Fig. 110 The size of the mastoid air cell system found by Diamant (1940) in consecutive patients hospitalized for scarlet fever. The dashed line indicates the Gaussian curve. After Diamant (1940)
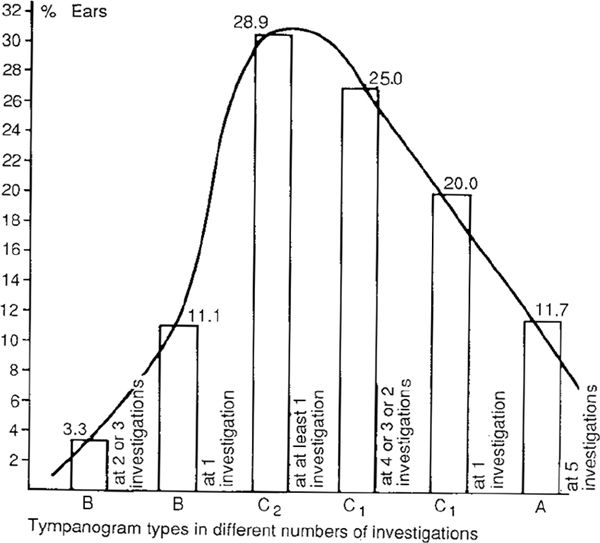
Fig. 111 The Gaussian distribution of the severity and duration of middle ear and tubal diseases expressed in five tympanograms obtained during the first year of life in 90 otherwise healthy infants (180 ears). The most severe, ears are on the left side of the curve, and the completely healthy ears are on the right (Tos, Acta Otolaryngol, 1982b)
In our second cohort, consisting of 184 otherwise healthy two-year-old children followed up over 27 months by six tympanometries, a Gaussian curve of severity of disease was also found (Fig. 112).
In our third cohort consisting of 288 four-year-old children investigated by five tympanometries every three months for one year, 73% had type B or type C2 tympanograms at least once. The severity of tubal dysfunction and secretory otitis media again had an almost Gaussian distribution (Fig. 113).
By performing quantitative histology on autopsy material for children over two years whose middle ears were clinically normal, we found mucous glands in the middle ear mucosa in 90% of the ears (Bak-Pedersen and Tos 1973). The mucous glands were definitely pathological, and were formed due to previous disease, either secretory otitis or acute otitis media. Normally there are no glands in the middle ear mucosa. The distribution of the total number of glands was again Gaussian (Fig. 114).
At autopsies from clinically normal temporal bones from adults, mucous glands were found in 91 % of the middle ears. As regards the total number of glands, the material showed an almost Gaussian distribution (Fig. 115). The glands found in adults are thought to be sequelae of pathological changes of the mucosa in childhood (Bak-Pedersen and Tos 1973).
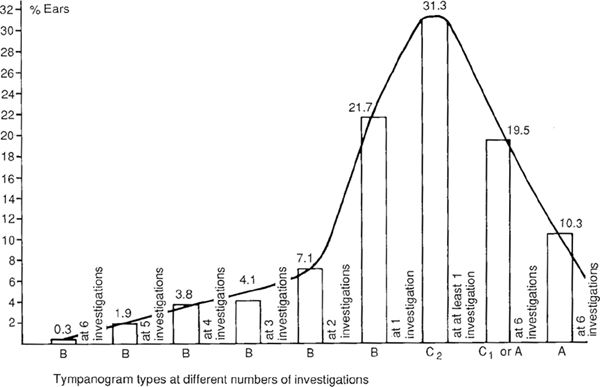
Fig. 112 The Gaussian distribution of the percentage of 368 ears with different combinations of severity and duration of middle ear diseases in 184 2-year-old children followed with six tympanometries during a 27-month period (four tympanometries every three months, the fifth six months later, and the sixth 12 months later) (Tos 1982b)
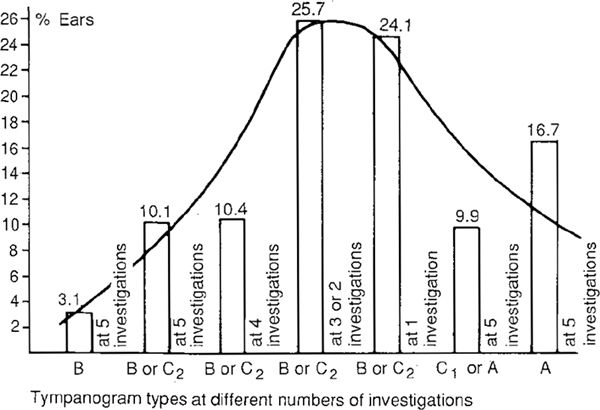
Fig. 113 A similar Gaussian curve to those in Figures 111 and 112, but based on five repeated tympanometries every three months in a different study group consisting of 288 4-year-old children (576 ears) (Tos 1982b)
These studies have shown that the middle ear mucosa in childhood, when the pneumatization process is taking place, is exposed to pathological stimuli of various degrees of severity and duration. These stimuli may have a considerable effect on the process of pneumatization, the end results of which may be large variation in the size of the cellular system.
It is well known that the process of pneumatization takes place from birth throughout childhood. It is also well known and documented by several human histological and experimental studies (Sadé 1979, Tos 1980a) that the mucosa is severely pathologically altered in secretory otitis media and in acute suppurative otitis media. It was shown by Wittmaack (1918) that pathological changes in the mucosa hamper the developing process of pneumatization, and the variation in the size of the cellular system can be fully explained by the range of exposure to disease. The Gaussian distribution of the variations in size of the air cells, which is the cornerstone of the hereditary theory can thus—with better evidence—be taken as the cornerstone of the environmental theory. Diamant’s so-called “normal” population of children and adults were—as in our materials—exposed to upper respiratory tract infections during early childhood, resulting in secretory otitis media and acute otitis media that influenced the process of pneumatization and resulted in the variation of the air cell system.
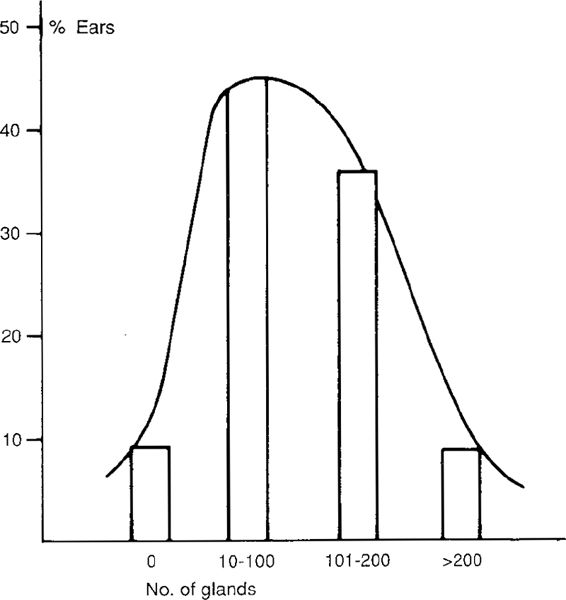
Fig. 114 The total number of abnormal mucous glands found in the middle ear mucosae of 11 temporal bones from children with clinically normal middle ears (Tos 1982b)
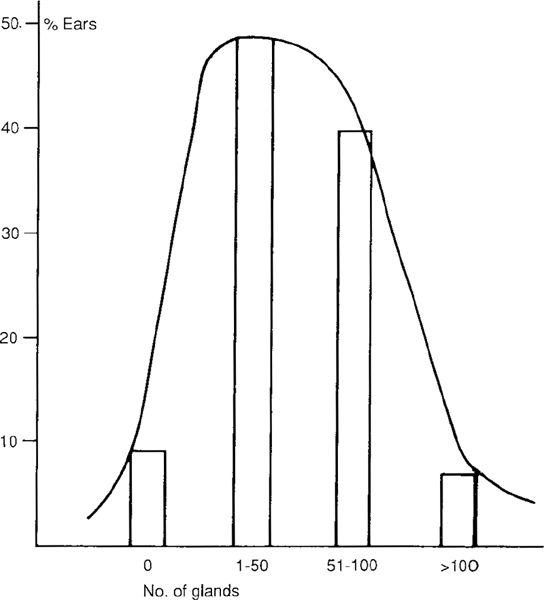
Fig. 115 The total number of abnormal mucous glands found in the middle ear mucosae of 45 clinically normal middle ears in adults (Tos 1982b)
The Size of Air Cells and Previous Disease
Our epidemiological studies provide definitive proof that the variation in size of the air cells system is a direct consequence of previous disease.
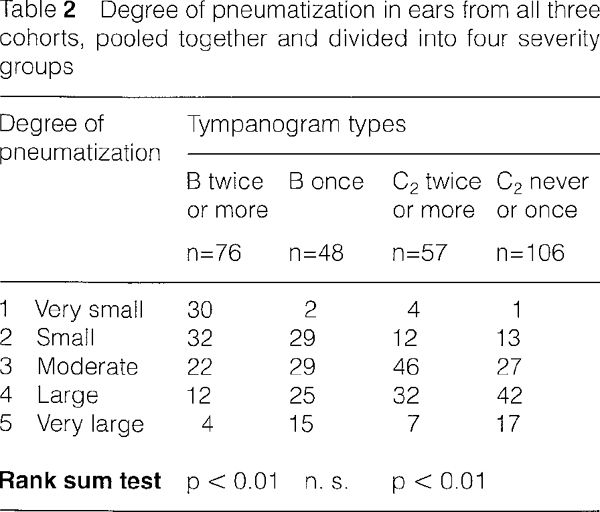
The three cohorts of otherwise healthy children (Figs. 111–113) followed up by several repeated tympanometries and otomicroscopies have also been examined radiologically, and the size of the air cell system was measured planimetrically and blindly estimated. Forty-one children from the first cohort (Tos et al. 1984a) were radiologically examined at the age of six, after 13 tympanometries (Fig. 111), as were 79 children from the second cohort (Tos et al. 1985) at the age of seven, after nine tympanometries (Fig. 112), and 41 children from the third cohort (Tos and Stangerup 1984) at the age of eight, after seven tympanometries (Fig. 113). At the time of evaluation, the middle ears of all the children were clinically healthy, but children with a history of previous secretory otitis media of a severe or extended duration had significantly smaller air cell systems than children with a history of limited disease (Table 2). Significantly, the largest air cell systems were found in children with no previous disease.
It has also been demonstrated that individual asymmetry in the size of the cell system can be attributed to a history of more extensive previous middle ear pathology on the side of the smaller cell system (Tos and Stangerup 1985a). It has also been shown that the reason why boys have smaller air cell systems is that they generally have more middle ear disease during infancy than girls (Tos and Stangerup 1985b). It has also been shown that the insertion of grommets has a positive effect on the process of pneumatization (Stangerup and Tos 1986).
The Pneumatization Process
The normal process of pneumatization starts in the perinatal period in the last weeks before birth, and progresses during infancy and childhood through to puberty, when the last part of the petrous apex is pneumatized.
Embryonic mesenchyme, which in the eighth fetal month is found in the upper two-thirds of the tympanic cavity, is gradually reduced. At birth, the entire tympanic cavity is filled with air, with the antrum still partly filled with mesenchyme.
The pneumatization of the mastoid process starts at birth with the development of the periantral cells, and continues through early childhood toward the mastoid tip. From the antrum, pneumatization continues toward the labyrinth and the apex of the pyramid (Wittmaack 1918, Rainer 1938). At puberty, the last part of the petrous bone is pneumatized. Air cells of the mastoid process start to develop from the antrum, but some peritubal and hypotympanic cells develop from the Eustachian tube and the hypotympanum, respectively. Some air cell tracts originating in the hypotympanum continue toward the mastoid process, passing medially to the vertical portion of the facial nerve.
The pneumatization process of the air cells can be divided schematically into three stages: 1) Lacunar resorption of the bony trabeculations of the spongiotic bone by the mesenchymal tissue. In the lacunas, extensive osteoclastic activity is found. 2) Invasion of fibrous tissue into the lacunar spaces and displacement of the bone marrow. 3) Disappearance of the fibrous tissue and ingrowth of epithelium into the air cells. Further lacunar resorption of the bone takes place at the base of the cells, and formation of new air cells starts again in the same manner. This process continues as long as there is spongiotic marrow in the temporal bone. The normal process of pneumatization requires normal middle ear mucosa, and is disturbed and delayed by any pathological process in the middle ear, such as infection or inflammation.
The Air Cell Tracts
The air cell system of the temporal bone can be divided into:
1. Mastoid air cell tracts, which are the result of the mastoid pneumatization, originating in the antrum.
2. Petrous bone cell tracts, divided into a) perilabyrinthine cell tracts, which are the result of petrous bone pneumatization starting in the antrum, and b) petrous apex cell tracts, originating in the antrum, hypotympanum, and Eustachian tube.
3. Sublabyrinthine cell tracts, originating from the Eustachian tube and hypotympanum.
4. Precochlear or inferior prelabyrinthine cell tracts, originating from the antrum, Eustachian tube, and hypotympanum.
Mastoid Air Cells
Since the antrum is the site of origin of the mastoid air cells, the first to develop are the periantral and tegmental cells, as well as the central mastoid cells.
In adults, several mastoid air cell systems can be distinguished. They can be divided and subdivided in various ways, and the classification described by Allam (1969) and slightly modified by the present author will be used here (Fig. 116).
1. The periantral cells surround the antrum on all sides and occupy the anterosuperior portion of the mastoid process (Fig. 116).
2. The tegmental cells extend along the middle fossa dura plate. They can be subdivided into mastoidal tegmental cells, antral tegmental cells, and tympanic tegmental cells, relating to the classification of the three subdivisions of the tegments stressed by the author. The periantral cells are in fact antral tegmental cells (Fig. 116).
3. The sinodural cells occupy the sinus dura angle and are bounded superiorly by the middle fossa dural plate, and Inferiorly by the dural plate over the superior part of the sigmoid sinus (Fig. 116).
4. The perisinusal cells lie around the sigmoid sinus. They can be subdivided into posterior perisinusal cells, lying posterior to the sigmoid sinus, lateral perisinusal cells, lying lateral to the sinus, and medial perisinusal cells, lying medial and anterior to the sinus. Because the posterior perisinusal cells (or retrosigmoid cells) can reach far posteriorly into the occipital bone in extensively pneumatized ears, the present author has further subdivided them into the superior and inferior retrosigmoidal cells (Fig. 116).
5. The central mastoid cells occupy the central area, which extends from the antrum down to the mastoid tip. These cells are usually large cells (Fig. 116). They can be further subdivided into superficial and deep intersinofacial cells.
6. The mastoid tip cells or apical cells, which again are usually large cells, are subdivided into lateral apical cells, lying lateral to the digastric crest, and medial apical cells, lying medial to the digastric crest and inferior to the sigmoid sinus (Fig. 116).
7. The perifacial cells lie adjacent to the posterior and lateral aspects of the vertical segment of the facial nerve (Fig. 116). The cells of the facial recess are also perifacial cells. The perifacial cells connect with the tympanic cavity above the fossa incudis, not through the facial recess.
8. The zygomatic cells are divided into the lateral and medial zygomatic cells. They occupy the most anterior space between the posterosuperior part of the external auditory meatus and the middle fossa dural plate. They can extend anteriorly far into the zygomatic arch (Fig. 116).
9. The cells lying around the superior and lateral walls of the aditus ad antrum and the epitympanum are termed the antral cells (Fig. 116).
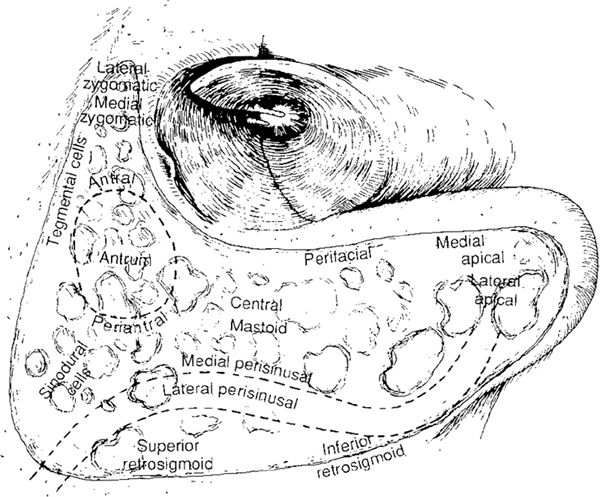
Fig. 116 The air cells of the mastoid process. Posteriorly around the sigmoid sinus lie the medial and lateral perisinusal cells, and behind the sinus the superior and inferior retrosigmoidal cells. In the mastoid apex lie the lateral and medial apical cells. Around the facial nerve are the perifacial cells. Around the antrum are the periantral cells, and toward the aditus ad antrum lie the antral cells. The tegmental cells are located along the middle fossa dura plate. Anteriorly, the lateral and medial zygomatic cells are seen.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


