusion between the two sacci leads to a septation of the mastoid antrum by a bony partition called the Korner’s septum [15] (Fig. 5.1).
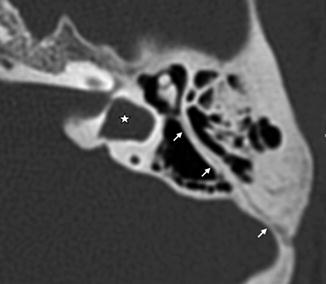
Fig. 5.1
Transversal computed tomography view of a left ear. Thin hyperlucent line (white arrows) along the fusion zone between the squamous and petrosal part of the mastoid, resulting in a bilamellar Korner’s septum. Developmental arrest of the vestibule (*)
The antrum is well developed at birth and has a mean surface of 1 cm2 [16]. The size of the antrum does not change after birth; however, it undergoes medial displacement because of the growth of the mastoid process. The mastoid process continues to grow until puberty and even beyond.
5.1.2 Postnatal Mastoid Pneumatization
At birth, the mastoid process contains only the antrum. After birth, mastoid air cells develop as an outgrowth of the antrum; epithelial air tracts bud from the antrum and extend to the adjacent areas of the temporal bone to form the mastoid air cells (Fig. 5.2). This extension is facilitated by the differentiation of bone marrow into loose mesenchyme. This process is called mastoid pneumatization.
Fig. 5.2
Transversal computed tomography of right ears: (a) in a newborn, showing the antrum (*) as the only air cell at this age; (b) in a child of 2 years old, showing advanced mastoid pneumatization medial and inferior to the antrum (arrows)
5.1.2.1 The Tracts of Pneumatization
Mastoid pneumatization proceeds through several well-established tracts. These tracts of pneumatization vary considerably. The main tracts of pneumatization are the following:
5.1.2.1.1 The Posterosuperior Cell Tract
The posterosuperior tract extends medially from the antrum at the junction of the posterior and middle fossa dural plates and above the superior semicircular canal and the internal auditory canal. It pneumatizes the medial pyramid of the temporal bone.
5.1.2.1.2 The Posteromedial Cell Tract (Superior Retrolabyrinthine)
The posteromedial tract extends medially through the antrum, parallel and inferior to the posterosuperior tract, to pneumatize the medial pyramid.
5.1.2.1.3 The Subarcuate Cell Tract (Translabyrinthine)
The subarcuate tract is situated more medially. It arises from the mastoid antrum and extends anteromedially passing below the superior semicircular canal; it pneumatizes the petrous apex.
5.1.2.1.4 The Perilabyrinthine Cell Tract
The perilabyrinthine cell tract arises from the antrum and pneumatizes the labyrinthine area. It is divided into the supralabyrinthine and the infralabyrinthine tracts. It can extend to the petrous apex.
5.1.2.1.5 The Peritubal Tract
This tract arises from the mastoid antrum and pneumatizes the tubal and peritubal area passing inferior to the labyrinth.
5.1.2.2 Mastoid Pneumatization Phases
The pneumatization of the mastoid begins at the 33rd week of gestation and ceases around puberty [1, 2, 17]. The last air cells to develop are the cells of the petrous apex. These air cells are present in about 35–40 % of adult temporal bones [2, 18, 19].
From birth until puberty, three phases of mastoid pneumatization are distinguishable:
Phase I (0–1 year): The antrum is of adult size at birth and has a mean surface of 1 cm2 (Fig. 5.2). During the first year of life, there is a rapid development of mastoid air cells. These new mastoid air cells add 3 cm2 to the whole surface of mastoid air cell system, resulting in a total surface of 4 cm2 at the age of 1 year.
In the same time the mastoid process increases 1 cm in length and width and 0.5 cm in depth.
Phase II (1–6 years): during this phase, mastoid pneumatization follows a linear pattern adding about 1 cm2 per year. At the age of 2 years, the mastoid tip covers the emergence of the facial nerve at the stylomastoid foramen. The mastoid process growth increases then by about 0.5 cm per year in length and width and 0.25 cm per year in depth (Fig. 5.2).
Postnatal mastoid pneumatization displays considerable variation and this is related to several factors including heredity, environment, infections, and Eustachian tube function. A controversy exists concerning the relationship between the degree of mastoid pneumatization and the development of middle ear diseases. There are two theories:
1.
Clinical Implications
The mastoid process is underdeveloped at birth. This situation leaves the facial nerve relatively superficial and unprotected where it emerges from the stylomastoid foramen. During difficult delivery, the use of forceps may damage the facial nerve by compression at this level. At the age of 2 years, as the air cells develop, the lateral part of the mastoid process grows downwards and forward to form the mastoid tip, which covers the stylomastoid foramen and offers progressively a better protection to the emerging facial nerve.
5.2 Mastoid Process Anatomy
The adult mastoid process is cone shaped and is slightly oblique forward and downwards. Its anterior border is rounded and vertical. Its posterior border is inclined about 45° downwards and forward. Behind the superior part of the mastoid process, the mastoid foramen is situated where the mastoid emissary vein passes.
The squamous bone forms the anterosuperior portion of the mastoid process. The petrous bone forms its postero-inferior part. The junction of the two parts forms the petrosquamous suture. The petrosquamous suture runs vertically from the superior border of the mastoid process to join its antero-inferior border just above the mastoid tip (Fig. 5.3).
Fig. 5.3
Lateral surface of a left temporal bone, showing the mastoid process (black dotted line) formed from a squamous part and a petrous part, joined by the petrosquamous suture (white dotted line). The mastoid process is attached to the tympanic bone by the tympanomastoid suture (TMS); * digastric notch
The mastoid process serves as a point of attachment for several muscles like the splenius capitis, the longissimus capitis, the digastric, and the sternocleidomastoid muscles. The mastoid process is larger in men because they require larger points of attachment for their bigger muscles. The sternocleidomastoid muscle inserts to the outer surface of the mastoid tip. The posterior belly of digastric muscle inserts on the digastric groove situated on the inner surface of the mastoid tip. The digastric groove is an infallible guide to point the facial nerve emergence from the stylomastoid foramen at the anterior end of the groove.
5.2.1 Surface Landmarks of the Mastoid Process
Along the lateral surface of the mastoid process, we distinguish several important surgical landmarks:
5.2.1.1 Temporal Line
The temporal line is a horizontal ridge situated at the upper limit of the mastoid process. It extends behind the posterior root of the zygomatic process and marks the inferior margins of the insertion of the temporal muscle (Fig. 5.3). The temporal line may be a prominent sharp edge or a broad prominence. It may be absent [23].
Surgical Pearl
It is widely accepted that the temporal line is indicative of the inferior level of the middle fossa dura. Hence, during mastoidectomy, it is always recommended to drill along, not above, the temporal line in order to avoid inadvertent injury to the dura [24].
Cadaveric studies found that the temporal line is located about 5 mm inferior to the middle fossa dura [25]. This may suggest that the drilling could start even at 5 mm above the temporal line without danger to the dura in order to increase the surgical exposure of the mastoid antrum.
5.2.1.2 Henle’s Spine
Henle’s spine is a prominent bony plate seen on the outer surface of the mastoid process. It is situated behind and above the posterosuperior quadrant of the external auditory meatus and below the origin of the temporal line [26]. This lamella is incurved nearly concentrically to the circumference of the meatus and its upper extremity is more anterior than its inferior one (Fig. 5.4). Henle’s spine could be small and smooth or sharp and long. It is absent in about 6 % of temporal bones [27, 28]. It serves as a point of attachment to the ligaments fixing the cartilaginous parts of the external acoustic meatus.
Fig. 5.4
Left cadaveric mastoid surface showing Henle’s spine and Mac-Ewen’s triangle. EAC external auditory canal
Surgical Pearl
Henle’s spine is an excellent landmark during mastoidectomy because it indicates the region of the deeply located aditus ad antrum. In addition it may serve as a landmark for middle fossa dura when the temporal line is absent; the dura is situated about 1 cm superior to Henle’s spine [25].
5.2.1.3 Mac-Ewen’s Triangle
The suprameatal triangle or “Mac-Ewen’s triangle” is a depression on the lateral surface of the mastoid process. It is located just between the anterior end of the temporal line, Henle’s spine, and the posterosuperior quadrant of the external acoustic meatus (Fig. 5.4).
5.2.2 Surgical Anatomy of the Mastoid Antrum
The mastoid antrum is the biggest mastoid air cell. It is of 10 × 10 mm in dimensions. It is located posterior to the external auditory canal and middle ear, inferior to the middle fossa dural plate, and anterior to the sigmoid sinus and the posterior fossa dural plate. The mastoid antrum communicates anteriorly with the attic through the aditus ad antrum (Figs. 5.5 and 5.6).
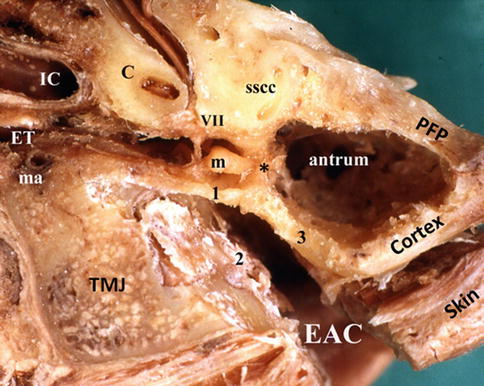
Fig. 5.5




Transverse cut of a left cadaveric temporal bone showing the antrum at the level of the aditus ad antrum (*). PFP posterior fossa plat, EAC external auditory canal, 1 attic outer wall, 2 anterior wall of the EAC, 3 posterior wall of the EAC, C cochlea, sscc superior semicircular canal, m malleus, VII facial nerve, IC internal carotid artery, ET Eustachian tube, ma middle meningeal artery, TMJ temporomandibular joint
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
