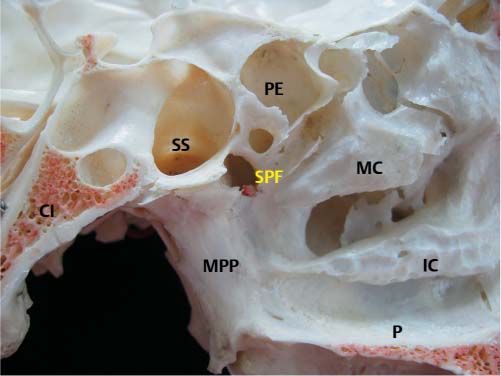
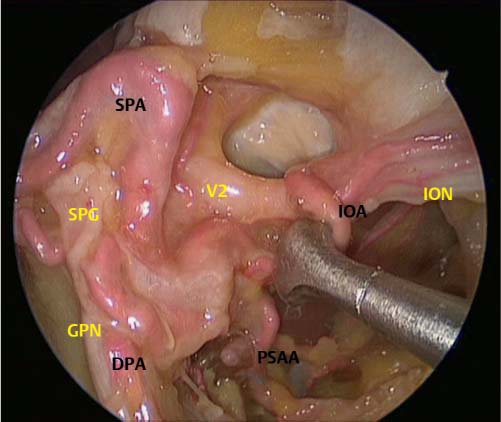
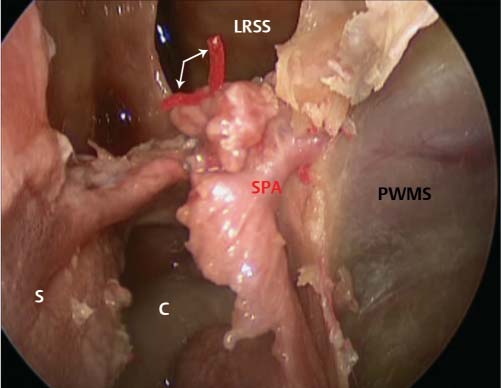
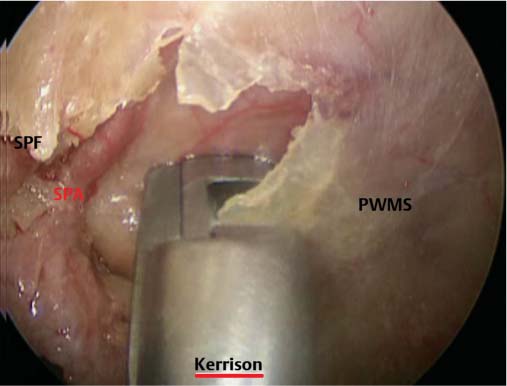
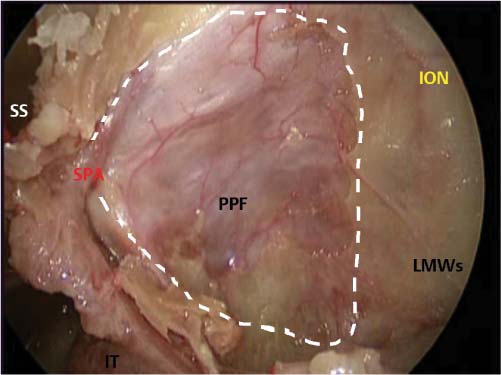
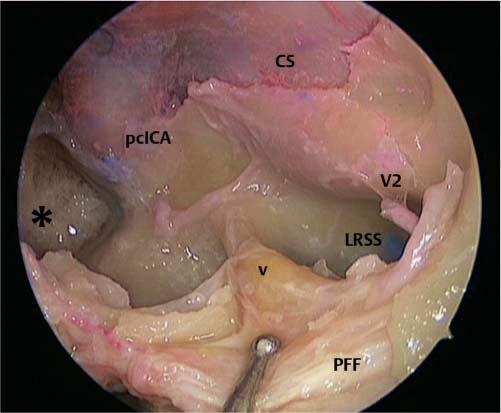
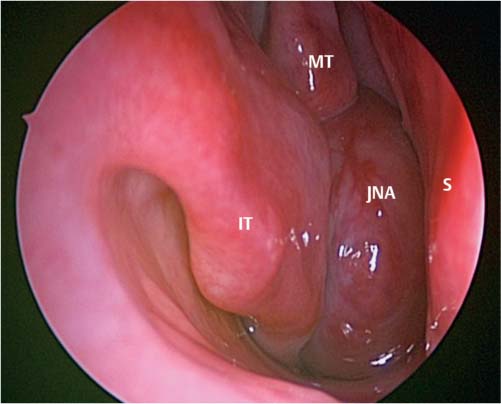
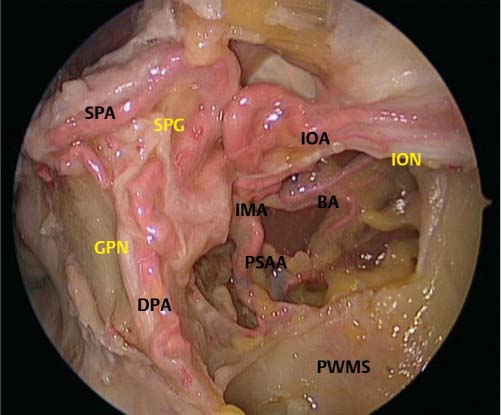
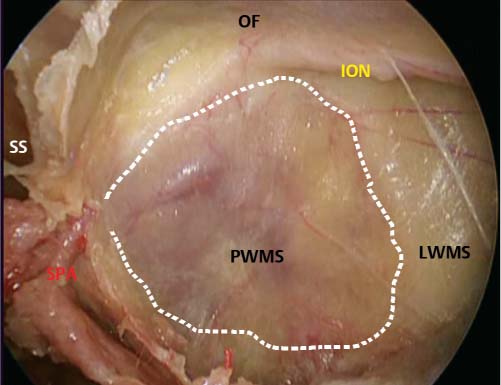
19 The Pterygopalatine Fossa The pterygopalatine fossa (PPF) is a pyramidal space with incomplete osseous boundaries located among the maxillary, sphenoid, and palatine bones (Fig. 19.1). The PPF is bounded posteriorly by the pterygoid plates of the sphenoid bone, which fuses at the skull base into the pterygoid process. Medially, the perpendicular plate of the palatine bone constitute the wall of the PPF, which tapers inferiorly in a funnel-shaped space at the level of the attachment between maxillary bone and the pyramidal process of the palatine bone (Fig. 19.2). The maxillary tuberosity constitutes the anterior boundary of the PPF, which communicates with the orbital apex through the medial portion of the inferior orbital fissure. Through the pterygomaxillary fissure, the PPF merges laterally with the masticatory space of the infratemporal fossa. The pterygopalatine fossa communicates with the middle cranial fossa, orbit, nasal cavity, oral cavity, and the infratemporal fossa via rotundum and sphenopalatine foramina, the vidian and palatovaginal canals, and the greater and lesser palatine foramina.1 Topographically, the PPF can be divided into an anterior and posterior compartment. The anterior space is occupied by the third segment of the maxillary artery (MA) and its branches, whereas the posterior compartment is represented by the maxillary nerve and the sphenopalatine ganglion and its branches.2 The pterygopalatine segment of the maxillary artery (third segment) runs on the anterior edge of the lateral pterygoid muscle and reaches the pterygopalatine fossa through the pterygomaxillary fissure (PMF). The MA passes horizontally deep to the mandibular ramus and gives off the buccal artery (BA), which supplies the buccinator muscle. It then turns medially through the PMF coursing in the anterior and superior direction to give off several branches. According to the order of branching in its course from the pterygomaxillary junction area, the posterosuperior alveolar artery (PSAA) and infraorbital artery (IOA) are located at the posterior wall of the maxilla and enter into the posterosuperior alveolar foramen and the infraorbital fissure, respectively (Fig. 19.3). Then, it divides into the descending palatine artery (DPA), which supplies the palate, the artery of the pterygoid canal (VA), which is located in the pterygoid canal, and the sphenopalatine artery (SPA).3 Fig. 19.1 Photomicrograph of a sagittal image of the bony medial boundaries of the left pterygopalatine fossa. SPF, sphenopalatine foramen; MPP, medial pterygoid plate; SS, sphenoid sinus; PE, posterior ethmoid cell; Cl, clivus; MC, middle concha; IC, inferior concha; P, hard palate. Fig. 19.2 Axial computed tomography (CT) scan showing the pterygopalatine fossa (white arrows). Fig. 19.3 Endoscopic view of the contents of the anterior compartment of the pterygomaxillary fossa. IMA, internal maxillary artery; BA, buccal artery; PSAA, posterior superior alveolar artery; SPA, sphenopalatine artery; IOA, infraorbital artery; DPA, descending palatine artery; SPG, sphenopalatine ganglion; GPN, greater palatine nerve; ION, infraorbital nerve; PWMS, posterior wall of maxillary sinus. Fig. 19.4 Endoscopic view of the contents of the posterior compartment of the pterygomaxillary fossa. V2, maxillary division of trigeminal nerve internal; PSAA, posterior superior alveolar artery; SPA, sphenopalatine artery; IOA, infraorbital artery; DPA, descending palatine artery; SPG, sphenopalatine ganglion; GPN, greater palatine nerve; ION, infraorbital nerve. Displacement of the vascular branches in the anterior compartment allows for visualization of the posterior compartment of the PPF (Fig. 19.4). The sphenopalatine ganglion (also known as the pterygopalatine ganglion) is naturally lodged into a niche of the posterior-inferior portion of the PPF just anterior to the pterygoid canal that conveys the vidian nerve. The maxillary nerve enters the PPF through the foramen rotundum and remains superolateral to the ganglion to give rise to its zygomatic branch while continuing to the infraorbital groove as the infraorbital nerve.4 During its anterolateral course, the infraorbital nerve constitutes an important surgical landmark that defines the PPF (medial) from the infratemporal fossa (lateral). Neural rami of distribution from the sphenopalatine ganglion are divisible into few groups: ascending (or orbital), posterior (to the pharynx), internal (to the nose), and descending (to the palate). Communicating rami connect the maxillary nerve to the inferiorly located sphenopalatine ganglion.5 These nerves, along with the presence of orbital rami, contribute to form the superior apex of the small ganglion conferring to it its characteristic macroscopic triangular-shaped appearance. The thin orbital rami carry parasympathetic neurons and erratically reach the nasal mucosa through the anterior or posterior ethmoidal canals. The sphenopalatine ganglion also receives sympathetic and parasympathetic fibers through the vidian nerve. This nerve, formed by the fusion of greater and deep petrosal nerves at the level of the lacerated foramen, enters the PPF through the pterygoid (vidian) canal along with the vidian branch of the maxillary artery. The greater and lesser palatine nerves (descending branches) arise from the inferior-posterior portion of the ganglion and through the palatine canals reach the oral cavity. The endoscopic endonasal route allows exposure of the pterygopalatine fossa through its anteromedial surface (see Video 19.1). The medial wall of the maxillary sinus is enlarged by extending the maxillary antrostomy to create a mega antrostomy or by performing a modified medial maxillectomy (Fig. 19.5). The posterior-lateral attachment of the middle turbinate is removed to gain access to the sphenopalatine foramen. The foramen is formed by the sphenopalatine notch inferiorly against the lower surface of the body of the sphenoid (Fig. 19.6). The notch itself is formed anteriorly by the orbital process of the palatine bone, inferiorly and posteriorly by the upper edge of the vertical plate of the palatine bone and the sphenoid process, respectively. A small bony ridge, the ethmoid crest, usually points to the sphenopalatine foramen, with the latter laying either completely or partially above the crest (class I and II, respectively). Occasionally, the sphenopalatine foramen consists of two separate openings, a larger superior opening and a small inferior one (class III). The orbital process of the palatine bone is removed and the sphenopalatine foramen is enlarged using a drill or a Kerrison rongeur (Fig. 19.7). The posterior wall of the maxillary sinus is then removed up to the vertical process of the palatine bone medially, and up to the angle between the lateral and posterior wall of the maxillary sinus to expose the pterygomaxillary fissure, which represents the communication between the pterygopalatine and the infratemporal fossa (Fig. 19.8). The pterygoid canal, the inferior part of the superior orbital fissure, the foramen rotundum, and the anterior surface of the pterygoid process can be identified and visualized. A wide sphenoid sinusotomy is then performed to determine the level of the sphenoid floor. The vidian foramen can be identified along the inferior bony face of the sphenoid sinus immediately posterior and perpendicular to the sphenopalatine foramen. The vidian nerve and artery can be identified in the pterygoid canal at the superior portion of the pterygopalatine fossa. Just medial to the vidian foramen, a small canal holding the pharyngeal or palatovaginal artery, which forms the sphenopalatine artery within the pterygomaxil lary fossa, can be visualized. The vidian nerve is an important landmark for the identification of the foramen lacerum and for the intrapetrous carotid artery. Safe surgical dissection can be performed by drilling on the inferior and medial surface of the vidian canal. The inferior 180 degrees of the vidian canal should be drilled prior to proceeding to the superior 180 degrees to avoid inadvertent injury to the vessel.1 Fig. 19.5 Endoscopic view of the posterior wall of maxillary sinus with window into the pterygomaxillary fossa (PPF). SPA, sphenopalatine artery; PWMS, posterior wall of maxillary sinus; LWMS, lateral wall of maxillary sinus; SS, sphenoid sinus; OF, orbital floor; ION, infraorbital nerve. Dashed white line window to PPF. Fig. 19.6 Endoscopic image showing a direct view of the sphenopalatine foramen with a wide sphenoidotomy showing septal branch of the sphenopalatine artery. SPA, sphenopalatine artery; PWMS, posterior wall of maxillary sinus; LRSS, lateral recess of sphenoid sinus; S, septum; C, choanae. White arrows indicate the posterior septal branches of sphenoid sinus. Fig. 19.7 Endoscopic resection of postwall of the left maxillary sinus with a Kerrison rongeur. SPA, sphenopalatine artery; SPF, sphenopalatine foramen; PWMS, posterior wall of maxillary sinus; Kerrison, Kerrison rongeur. Fig. 19.8 View of the left maxillary sinus after endoscopic resection of the posterior maxillary wall for a window into the pterygomaxillary fossa (PPF). SPA, sphenopalatine artery; PWMS, posterior wall of maxillary sinus; LWMS, lateral wall of maxillary sinus; SS, sphenoid sinus; ION, infraorbital nerve; IT, inferior turbinate. Dashed white line window to PPF. Through the foramen rotundum, the maxillary nerve travels from the cranial cavity into the pterygopalatine fossa. After piercing the foramen rotundum, this nerve passes through the pterygopalatine fossa and then reaches the inferior orbital fissure. The maxillary nerve is encountered during dissection within an area bounded superiorly by an oblique (or horizontal) line that connects the foramen rotundum and the infraorbital canal, inferiorly by a horizontal line at the level of the lower border of the sphenopalatine foramen, medially by a vertical line that passes through the foramen rotundum, and laterally by another vertical line at the posterior end of the infraorbital canal. In addition, the lower margin of the vidian canal can be used to depict the lowest level of the maxillary nerve more laterally. Before it becomes the infraorbital nerve, the maxillary nerve gives rise to the posterior alveolar nerve.6 The infraorbital nerve is a consistent landmark that delineates the surgical boundaries between the pterygopalatine and the infratemporal fossa. The pterygopalatine fossa is located medially to it, whereas the infratemporal fossa is located laterally to it. The identification of the vidian nerve and the maxillary nerve enable the surgeon to better define a surgical corridor between them that enables the exposure of the lateral wall of the sphenoid sinus (Fig. 19.9). The quadrangular area can have lesions arising in the pterygopalatine fossa, extending toward the middle cranial fossa and/or the cavernous sinus.7 This quadrangular-shaped surgical corridor is delineated anteriorly by the pterygoid bone from the foramen rotundum to the pterygoid canal, posteriorly by the intrapetrous segment of the intracavernous carotid artery, superiorly by the maxillary nerve and inferiorly by the vidian nerve. The lateral extension of the dissection using this approach can destabilize the pterygoid process, and consequently, problems with mastication ensue due to malfunction of the lateral pterygoid muscle and the medial pterygoid muscle.8 Tumors involving the pterygopalatine fossa can have multiple clinical presentations depending on the type and extent of tumor. Typical symptoms include unilateral nasal obstruction, epistaxis, V2 paresthesia, diplopia, and proptosis. Ocular symptoms with tumors involving the PPF can be secondary to affected pterygopalatine ganglion or cavernous sinus extension and subsequent abducens palsy. The differential diagnosis for lesions involving the PPF can be extensive including angiofibroma, carcinoma, lymphoma, melanoma, tumors of neural origin, and metastatic disease. It is important to note that imaging of tumors in the PPF usually identifies the extent of the tumor, but does not necessarily establish the diagnosis. Juvenile nasopharyngeal angiofibroma (JNA) is the most frequent benign neoplasm of the nasopharynx (Fig. 19.10). JNA originates at the sphenopalatine foramen and extends into the nasal cavity, nasopharynx, paranasal sinuses, pterygopalatine fossa, infratemporal space and the cranial base. The main blood supply to the tumor is the internal maxillary artery; however, the tumor may receive secondary blood supply from branches of the internal carotid artery, temporal and facial arteries. The most common clinical presentation of patients with JNA is nasal obstruction followed by epistaxis. Contrast-enhanced high-resolution computed tomography (CT) with axial and coronal reconstruction is the method of choice for evaluating the location and extent of the angiofibroma. Magnetic resonance imaging (MRI) is useful for evaluation of intracranial extension and recurrence cases. Preoperative embolization 24 to 48 hours prior to resection is recommended to reduce perioperative blood loss. The resection of JNA has to be tailored to the extent of the tumor and experience of the surgeon. The most common surgical approaches used are endonasal endoscopic, midface degloving, lateral rhinotomy, transpalatal, midfacial translocation, and infratemporal. Fig. 19.9 Angled endoscopic view of the lateral recess of the sphenoid sinus with the vidian nerve coursing posteriorly toward the foramen lacerum and the intrapetrous carotid artery. pcICA, paraclival internal carotid artery; CS, dura of cavernous sinus; V2, maxillary division of trigeminal nerve; v, vidian nerve; PPF, pterygopalatine fossa; LRSS, lateral recess of sphenoid sinus. * indicates the clivus. Fig. 19.10 Endoscopic view of a juvenile nasopharyngeal angiofibroma (JNA) in the right nasal cavity. IT, inferior turbinate; MT, middle turbinate; S, septum. Traditional approaches to the PPF via an anterior transmaxillary and transoral-transantral approaches have been associated with complications, such as facial edema, oroantral fistula, chronic maxillary sinusitis, vascular injury, injury of the infraorbital nerve, and dental injury. Therefore, lateral approaches especially for exposure and resection of malignant or invasive tumors have also been advocated. The endoscopic endonasal approach has been used for the surgical treatment of various neoplastic and inflammatory diseases of the PPF and its boundaries, as well as the lateral recess of the sphenoid sinus, which represents an extended pneumatization of the sphenoid bone just posterior to the PPF. In addition, this approach can be extended to reach the infratemporal fossa, cavernous sinus, middle cranial fossa, and nasopharynx. To perform a surgical access to or through the PPF a thorough knowledge and understanding of the intricate and complex neurovascular anatomy is necessary.9 This surgical anatomy is further complicated by anatomic variations and protected positions that may be difficult to access especially when bleeding or space-occupying lesions obscure them. The use of the endoscopic approaches together with intraoperative image-guided navigation systems has allowed for further broadening of the indications of the extended endoscopic endonasal approaches to the pterygopalatine fossa safely. • Tumors involving the pterygopalatine fossa can have multiple clinical presentations depending on the type and extent of the tumors. • PPF communicates with the orbital apex masticatory space, the infratemporal fossa, and the middle cranial fossa. • Topographically, the PPF can be divided into an anterior and posterior compartment. • The internal maxillary artery runs on the anterior edge of the lateral pterygoid muscle. • The sphenopalatine foramen is formed by the orbital process of the palatine bone, the vertical plate of the palatine bone, and the sphenoid process. • The vidian nerve can be identified at the superior portion of the pterygopalatine fossa. It is an important landmark for the identification of the foramen lacerum and for the intrapetrous carotid artery. • The most common clinical presentation of patients with JNA is nasal obstruction followed by epistaxis.

 Endoscopic Endonasal Surgery of the Pterygopalatine Fossa
Endoscopic Endonasal Surgery of the Pterygopalatine Fossa
 Tumors of the Pterygopalatine Fossa
Tumors of the Pterygopalatine Fossa
The Pterygopalatine Fossa
Pearls
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


