, Jacques Magnan3, Hassan Haidar4, Karen Nicolas5, 6 and Stéphane Louryan7
(1)
Hospital Sacre Coeur ORL Chirurgie Cervico – Faciale, Lebanese University, Baabda, Lebanon
(2)
ORL Chirurgie Cervico – Faciale, Hôpital Trad, Beirut, Lebanon
(3)
ORL – Chirurgie Cervico – Faciale, University Aix-Marseille Hôpital Nord, Marseille, France
(4)
ORL – Chirurgie Cervico – Faciale, Hôpital Nord, Marseille, France
(5)
Department of Radiology Middle East Institute of Health, Bsalim Levant Clinics, Fachaerztin fuer Radiologische Diagnostik Lebanese University, Beirut, Lebanon
(6)
Department of Radiology, Levant Clinics, Sinn el Fil, Lebanon
(7)
Laboratoire d` Anatomie Biomécanique et Organogenèse, Université Libre de Bruxelles Faculté de Médecine, Brussels, Belgium
7.1.1 Postnatal Growth (Fig. )
7.2.2 The Junctional Segment
7.2.4 The Pharyngeal End
7.2.6 Eustachian Tube Mucosa
7.2.8 Eustachian Tube Nerves
Abstract
The Eustachian tube (ET) or auditory tube is a slender tube that connects the middle ear cavity with the nasopharynx and serves to equalize air pressure on either side of the eardrum.
It is a hollow structure of bone and cartilage, lined with mucous membrane, and equipped by a muscular opening mechanism.
It is part of a system of contiguous organs, including the nose, the middle ear, and the mastoid air cells. This system is devoted to the middle ear ventilation, its protection, and its clearance. The impairment of this system leads to a middle ear dysventilation, which is the primary cause of the establishment of chronic otitis media.
The Eustachian tube (ET) or auditory tube is a slender tube that connects the middle ear cavity with the nasopharynx and serves to equalize air pressure on either side of the eardrum.
It is a hollow structure of bone and cartilage, lined with a mucous membrane, and equipped by a muscular opening mechanism.
It is part of a system of contiguous organs, including the nose, the middle ear, and the mastoid air cells. This system is devoted to middle ear ventilation, its protection, and its clearance. Impairment of this system leads to middle ear dysventilation, which is the primary cause of the development of chronic otitis media.
7.1 Eustachian Tube Development
The ET lumen develops from the persistence of the first pharyngeal pouch. Between the second and third week of gestation, the first pharyngeal pouch extends laterally between the first and the second branchial arches to make contact with the first branchial groove which is the origin of the external auditory meatus (Fig. 7.1). The distal part of this pouch expands to form the tubotympanic recess which is the primordium of the middle ear cavity. The proximal part becomes constricted to connect the future middle ear to the pharynx.
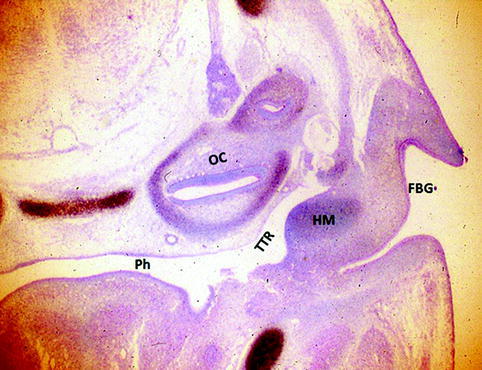
Fig. 7.1
The tubotympanic recess (TR) in a mouse embryo of gestation day 12. HM handle of malleus, Ph pharynx, OC otic capsule, TTR tubotympanic recess, FBG first branchial ectodermal groove. This horizontal section demonstrates the continuity between the pouch and the pharynx. Incorporation of radioactive sulfur with hematoxylin-eosin counterstaining
The structures associated with ET lumen develop from the mesenchyme surrounding the first pharyngeal pouch in a predictable sequence:
Before the 10th week of gestation, only the epithelial lining of the lumen has differentiated. Between the 10th and 12th week, the levator veli palatini (LVP) and tensor veli palatini muscles (TVP) develop and become delineated from the surrounding mesenchyme [1, 2] (Fig. 7.2).
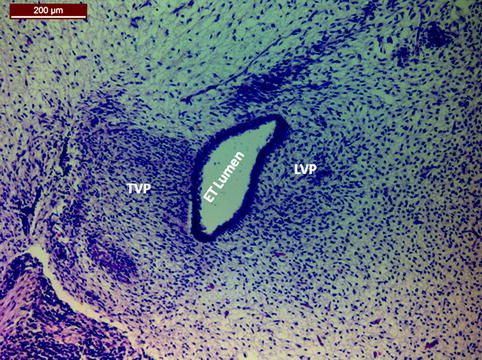
Fig. 7.2
Frontal section of the auditory tube rudiment in a 27-mm human embryo (end of the second month). TVP tensor veli palatine muscle anlage, LVP levator veli palatine muscle anlage. Hematoxylin-eosin staining
The initial differentiation of the cartilage begins at the 14th week. By the 20th week, the initial center of chondrification has increased in size and a perichondrium is clearly differentiated in the anteromedial portion of the tube [1, 2] (Fig. 7.3).
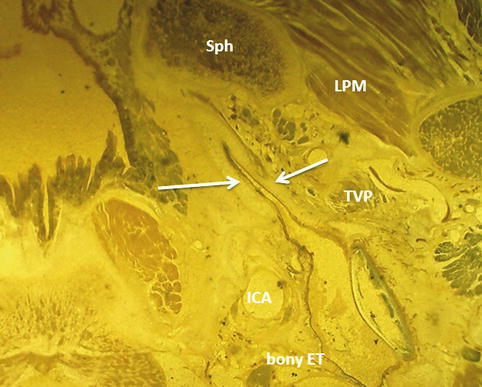
Fig. 7.3
A transverse cut of the base of skull in a 6-month fetus showing the Eustachian tube. Note the cartilaginous part is well developed (white arrows) and is in the same plane as the bony Eustachian tube (ET). LPM lateral pterygoid muscle, Sph sphenoid bone, ICA internal carotid artery, TVP tensor veli palatini muscle
These processes yield an ET structure very similar to that observed in an adult. Later during the rest of fetal life, morphometric changes occur among the ET structures. The most pronounced change is the increase in the length of the cartilaginous portion of the tube from 1 mm at the 10th week of gestation to 13 mm at birth.
While the fetus is growing, the tube deviates from the horizontal plane only about 10°, because the fetal cranial base is relatively flat; this situation persists until early childhood [1–4].
Clinical Application
An arrest of the development of the tubotympanic recess when the normal constriction of the tube is deficient may lead to a persistent wide open Eustachian tube all over its length. This is illustrated in this case of an adult female of 35 years old (Fig. 7.4). The developmental arrest concerns the whole left ear, associated to microtia, and external auditory canal atresia.
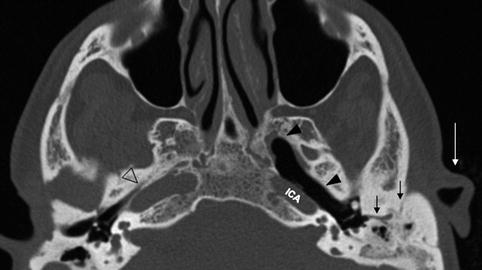
Fig. 7.4
Transversal computed tomographic view of both ears in a patient presenting left ear microtia (white arrow) and atresia of the external auditory canal (black arrows), also an abnormally large Eustachian tube (arrow heads) due to the arrest of constriction of the tubotympanic recess in contrast to the normal right side (empty arrow head). ICA internal carotid artery
7.1.1 Postnatal Growth (Fig. 7.5)
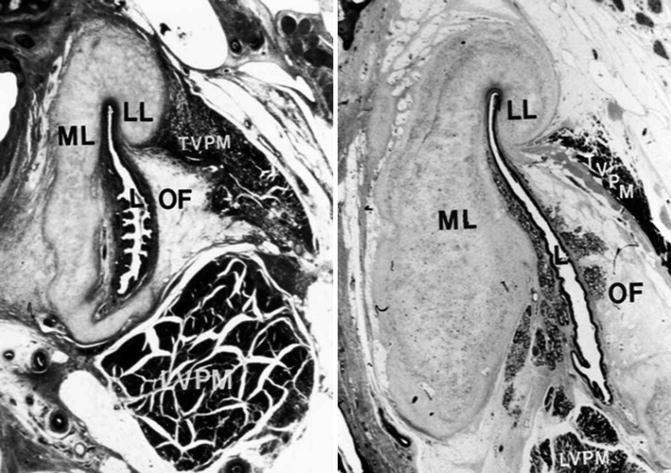
Fig. 7.5
Photomicrographs of cross sections through the midcartilaginous portion of the Eustachian tube (ET) of a 3-month-old female (left) and a 34-year-old male (right) showing the developmental difference of Ostmann’s fat pad (OF) and the size of the ET. L lumen, LL lateral lamina of the Eustachian tube cartilage, LVPM levator veli palatini muscle, ML medial lamina of the Eustachian tube cartilage, TVPM tensor veli palatini muscle (Courtesy of I. Sando, MD) (Reproduced with permission from Eustachian tube: structure, Function, Role in otitis media, by Charles D. Bluestone. pmph-usa.com)
The ET lengthens rapidly during early childhood: In infants, it is about half as long as that in adults; it is about 18 mm [5] and it reaches adult size by 7 years of age [6, 7].
The cartilaginous portion increases dramatically: The ratio of the length of the cartilaginous portion to the osseous portion is 8:1 in the infant, but this ratio becomes 4:1 in the adult due to the growth of the bony portion [8].
In infants, the cartilaginous and bony portions are aligned with a line that connects the pharynx and middle ear; however, due to the craniofacial growth, the cartilaginous tube is angled inferiorly from the osseous portion to form an angle of approximately 45° related to the horizontal plane [1, 9].
The LVP muscle increases in cross-sectional area and in volume and assumes a more suitable vector for an efficient active tubal dilatation.
The ET of the infant is floppy, very distensible, and lacks recoil phenomena of the hinge region. With time, the tubal cartilage stiffens and the elastin component develops in the hinge region; this will result in a reduced tubal compliance and an increased recoil, which raise the protective mechanism of the ET [10].
The lumen of the ET increases almost five times from the newborn to persons aged 20 years old; the cross-sectional length of the lumen increases significantly with age, especially in the pharyngeal area of the tube.
The lumen in most of the cartilaginous portion of the ET is significantly smaller in children than in adults [11].
Also the Ostmann’s fat pad increases in volume with age until adulthood, which may be related to better protective function in adults [12].
Surgical Implication
The majority of temporal bone with pneumatized petrous apex harbor peritubal air cells that may open directly into the ET lumen (Fig. 7.9). This explains the probability of cerebrospinal fluid rhinorrhea after translabyrinthine approach to the cerebellopontine angle when ET obliteration is not performed sufficiently far into the lumen by the end of the procedure [16].
7.2 Eustachian Tube Anatomy
The ET is a narrow osteocartilaginous channel connecting the tympanic cavity to the nasopharynx. Its lumen allows the passage of two different physical substances: one is gaseous for middle ear ventilation, and the second is fluid for the middle ear clearance. The ET begins at the tympanic orifice of the protympanum and ends at the pharyngeal orifice situated on the lateral wall of the nasopharynx. During its trajectory, the tube takes a slow curving inverted S course.
The general shape of the ET resembles to an hourglass made of two unequal cones. The first is small and fix, the posterior third, and represents the bony ET. The other one is elongated and mobile, the anterior two-thirds, and represents the fibrocartilaginous ET. Both parts are connected at the junctional zone, forming an angle of 160°.
In adults, the tubal axis forms with the plane of the hard palate an average angle of 36°(range 31–40°); the total length of the ET is 33 mm, divided as the following: the cartilaginous part is of 23.5 mm, the junctional part is of 3 mm, and the bony part is of 6.5 mm [13, 14] (Fig. 7.6).
Fig. 7.6
Schematic drawing of different Eustachian tube dimensions (average)
The bony portion is patent at all times; in contrary the fibrocartilaginous portion is closed at rest and opens intermittently.
7.2.1 The Bony Portion of the Eustachian Tube
The bony part of ET lies completely within the petrous part of the temporal bone. It runs from the tympanic orifice of the middle ear cavity in an anteromedial direction, following the petrous apex, towards the petrosphenoid sulcus on the inferior surface of the skull base.
The tympanic orifice of the Eustachian tube lies in the middle third of the anterior wall of the middle ear cavity, 4 mm above the floor of the middle ear and close to the carotid canal and the labyrinth (see Section 2.5.2). It is an oval structure that measures about 5 mm (horizontally) × 2 mm (vertically) [9] (Fig. 7.6).
Bony ET lumen is roughly triangular, measuring 2–3 mm vertically and 3–4 mm along the horizontal base [15].
The medial wall of the bony tube corresponds to the cochlea posteriorly and to the carotid canal anteriorly. The average thickness of the anteromedial portion of its bony wall is 1.5–3 mm. This bony wall is dehiscent in 2 % of individuals, exposing the carotid artery [15] (Fig. 7.7).
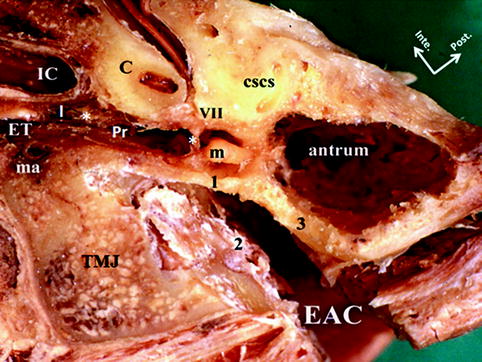
Fig. 7.7
Transverse cut of a left ear showing the bony Eustachian tube (Pr) housing the tensor tympani muscle (*), the cartilaginous Eustachian tube (ET), and the isthmus (I). Notice the relation of the Eustachian tube and the cochlea (C) and the petrous internal carotid artery (IC) medially and the temporomandibular joint (TMJ) and middle meningeal artery (ma) laterally. EAC external auditory canal, 1 attic outer wall, 2 anterior wall of EAC, 3 posterior wall of the EAC, m malleus, VII tympanic segment of facial nerve, CSCS superior semicircular canal
The upper third of the endoluminal surface of the medial wall presents the bony canal of the tensor tympani muscle. The lateral wall of the bony tube neighbors the canal of Hugier and the temporomandibular joint. The upper wall or roof of the bony tube corresponds to the tegmen tubari (Figs. 7.7 and 7.8).
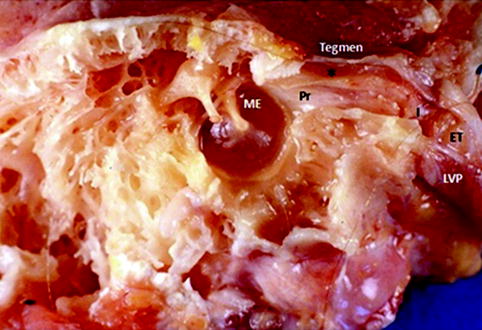
Fig. 7.8
Medial view of a sagittal cadaveric cut through a left middle ear (ME), showing the bony Eustachian tube (Pr) and the canal of tensor tympani muscle (asterisk), the isthmus (I), the cartilaginous Eustachian tube (ET), and its inferiorly related levator veli palatini muscle (LVP). The superior wall of the bony Eustachian tube is formed by the tegmen tubari
On the inferior surface of the base of skull, the end of the bony tube is constricted and it opens on the posterior part of the tubal sulcus; the bony tube end is situated between the carotid canal medially and the temporomandibular joint laterally.
Fig. 7.9




(a) Transversal computed tomographic view of a right ear. Eustachian tube (white arrow heads), surrounded by numerous aerated cells (white arrows); ICA internal carotid artery. (b) Computed tomograpic reconstruction perpendicular to the Eustachian tube (*) showing an air cell opened into the Eustachian tube (arrow); TTM (arrowhead)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
