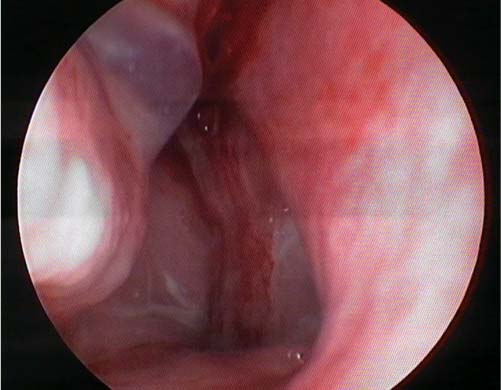
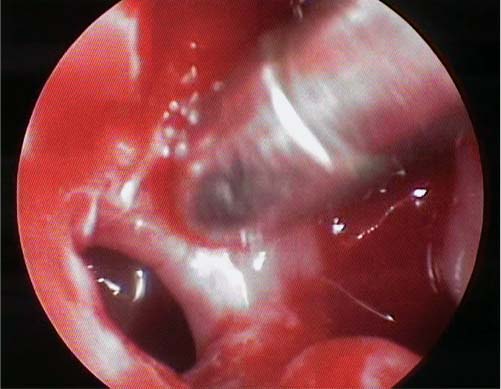
21 Management of Persistent Maxillary Sinusitis: The View from India Chronic rhinosinusitis (CRS) is defined as the mucosal inflammation of the nose and paranasal sinuses, persisting beyond a period of 12 weeks. Involvement of the maxillary sinus and ostiomeatal complex in CRS is a fairly common occurrence. During acute rhinosinusitis, in which there is generalized mucosal involvement of the nose and paranasal sinuses, the maxillary sinus is constantly soiled by the direct downpour of the inflammatory secretions from the frontal and anterior ethmoid sinuses. Due to its dependent position and mucociliary transport against gravity, acute inflammatory process within the maxillary sinus is more likely to become chronic and persistent if appropriate therapeutic intervention is not done. Although making a diagnosis of the patient with persistent maxillary sinusitis (PMS) is easy from its clinical symptoms and signs, endoscopic findings, and the radiologic images, the management of this condition is often difficult. In India, it is common to see patients presenting with PMS because of poverty and poor health care delivery. Despite multiple medical and surgical treatments being offered to them, patients with PMS show recurrences again owing to inadequacy of therapy and appropriate follow-up care. Diverse etiologic factors causing PMS also influence its poor results in India. The pathophysiology of PMS is a diverse process: it includes both intrinsic and extrinsic factors such as infective bacteria, virus, fungus, coexisting allergy, systemic causes like diabetes, immunodeficiency, and mucociliary disorders. Autoimmune disorders like sarcoidosis and Wegener granulomatosis, and anatomic abnormalities also play an important role. Mucus stasis within the maxillary sinus due to ostiomeatal obstruction or mucociliary dysfunction is the common basis of PMS. Persistent obstruction results in decreased oxygen tension, reduced sinus pH, ciliary dysfunction, negative pressure within the sinus and all these lead to stasis and such a collection invites infection. Associated sneezing due to allergies and nose blowing promotes the entry of the infectious agents from the nasal cavity into maxillary sinus resulting in rhinosinusitis. The inflammatory role played by virus, bacteria, and fungi is of importance as it causes host inflammatory responses due to local (mucosal) production of chemical mediators like cytokines. It eventually leads to persistent maxillary sinusitis (PMS). PMS has recently drawn a great deal of attention from both clinicians and basic researchers. The role of eosinophilic inflammation, biofilm formation, and superantigens needs special mention in the causation of persistent maxillary sinusitis. Studies1,2 have shown that biofilms, which are a structural community of cells of bacteria (Staphylococcus aureus and Pseudomonas aeruginosa) or fungus enclosed in a self-produced matrix, play a significant role in CRS. In addition to biofilm formation, colonization in the nose and paranasal sinuses of toxigenic strains of bacteria like S. aureus may also yield exotoxins with super antigenic properties, which are capable of producing eosinophilic and lymphocytic local inflammatory responses. Allergy also plays a role in PMS and allergic stimulation results in the release of histamine, leukotrienes, tumor necrosis factor, and cytokines. These recruit inflammatory cells. A clinical association between asthma and CRS has long been recognized. Increased levels of leukotrienes have been observed in patients having associated asthma and nasal polyps.3 In patients with PMS who receive antileukotriene therapy and experience improved outcomes suggests coexisting nasal allergy and/or asthma. Extra esophageal reflux diseases are also in the list of causative factors of refractory CRS.4 Patients with a history of maxillofacial trauma may present with PMS due to anatomic disruption of the ostiomeatal drainage mechanism. In older patients, PMS unresponsive to medical therapy should raise the suspicion of presence of a neoplastic condition involving the maxillary sinus. Such a patient needs a detailed assessment including a computed tomography (CT) scan and endoscopic biopsy from the suspected area for a confirmation of the diagnosis. The anatomic aspect of paranasal sinuses including the maxillary sinuses influences the pathophysiology of persistent maxillary sinusitis and so it needs a consideration. The maxillary sinus is the largest of the paranasal sinuses and is surrounded on all its sides by the bony walls, except on the medial side where the natural ostium and accessory one (when present) provides communication to the nasal cavity. The natural ostium is located in the superior aspect of the medial wall of the sinus, seen behind the lower attachment of uncinate process and above the superior portion of the inferior turbinate. The floor of the maxillary sinus is usually 4 to 5 mm below the floor of nasal cavity in adults and it explains the importance of mucociliary transport from the dependent portion of the sinus into the superiorly placed natural ostium and ethmoidal infundibulum. When the accessory ostium is present, it also plays an important role in the mucociliary transport and ventilation. The ethmoidal infundibulum is the common drainage point of the anterior group of sinuses: it is bound medially by the uncinate process, laterally by the lamina papyracea, and posteriorly by the anterior surface of ethmoidal bulla. It is obvious that anatomic abnormalities involving any of these structures like a bent or pneumatized uncinate process, prominent ethmoid bulla, and a Haller cell in the inferomedial aspect of orbit can compromise the drainage of the maxillary sinus. These abnormalities should be carefully looked into during endoscopic and radiologic assessment before making treatment plans in persistent maxillary sinusitis. Another anatomic consideration regarding the floor of the maxillary sinus is the close proximity of the root of the maxillary premolars and molars to the floor. Infection of the maxillary teeth, iatrogenic displacement of a maxillary tooth into the sinus, and injury to the sinus lining during extraction can also cause PMS of odontogenic origin. The most common symptoms are nasal congestion or blockage, purulent rhinorrhea, facial pain or pressure, discolored postnasal drainage, and anosmia or hyposmia. The other minor symptoms are headache, occasional fever, halitosis, fatigue, dental pain, dry cough, and ear pain/pressure/fullness. Maxillary sinusitis may also present with infraorbital pain and tenderness extending to the maxillary teeth. Children with PMS may not have the classical features and they may present with irritability as their only symptom. Persistent cough that is worse at night due to postnasal drip is another common feature seen in children. Intranasal examination with the help of nasal speculum and nasal endoscopic examination provides clinical evidence for the diagnosis of PMS. The status of the mucosal linings of the nose especially of the inferior and middle turbinates, middle meatus, presence of polyps and purulent secretions along the middle meatus help in diagnosing maxillary sinusitis (Fig. 21.1). Endoscopic examination also indicates the presence of anatomic abnormalities that may cause ostiomeatal blockage. In patients who have PMS after functional endoscopic sinus surgery (FESS), examination of the interior aspect of the maxillary sinus through the middle meatal antrostomy opening is important. It allows us to assess the condition of the mucosal lining of maxillary sinus, the presence of purulent secretions, and/or any residual/recurrent mucosal disease. Fig. 21.1 Endoscopic evidence of persistent maxillary sinusitis– mucopurulent secretions in the middle meatus. Culture-directed therapy is important in patients with PMS who are unresponsive to empirical therapy. Cultures may be taken from the middle meatus with a swab stick during endoscopic examination. Despite precautions, cultures are more prone to contamination: sinus aspiration/puncture helps in identifying the pathologic organisms involved in PMS. It is done by a sublabial canine fossa approach in adults and an inferior meatal approach under general anesthesia in children. It is not routinely indicated in immunocompetent patients with uncomplicated PMS keeping in mind the rare but serious complications such as soft tissue emphysema, air embolism, vasovagal reaction, and injury to the orbit. Patients with PMS who are immunocompromised and have failed to respond to multiple courses of antimicrobial therapy need a sinus aspiration for a diagnosis. A noncontrast computed tomography (CT) scan of the paranasal sinuses (Fig. 21.2) with axial and coronal cuts is our preferred radiologic modality for assessing PMS. The plain radiographs lack the sensitivity, specificity and anatomic precision. MRI is not preferred due to its limited ability to display bony details. A CT scan helps in diagnosing changes within the maxillary sinus like focal or diffuse mucosal thickening, extensive polyps, anatomy of the ostiomeatal complex and anatomic abnormalities causing obstruction to the drainage pathway. It helps in assessing the response to treatment and also preoperative planning. It is very important to know whether symptoms of PMS correlate with the CT findings before determining the need for a surgical intervention. Studies have shown that there is CT evidence of asymptomatic paranasal sinus changes in patients without CRS,5,6 and in such a situation therapy is controversial. Fig. 21.2 Computed tomography (CT) coronal section showing complete opacification of the left maxillary sinus in persistent maxillary sinusitis. PMS may present as three conditions with regard to its management: (1) PMS without polyp, (2) PMS with polyp, and (3) PMS after endoscopic sinus surgery. The treatment approach is different for each of these conditions. These patients present with clinical symptoms of PMS persisting beyond a period of 12 weeks without any polyps in the middle meatus or nasal cavity on endoscopic examination. They present with characteristic endoscopic findings of rhinosinusitis (erythema, edema, nasal purulence) in the middle meatus and radiologic evidence of localized or diffuse mucosal thickening, partial opacification of maxillary sinus/ostiomeatal complex. Though all three factors (clinical symptoms, endoscopic examination, and radiologic examination) are assessed before therapy, treatment of these patients depends mainly on the clinical symptoms. If the symptoms are mild, intermittent with absence of nasal purulence, a short course of topical intranasal corticosteroid therapy for 8 weeks is indicated. The efficacy of treatment is assessed after 8 weeks by monitoring the improvement in symptoms and resolution of endoscopic findings. If there is good response to treatment, topical intranasal corticosteroids should be continued for at least 6 months as maintenance therapy. If the patient with PMS has severe, frequent, and continuous symptoms or symptoms affecting the patient’s daily activities, supported by endoscopic and radiologic findings, empiric therapy with broad-spectrum antibiotics should be given for 3 weeks. In ideal settings, culture-directed therapy is preferable over empiric treatment, as it targets the specific organism. Though culture-directed therapy may not be possible in all cases because of time constraints, it should be tried in patients in whom empiric antimicrobial therapy has failed and before contemplating FESS. Along with the antibiotics, topical intranasal corticosteroid therapy may be given for 6 to 8 weeks. A short course of oral steroids for 7 to 10 days before embarking on topical corticosteroid therapy is also recommended to treat the inflammatory component associated with PMS provided there are no contraindications. Saline spray/irrigation is helpful in the decongestion of the inflamed mucosa without causing rebound congestion like topical nasal decongestants. Saline irrigation also helps in washing away the inflammatory secretions and improves the mucociliary transport. If there is good response to this treatment, patients should be put on maintenance therapy with topical corticosteroid nasal spray for 6 months or longer as long as the symptoms warrant. If there is poor response, patients with PMS should be considered for FESS. Endoscopic and radiologic assessment helps in differentiating limited disease (polyps limited to the middle meatus or polyps beyond middle meatus but not obstructing nasal cavity) from extensive disease (polyps completely obstructing the nasal cavity). Patients with PMS with limited nasal polyposis and mild symptoms of CRS can be treated with topical corticosteroid nasal spray alone for 2 months, and if there is good response, they should be put on maintenance therapy for a further 6 months. For patients with moderate or severe symptoms affecting daily activities and extensive nasal polyposis, a 2-month course of topical corticosteroid and a 3-week course of antibiotics (especially for cases with symptoms and signs of infection, i.e., pain and nasal purulence on endoscopy) should be given. Initial treatment with oral steroids is of additional benefit. If there is a good response, they should be put on maintenance therapy with topical corticosteroid nasal spray for 6 months or longer to minimize recurrence of polyps. If there is poor response after 2 months of medical treatment, patients with PMS with polyposis should be considered for FESS. In recent years, considerable evidence has emerged to suggest that macrolide antibiotics have an antiinflammatory effect7 in addition to their well-established antibiotic effect. Macrolides accumulate in inflammatory cells at higher concentrations and have been shown to inhibit cytokines, increase inflammatory cell apoptosis, and inhibit the activation of the key proinflammatory transcription factor. The preliminary analysis of our ongoing study on the efficacy of low-dose, long-term macrolide therapy (roxithromycin 150 mg or clarithromycin 250 mg once daily for 3 months) in CRS has shown improvement in both subjective (nasal symptoms) and objective (endoscopic and CT findings) outcome measures.8 Larger prospective randomized controlled trials are needed to know the efficacy of low-dose macrolide in PMS refractory to medical therapy and FESS. Nasal lavage for the treatment of chronic rhinosinusitis has gained attention in the world literature in last decade. “Jal-Neti” (nasal water irrigation therapy) is an ancient yogic practice of cleaning the nostril with lukewarm water with a special utensil (lota). In India, it has been practiced for centuries and is recommended by medical practitioners, allied medical professionals, and yogic experts for the treatment of chronic rhinosinusitis. “Sutra-neti” (nasal cleaning with thread) is another ancient yogic technique of nasal cleansing wherein a length of string is inserted through the nose and into the mouth. The end is then pulled out of the mouth and while holding both ends at once the string is alternately pulled in and out of the nose and sinuses to clean the nasal passages. Though it is in practice, sutra-neti is not recommended by the medical professionals for the treatment of chronic rhinosinusitis in view of associated trauma to the already inflamed nasal mucosa. It is assumed that intranasal application of the antifungal agent amphotericin B in the form of nasal lavage (20 mL of 100 μg/mL solution twice daily in each nostril) would reduce the fungal load by mechanical irrigation as well as reduce the immunologic changes produced by fungus in the nose and sinuses in patients with allergic fungal rhinosinusitis (AFRS). Topical antifungal nasal lavage when combined with the corticosteroid (fluticasone) nasal spray, which has antiinflammatory properties will have an additive effect in the treatment response. Although there is strong evidence to support the role of fungi in AFRS, there is a lot of controversy over the role of fungi in nonallergic CRS. Studies9,10 have shown the presence of a fungal colony in the nose of normal volunteers and also in risk groups (such as patients with anatomic abnormalities like a deviated nasal septum, allergy to dust/pollens, house mites, etc.). In our experience, combination therapy of amphotericin B nasal lavage and topical corticosteroid nasal spray was found to be very effective in the treatment of AFRS with improvement in nasal symptoms, and endoscopic and radiologic findings.11–14 Uncinectomy is the first and the most important step in FESS. If poorly performed, it results in surgical failure. The uncinate process can be seen as the union of three anatomic parts, upper or anterosuperior one-third, middle one-third, and posterior or horizontal one-third. In FESS, it is necessary to remove both the middle one-third to expose the natural ostium of maxillary sinus and the horizontal one-third of the uncinate process to allow the mucosa of ostium to be trimmed delicately and to heal by primary intention without scarring (see Video 21.1). The removal of the upper one-third of the uncinate process is not indicated in the surgery of maxillary sinus and the ostiomeatal complex unless there is associated disease in the frontal sinus. The fontanelles (membranous areas in the medial wall of the maxillary sinus) are classified as anterior and posterior fontanelles in relation to the natural ostium. Failure of the surgeon to identify the natural ostium and the forceful insertion of angled instruments into the membranous part of the medial wall results in the creation of a posterior fontanelle ostium. It results in the circular flow of mucus and inflamed secretions between the unidentified natural ostium and the newly created posterior fontanelle ostium resulting in PMS after ESS.15 This can be easily prevented by correct identification of the natural ostium after uncinectomy, the avoidance of blind instrumentation in the medial wall, and if an accessory ostium is found it has to be surgically joined with the natural ostium. The studies in literature are not conclusive regarding the ideal size of the maxillary sinus ostium to be made in FESS.16,17 For all practical purposes, if the maxillary sinus has minimal disease, uncinectomy and opening of the blocked natural ostium is sufficient for the long-term health of the sinus (Fig. 21.3). If there is extensive polyp formation with thick and viscid secretions, a large maxillary antrostomy is required. Failure to remove the polyps attached to the anterior and inferomedial wall of the maxillary sinus is another cause for PMS after FESS. This may occur due to two reasons: (1) the inability to visualize the interiors of the maxillary sinus, and (2) the inability to remove the disease even after visualization. Better visualization can be achieved with angled endoscopes such as a 30-degree and 70-degree telescope. The removal of polyps from inaccessible areas can be achieved by angled forceps/microdebrider via the middle meatal antrostomies (see Video 21.1) or in difficult circumstances by canine fossa puncture. Canine fossa puncture by a sublabial approach helps in the easy insertion of instruments/microdebrider via a small opening made in the canine fossa of the anterior wall of maxillary sinus for the removal of polyps. Fig. 21.3 Opening of blocked natural ostium during endoscopic sinus surgery. Endoscopic examination and cleaning at regular intervals in the first 6 to 8 weeks after FESS is crucial for a good postoperative outcome. This helps in the healing process and improves the drainage and ventilation of the sinuses. If symptoms of sinusitis are persistent even after 8 weeks, endoscopic examination and radiologic assessment with CT scanning is required. Endoscopy helps in identification and treatment of causes of mechanical obstruction like crusts and synechiae formation. A CT scan helps to identify the residual/recurrent polyp within the sinus, mucocele formation, and anatomic factors causing obstruction to sinus drainage. Though anatomic factors causing obstruction and a mucocele has to be dealt by revision endoscopic sinus surgery, PMS with or without residual/recurrent polyps within the sinus can be treated with topical steroid spray and low-dose long-term macrolide therapy before embarking on FESS again. Topical instillation of antibiotics18 (e.g., tobramycin) and irrigation with steroid solution are also helpful when there is evidence of continued inflammation, as these procedures allow the delivery of a higher concentration of medication to the affected sinus mucosa and minimizes the systemic side effects of medications. In the management of patients with PMS who are refractory to medical or surgical treatment, it is important to consider the potential contribution of allergy to their symptoms. Allergy management should be included in the treatment protocol of PMS with or without polyp. Allergy management includes allergen reduction, avoidance, medications, and in extreme cases immunotherapy. It is also important to rule out systemic causes like immunodeficiency disorders and autoimmune diseases in patients with PMS who are refractory to treatment. The management of persistent maxillary sinusitis continues to evolve. It is very important to understand the etiopathogenesis of this condition in a broad range and not focus on bacterial infection alone. The comprehensive management of PMS requires an understanding of the role of infective organisms with its characteristic biofilm formation and superantigen production, role of inflammatory process perpetuated by eosinophils, lymphocytes and their chemical mediators, the diverse etiological factors including anatomic abnormalities and the possible role of allergy. Treatment options include pharmacotherapy and surgery. The pharmacotherapy should be based on the etiopathogenesis and it includes antibiotics, topical/systemic steroids, topical antifungal therapy, and novel antiinflammatory therapies like antileukotrienes and low-dose macrolide therapy. Surgical treatment involves functional endoscopic sinus surgery with the aim to preserve function and provide ventilation to the affected sinus. Endoscopic sinus surgery should be contemplated for patients with moderate to severe disease with extensive polyps and patients with persistent maxillary sinusitis refractory to medical therapy. • The pathophysiology of PMS involves both intrinsic and extrinsic factors. • The role of eosinophilic inflammation, biofilm formation, and superantigens needs special mention in PMS. • Clinical symptomatology, endoscopic findings, and radiologic assessment are crucial in the diagnosis and management of PMS. • Nasal swab/sinus aspiration and culture is indicated in patients with PMS who are immunocompromised and unresponsive to empirical therapy. • Medical treatment for PMS includes antibiotics, topical/systemic steroids, antileukotrienes and low dose, long-term macrolide therapy. • Functional endoscopic sinus surgery is indicated in patients with PMS refractory to medical therapy and in those with extensive polyps.
 Etiopathogenesis of Persistent Maxillary Sinusitis
Etiopathogenesis of Persistent Maxillary Sinusitis
 Anatomic Considerations in the Pathophysiology of PMS
Anatomic Considerations in the Pathophysiology of PMS
 Clinical Presentation of Persistent Maxillary Sinusitis
Clinical Presentation of Persistent Maxillary Sinusitis
 Diagnosis
Diagnosis
The Role of Nasal Swab, Sinus Aspiration, and Culture
Imaging in PMS: The Indian Experience
 Treatment of PMS
Treatment of PMS
Treatment of PMS with Polyposis
Treatment of PMS without Polyp
The Indian Experience: Low-dose Macrolide Therapy and Topical Antifungal Nasal Lavage in PMS
Endoscopic Sinus Surgery for PMS
Management of PMS after Functional Endoscopic Sinus Surgery (FESS)
 Conclusion
Conclusion
Management of Persistent Maxillary Sinusitis: The View from India

Pearls
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


