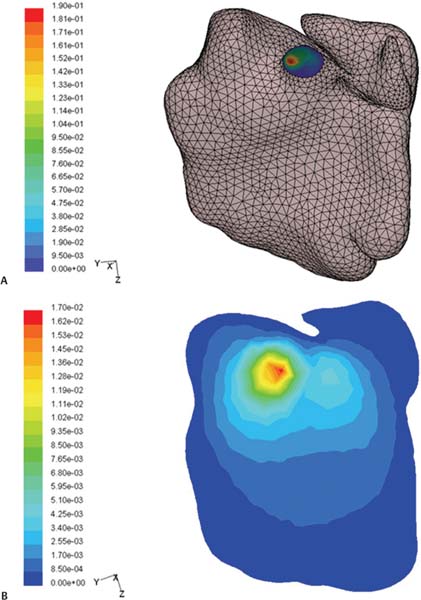
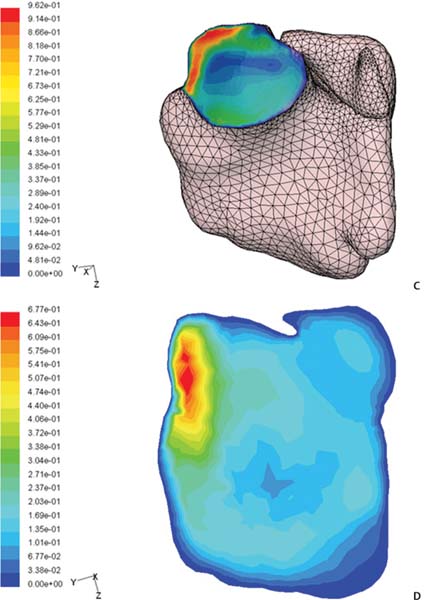
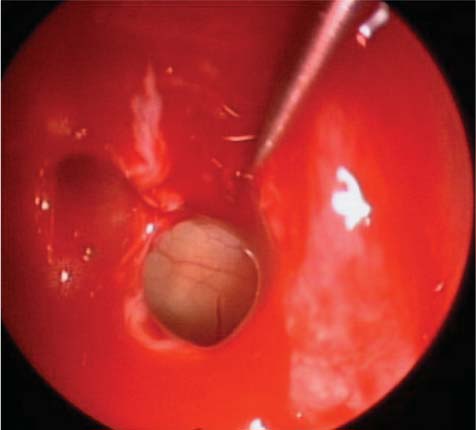
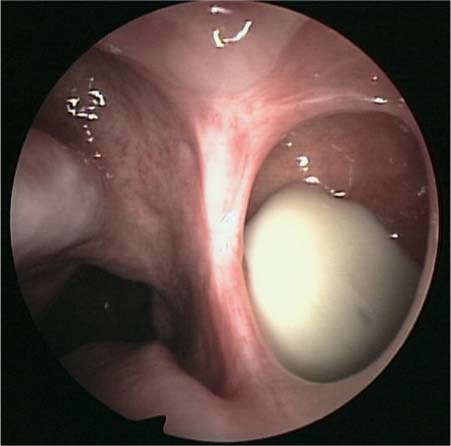
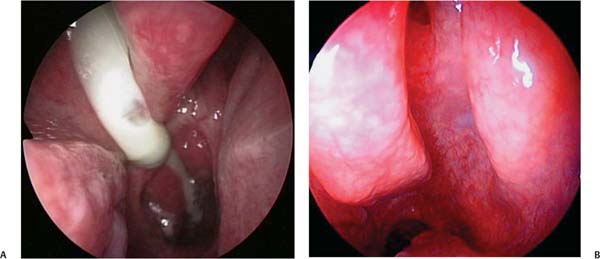
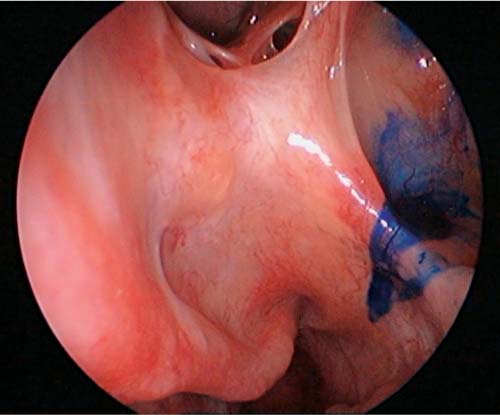
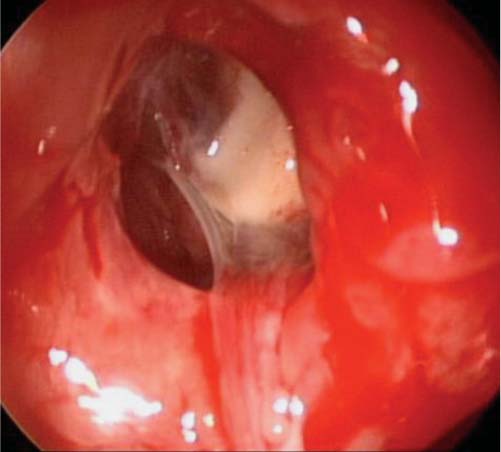
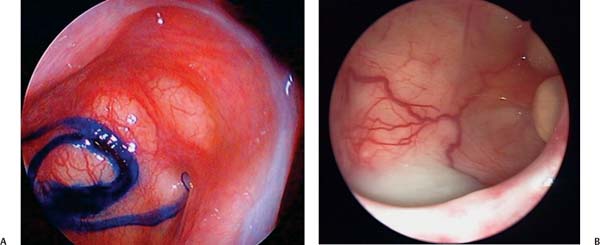
22 Management of Persistent Maxillary Sinusitis: The View from China When performing maxillary sinus surgery in our practice in China, we have found that the following points must be addressed: 1. Whether to open the maxillary sinus ostium 2. The position and scope of the opening 3. The opening pattern 4. Maxillary sinus disease management Fig. 22.1 (A–D) Computer simulation of nasal cavity and maxillary sinus air current and air exchange. After opening the maxillary sinus ostium, the maxillary sinus air current quantity changes. (A,B) Normal unoperated maxillary sinus ostium area. Note that only a small air current appears to enter the maxillary sinus proper (36.15 mL/s). (C,D) After enlarging the maxillary sinus ostium, air current into the sinus increases. The surgeon must determine whether a patient requires opening and enlargement of the natural ostium for the treatment of sinus disease. For the sinus to function in a healthy manner, the drainage pathway must be unobstructed. Obstruction of the sinus ostium results in a barrier to normal sinus ventilation and drainage, with consequent physiologic changes within the maxillary sinus. Changes in the oxygen and carbon dioxide composition, sinus pressure and airflow, pH, and ciliary function have all been documented in the obstructed and diseased sinus.1 Surgically opening a blocked sinus opening should be done in cases where it may help to reestablish a natural sinus environment. In our experience, the obstructed maxillary sinus ostia will often clear with medical treatment alone. In cases where inflammation is persistent, sinus outflow obstruction will not clear, polyps or other masses are present, surgery is indicated. However, surgery may change the sinus environment by opening it to the nasal passageway. The size and shape of the surgical opening may impact the characteristics of the sinus mucosa. In the normal nonoperated sinus, there is little exchange with nasal ventilation,2,3 in part due to the concealed nature of the natural opening by the uncinate process. When air enters the nasal cavity it does not directly interact with the maxillary sinus. To examine the relationship between nasal cavity ventilation and maxillary sinus aeration, we did a computer simulation of the nasal–paranasal sinus ventilation exchange. We found that in the normal unoperated condition, only a slight amount of air from the nasal cavity enters the maxillary sinus (2.938 mL/s). In the postsurgical maxillary sinus, this relationship changes significantly, and air enters the maxillary sinus at 5.914 mL/s (Fig. 22.1).4 It is possible that this change in sinus anatomy and ventilation is accompanied by a change in the sinus’ physiologic environment. Some authors have found that insufficient gas exchange in the maxillary sinus base is associated with an increase in maxillary sinus floor carbon dioxide differential pressure, and subsequent partial oxyphil agglomeration. In the normal condition, bacteria, viruses, and other foreign material that enter the nasal cavity invade the maxillary sinus itself very infrequently. In the postsurgical sinus, this relationship between the nasal cavity and the sinus is changed. Therefore, we advocate minimal surgery to the ostium itself in cases where the ostium can be healed by surgical removal of surrounding obstructive pathology (i.e., nasal polyps). In many cases, we believe opening or enlarging the maxillary sinus os may be unnecessary. We recall Professor Heinz Stammberger’s oft-repeated admonition at the First International Course of Functional Endoscopic Sinus Surgery in Vienna in 1992, “Maxillary sinus surgery is a surgery of the nasal cavity external wall.” One must recognize that surgical opening and enlargement of the sinus ostium will alter the internal sinus environment. Maxillary ostium mucous membrane inflammation and hypertrophy can create stenosis or blockage of the sinus outflow pathway. In these situations, the sinus ostium may require a surgical opening or expansion. When this is required, we favor the use of straight pliers to enlarge the ostium by roughly 0.5 to 1.0 cm. In some instances, due to severe mucous membrane polyposis or postoperative scar proliferation the surgical ostium may become obstructed again. When this occurs, we favor the use of further expansion and enlargement of the interior maxillary sinus wall. It has been well documented that the natural drainage pathway of the maxillary sinus is toward the natural ostium located in the anteromedial aspect of the sinus. This drainage pathway persists even in the light of surgical openings made elsewhere along the medial sinus wall.5–8 Research in support of this concept has been performed in China, as well. In one study, an inferior meatal antrostomy was created in patients with maxillary sinus infections. Subsequently, using a 70-degree nasal endoscope for guidance, dye was placed into the sinus through the inferior antrostomy. Drainage of this dye was then observed over a 60-minute period. Of 11 patients enrolled in this study, the dye in seven patients discharged through the natural ostium, whereas the dye in four patients discharged through both the ostium and the inferior nasal meatus orifice. In two of the seven patients, persistent empyema prevented drainage through the inferior antrostomy site (Fig. 22.2). Fig. 22.2 Endoscopic image showing that maxillary sinus empyema cannot be drained from the inferior meatus artificial orifice. Fig. 22.3 Endoscopic image demonstrating left maxillary sinus ostium opening/expansion. Fig. 22.4 Endoscopic image showing that because of the scars around the maxillary sinus ostium, the sinus empyema cannot drain. The results of this study support the concept of the surgical enlargement of physiologic drainage pathways as opposed to the creation of alternate sites of gravity-dependent drainage. This study reinforces the principle that in cases of maxillary sinus surgery, it is more favorable to enlarge the natural aperture, and not to create a secondary artificial orifice (Fig. 22.3). At present, most sinus surgeons in China adhere to this principle and favor enlargement of the natural maxillary ostium over creation of an inferior meatal artificial orifice. Improvement of maxillary sinus drainage may require opening or expanding the natural ostium. In some cases, even when the surgical antrostomy is open, the sinus secretions agglomerate and pool in the sinus cavity, resistant to discharge (Fig. 22.4).9 Situations such as this indicate that the maxillary sinus cilium system’s route of transmission is blocked despite an apparently open surgical antrostomy. Several experiments at the Otorhinolaryngology Hospital of the First Affiliated Hospital of Sun Yat-sen University were designed to shed light on the pathophysiology underlying this obstruction to sinus drainage. One-hundred thirty unoperated sinuses were examined, along with 30 postsurgical sinuses. The following observations were made. • Ninety-seven of 130 (71%) unoperated sinuses had a “dry river bed” type drainage pathway in which mucous from the maxillary sinus was swept by cilia over the inferior edge of maxillary ostium, passed through the “the river bed” area along the medial aspect of the turbinate into the lower middle nasal meatus, and then drained into the nasopharynx (Fig. 22.5). • The maxillary ostium superior, inferior, anterior, and posterior quadrants are covered entirely by cilia. The cilia length and the density do not have significant differences in these quadrants. There is a lack of nonciliated cell or secretory cell’s distribution nearby. The cilia direction in all quadrants sweeps mucous toward the inferoposterior area of the ostium. • Regardless of patient position—upright, seated, or supine—dye which is placed into the maxillary sinus exits via the ostium inferior edge, drains, and enters the middle nasal meatus directly (Fig. 22.6). Even when the maxillary sinus is filled with purulent secretion, discharge is still via the inferior edge of the ostium (Fig. 22.7). • In the postsurgical group of 30 participants who had a ring-like expanded maxillary ostium, drainage was along the inferior edge in 4 participants (13.3%), and along the posterior edge and/or superior edge in 17 participants (56.7%) (Fig. 22.8). In nine participants (30%), the tracer material accumulated in the maxillary sinus cavity and/or the sinus assumed revolving/circular transmission movement (Fig. 22.9). • In the postsurgical group where the inferior edge mucosa was retained, the sinus mucous in every case (100%) (Fig. 22.10) entered the middle meatus via the inferior edge of the ostium. Fig. 22.5 Endoscopic images showing (A) the drainage channel of the maxillary sinus ostium inferior quadrant “the river bed type,” and (B) the drainage channel of the maxillary sinus ostium inferior quadrant “the river bed type,” which directly drains into the nasopharynx. Fig. 22.6 Endoscopic image demonstrating the maxillary sinus filled with purulent secretion, which drains from the inferior edge of the ostium. Fig. 22.7 Endoscopic image shows that the maxillary sinus ostium inferior edge is the site for natural sinus drainage via cilia transmission. Fig. 22.8 Endoscopic image demonstrates that after a circumferential enlargement of the maxillary sinus ostium, the maxillary sinus displays delayed drainage. Note that the dye placed in the sinus cannot cross the inferior edge of the scar belt. This dye eventually drained out of the maxillary sinus in a superior direction into the ethmoid sinus area. From these clinical observations, the following conclusions were made. • The maxillary sinus ostium inferior edge is the primary drainage pathway for secretions from the maxillary sinus to enter the middle meatus. • In the postsurgical sinus in which the inferior edge of the ostium has been retained, maxillary sinus cilia transmission and drainage route do not differ between the postoperative and the nonoperated sinus. • After a ring-like, circumferential surgical enlargement of the maxillary ostium, the scar ribbon may alter the out-flow pathway of maxillary sinus cilium. In this situation, natural drainage patterns are observed in a minority of patients. The majority of patients who undergo circumferential enlargement of their natural ostia experience altered drainage into the middle meatus via the superior or posterior edges. In many of these cases, sinus drainage occurs with difficulty and at an altered rate. • In functional endoscopic sinus surgery (FESS) if the surgeon has to open and enlarge the maxillary sinus ostium, we recommend enlargement in an anterior or posterior direction. We recommend leaving the inferior edge untouched so that the natural drainage “river bed” patterns may continue in the postsurgical sinus.9 Fig. 22.9 Endoscopic images demonstrating that (A) after circumferential enlargement of the maxillary sinus ostium, a ring-like scar belt has formed. Note that the dye material cannot cross into the middle meatus, and a rotary, circular drainage pattern has developed. (B) In this postsurgical sinus, thick mucopurulent fluid is retained in the sinus and is unable to drain into the nasal cavity due to surgical damage to the inferior edge of the sinus. Small chronic abscesses can also be appreciated residing within the sinus itself. In cases in which the maxillary sinus disease is secondary to mucous membrane inflammation and hypertrophy without the presence of an obstructive polyp or cyst, enlargement of the sinus ostium is often unnecessary. In cases where there is an obstruction to sinus drainage, the obstructive mass (e.g., polyp, cyst, etc.) does need to be excised. It is imperative to try to retain the underlying periosteum in all cases. Powered instrumentation may assist in this goal. In cases where the maxillary sinus mucous membrane has been removed (including the periosteum and basement membrane), there is often a proliferation of poorly functional connective tissue fibers. It is for this reason that every attempt should be made to preserve mucosal lining and periosteum during maxillary sinus surgery. Fig. 22.10 Endoscopic image of a postsurgical sinus in which the inferior edge was preserved: the dye drains over the inferior edge and is transmitted in a natural manner toward the nasopharynx. • Surgical opening of the maxillary sinus should include enlargement of the natural ostium. • In most situations, the enlargement of the maxillary sinus opening should be in a posterior, anterior, and superior direction. Whenever possible, the inferior edge should be left untouched so as not to interfere with natural mucociliary clearance. • Always try to prevent mucosal stripping, and always try to preserve the sinus periosteum.
 Whether to Open the Maxillary Sinus Ostium
Whether to Open the Maxillary Sinus Ostium
 Location and Size of the Maxillary Sinus Opening
Location and Size of the Maxillary Sinus Opening

 The Maxillary Sinus Ostium Opening Pattern
The Maxillary Sinus Ostium Opening Pattern


 Maxillary Sinus Disease Management
Maxillary Sinus Disease Management
Management of Persistent Maxillary Sinusitis: The View from China
Pearls
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


