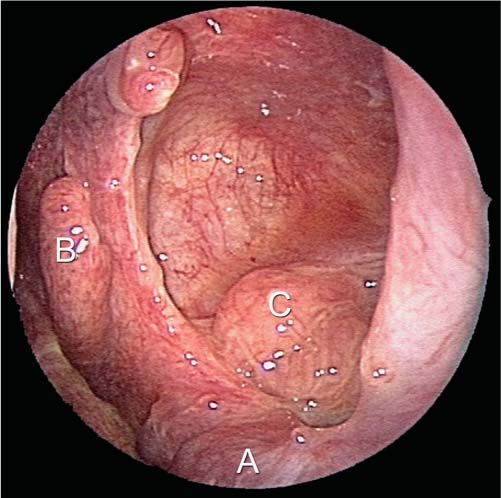
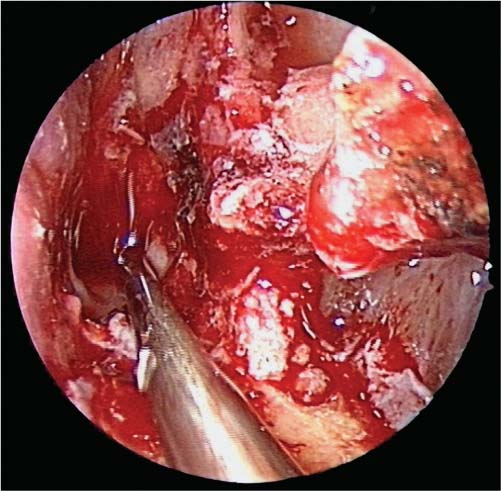
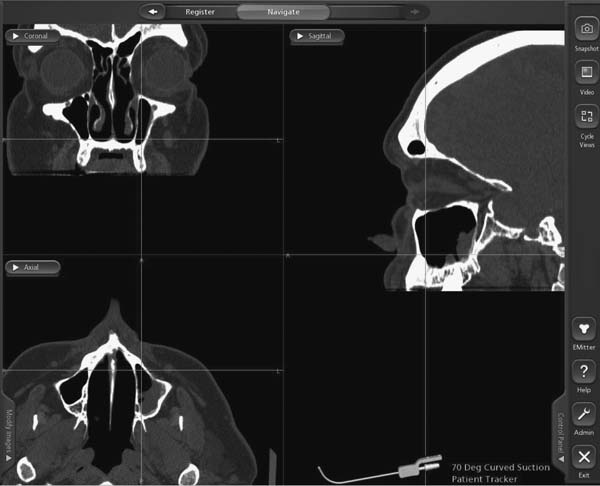
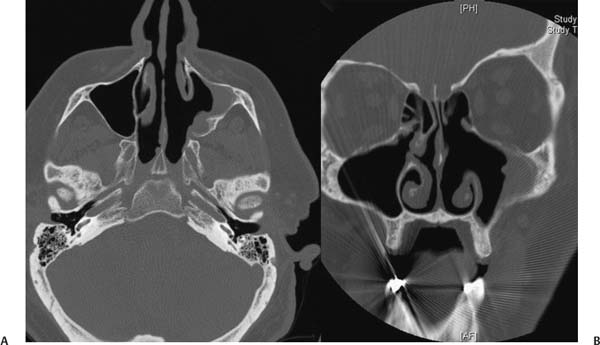
24 Learning from a Difficult Case: Recurrent Maxillary Sinus Inverted Papilloma As seen throughout this book, diseases of the maxillary sinus range from the simple to the complex and from the benign to the malignant. Likewise, medical and surgical approaches to these conditions vary and reflect both the nature of the disease and the skill set of the surgeon. Therefore, recalcitrant disease of the maxillary sinus often requires innovative treatment paradigms to completely eradicate disease. Inverted papilloma (IP) is a benign exophytic and polypoid soft tissue neoplasm arising from Schneiderian (ectodermal) mucosa characterized by inward growth of the neoplasm through the mucosa.1–3 It is also noteworthy for its locally aggressive nature, rate of recurrence, and rate of conversion to squamous cell carcinoma.1–8 In the not-so-distant past, resection of IPs was performed through numerous open approaches with long-term rates of recurrence ranging from 20 to 100%9 and often significant morbidity. More recently, the endoscopic resection of IPs has been described.4,8–14 In addition to superior illumination and magnification, the endoscopic removal of IP can result in improved outcomes4 with a greater degree of patient acceptance. Despite the evolution of hand instruments and the introduction of stereotactic navigation, certain areas of the paranasal sinuses continue to present technical challenges due to prohibitive anatomy. The lateral and anterior walls of the maxillary sinus represent two such areas. In many instances, endoscopic resection must be combined with external approaches (e.g., Caldwell–Luc or midfacial degloving procedure) to reach these areas. The modified endoscopic medial maxillectomy (MEMM) has been described for the resection of sinonasal neoplasia,15,16 as well as in revision surgery for recalcitrant inflammatory disease.17 Using this technique, areas of the maxillary sinus previously inaccessible during endoscopic sinus surgery (ESS) may be reached and tumors such as an IP can be effectively removed through this approach. We present a case of a patient with recurrent IP based on the lateral wall of the maxillary sinus and demonstrate how this extended endoscopic procedure can be used successfully to treat tumors in this location. A 53-year-old male patient with a Krouse stage III inverted papilloma of the left maxillary sinus presented with recurrent disease. Examination revealed a wide maxillary antrostomy with partial resection of the middle turbinate and partial ethmoidectomy. Small foci of implanted IP in the ethmoid and frontal recess and recurrent IP in the posterior and lateral aspects of the maxillary sinus were identified. With a 0-degree telescope, inspection of the tumor within the maxillary sinus was challenging due to the limitations presented by the anatomy. With the use of a 30-degree telescope, the tumor could be seen more extensively (Fig. 24.1); however, the delineation between tumor and normal tissue was challenging due to the limitations presented by the patient’s anatomy. Computed tomography (CT) was used to assess the extent of recurrence. Computed tomography in patients with IP is very helpful in determining the site of attachment because bony thickening has been reported to be associated with the pedicle of the tumor.18 In this patient, repeat CT imaging revealed a soft tissue mass in the posterior and lateral aspects of the left maxillary sinus and bony thickening along the lateral aspect of the maxillary sinus (Fig. 24.2). This correlated with the identified location of recurrence. Fig. 24.1 Endoscopic view of the tumor with a 30-degree telescope. A, The inferior turbinate, B, middle turbinate stump, and C, inverted papilloma can be seen. Even with a 30-degree telescope, the complete extent of the tumor cannot be seen. Fig. 24.2 (A,B) Computed tomography (axial and coronal) of the patient with recurrent inverted papilloma. (A) In the axial image, note the region of soft tissue thickening centered on the lateral aspect of the left maxillary sinus. (B) There is an area of thickened bone which represents the likely site of attachment. In the coronal image, the lateral, superior, and inferior extent of the tumor can be seen. The MEMM is performed under general anesthesia with the use of total intravenous anesthesia (TIVA). The use of TIVA has been shown19,20 to reduce intraoperative blood loss and is helpful in cases involving extensive surgery when blood loss might be expected to be high. Preoperatively, the nose is decongested topically with 0.5% oxymetazoline, and 4% topical cocaine is used prior to endoscopy. The mucosa of the inferior turbinate and lateral nasal wall is infiltrated with 1% lidocaine with 1:100,000 epinephrine to help achieve hemostasis. Additionally, a transoral pterygopalatine injection can be performed by inserting a 25-gauge needle bent at 2.5 cm into the greater palatine foramen opposite the second molar to provide additional vascular control. The majority of the resection is done with 4-mm, 30-degree, and 70-degree telescopes. In this case, an antrostomy and partial ethmoidectomy had been previously performed. (In the event that the maxillary sinus had not been previously entered, the uncinate process is resected with a sickle knife or backbiting instrument and the natural os of the maxillary sinus is identified midline along the maxillary line and is widened with through-cutting forceps or the micro-debrider.) Once a wide antrostomy is performed, the valve of Hasner is identified in the inferior meatus. The valve is located ~30 to 35 mm posterior to the limen nasi and must be identified prior to performing the maxillectomy; otherwise, the surgeon risks injury to the valve and/or lacrimal duct. An inferior turbinectomy is performed next using the endoscopic scissors. The inferior turbinate is incised between the anterior one-third and the posterior two-thirds of the turbinate, just behind the valve of Hasner. Cautery can be used to help with hemostasis, but care must be taken to avoid injury to the mucosal flap of the valve. Fig. 24.3 Endoscopic view of the modified endoscopic medial maxillectomy. The inferior turbinate has been removed. The medial maxillary wall has been made flush with the floor of the nasal cavity. Lastly, an inferior meatal window has been made to increase access to the anterior wall of the maxillary sinus. The mucosa along the lateral nasal wall is incised, and a mucoperiosteal flap is elevated toward the septum. (This flap is preserved and later draped into the maxillary defect.) A series of through-cutting instruments is used to resect the medial maxillary wall. If needed, a high-speed irrigating drill can be used to remove bone too thick for through-cutting punches. This is performed so that the maxillary sinus opens directly onto the floor of the nasal cavity. Because the valve of Hasner opens superiorly in the inferior meatus, the medial maxillary wall inferior to the valve of Hasner can be resected to provide additional exposure and room for instrumentation; this is performed with a backbiting instrument (Fig. 24.3) until the anterior wall of the maxillary sinus is reached near the piriform aperture. The use of navigation software (Fig. 24.4) can also be very helpful in confirming the precise anatomic location of the tumor and the exposure created during the approach. At this point, the exposure is complete (see Video 24.1) and the resection of the tumor begins. If the tumor is bulky in nature, it is carefully debulked until the site of attachment is reached. Using the curette and giraffe forceps, margins around the lesion are taken to ensure that preserved mucosa is free of tumor. Using the 70-degree endoscope and curved instruments, the tumor is carefully elevated off the posterior and lateral aspects of the maxillary sinus. In this instance, a malleable curved suction and curette is used to elevate the tumor off the bone. Instruments are passed through the medial maxillectomy as well as through the inferior meatal window to aid in the resection of the lesion. Once resected, the maxillary sinus is inspected thoroughly to evaluate for unaddressed foci of tumor. Stereotactic probes are used to correlate the endoscopic view with the CT images to confirm the completeness of the resection. Cautery is performed throughout the maxillary sinus to help achieve hemostasis and to fulgurate nests of IP. Because nests of IP have been demonstrated to infiltrate the underlying bone at the site of attachment, this bone must be removed.21 High-speed 15-degree and 70-degree rotating diamond burs are used to thin the bone along the attachment site of the tumor to address these nests (see Video 24.2). After a final inspection, the maxillary sinus is filled with a hemostatic agent. Fig. 24.4 Triplanar images of the patient during surgery. Notice that when the modified endoscopic medial maxillectomy has been performed, angled instruments can be used to access the inferior, lateral, and anterior aspects of the maxillary sinus. The postoperative care of the patient involves serial debridements and long-term surveillance. Given the considerable rates of recurrence,4,8,15 long-term surveillance is necessary in these patients, and particular attention to the pathology for the presence of any degeneration into squamous cell carcinoma is necessary. Irrigation with saline solution is proven to be beneficial and provide symptomatic relief to patients undergoing endoscopic sinus surgery.22–24 Irrigation also helps to manually debride blood clots and crusting.24 The role of antibiotics in this type of procedure has not been studied in a controlled manner; however, we believe prophylactic treatment with oral antibiotics is useful, especially in the presence of exposed bone where infection may easily occur. The MEMM presented here represents only one method of approaching and resecting the recurrent IP. As previously mentioned, a medial maxillectomy combined with a Caldwell–Luc procedure would have provided similar access with the benefit of a zero-degree telescope placed through the canine fossa into the antrum. The drawback of this adjuvant approach is the sublabial incision and canine fossa puncture. Other external procedures (midfacial degloving, open maxillectomy, etc.) could have been considered as primary or adjuvant surgical methods. Drawbacks of the external approaches are the incisions created and potential disfigurement and discomfort. Another method described by Harvey et al25 involves the creation of a septal window to obtain access to the lateral and anterior aspects of the maxillary sinus and simultaneously provide more direct visualization of the attachment site with a zero-degree or 30-degree telescope. The drawback of this approach is the creation of a controlled septal perforation that requires repair at the termination of the case. Recurrent IP can be a challenge to treat, especially if the tumor is attached to the lateral aspect of the maxillary sinus. However, the MEMM offers adequate exposure when combined with angled instruments and angled telescopes for the resection of difficult to reach tumor attachment sites within the maxillary sinus. • Intraoperative blood pressure and heart rate control, as well as thorough injection, will help minimize blood loss and improve visualization. • Preserving a nasal floor mucosal flap helps cover exposed bone after the case is completed. • Visualization with a 70-degree endoscope is performed through the mega-antrostomy while instruments can be passed through the inferior meatal window. • Use of image guidance can help confirm that all areas of the maxillary sinus are addressed by the surgeon. • Long-term surveillance is critical so that any recurrence is promptly identified and treated.
 Case Presentation
Case Presentation
History
Radiologic Evaluation
Operative Technique
Postoperative Care
 Alternative Procedures
Alternative Procedures
 Conclusion
Conclusion
Learning from a Difficult Case: Recurrent Maxillary Sinus Inverted Papilloma
Pearls
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


