Sympathetic Ophthalmia and Vogt-Koyanagi-Harada Syndrome
Chi-Chao Chan
Scott M. Whitcup
Robert B. Nussenblatt
SYMPATHETIC OPHTHALMIA
Sympathetic ophthalmia is defined as a bilateral granulomatous panuveitis that occurs after the uvea of one eye is subjected to a penetrating injury due to either accidental trauma or surgery. An alternative definition can be found in the work of Duke-Elder and Perkins1:
Sympathetic ophthalmitis is a specific bilateral inflammation of the entire uveal tract of unknown etiology, characterized clinically by an insidious onset and a progressive course with exacerbation and pathologically by a nodular or diffuse infiltration of the uveal tract with lymphocytes and epithelioid cells. It almost invariably follows a perforating wound involving uveal tissue.
This disease was known to Hippocrates and was fully described and named by MacKenzie in 1840.2 Schirman, as cited in Duke-Elder and Perkins,1 presented clinical data and supportive rabbit experiments in 1892 and 1905; however, it was Fuchs3 who described the classic histopathology as a distinct ocular disease in a treatise published in 1905. Capitalizing on the theme of sympathetic ophthalmia, Sir Frederick Treves was even able to develop a totally different medical subject into an entertaining horror story in his famous book “The Elephant Man and Other Reminiscences” in 1923.4
PREVALENCE
The prevalence of sympathetic ophthalmia is difficult to measure because it has always been a relatively rare disease; as a result of improvements in modern surgical and medical treatment, it has become even more uncommon. Still, on average, the older literature generally has found the incidence after a perforating injury to be approximately 2%.1 In the American Civil War (1861–1865), 16% of all ocular injuries led to the development of sympathetic ophthalmia. In the Franco-Prussian War (1870–1871), the prevalence of sympathetic ophthalmia after ocular injuries was 55.5% among the Germans and 50% among the French.5 In contrast, only rare cases of sympathetic ophthalmia were reported in World Wars I and II,3,5,6 and none were reported in the Korean, Vietnam, and Persian Gulf conflicts. Only one case is documented in the Iraq war.7 In surveys unrelated to warfare, Von Holland8 and Allen and Ho9 found sympathetic ophthalmia in 0.7% of 838 and in 0.3% of 348 cases of ocular trauma, respectively. In a retrospective analysis of 2,340 cases of open-globe injuries in Iran, 0.08% (two cases) were diagnosed with sympathetic ophthalmica from 1998 to 2003.10
After trauma, surgical wound is the second most important cause of sympathetic ophthalmia. Allen and Ho9 found one case (0.015%) of sympathetic ophthalmia in a survey of 6,613 cases of ocular surgery (5,325 cataract extraction and 1,288 glaucoma procedures). In 105 cases of sympathetic ophthalmia, Lubin et al11 found that traumatic perforating wounds accounted for 53.5% of cases, surgical wounds for 40.4%, perforating corneal ulcers for 6%, and malignant melanoma for 4%. Nevertheless, postsurgical sympathetic ophthalmia has been a rare event. Du Toit et al12 of the Cape Town Groote Schuur Hospital reported an incidence of 0.14% of sympathetic ophthalmia following penetrating trauma in 1,392 patients, among whom 1,283 underwent surgery on admission (primary repair or primary removal of the globe).
With the development of vitreous surgery and exploratory oculotomy in ocular trauma, however, sympathetic ophthalmia is becoming more prevalent. This may be partly explained by increased awareness and better diagnosis. In 1975, Michaels and Ryan13 reported that sympathetic ophthalmia is an extremely rare complication after vitrectomy. Since then, however, more isolated cases of sympathetic ophthalmia after several different intraocular surgeries, including pars plana vitrectomy, have been described.14,15,16,17,18,19,20 Other ocular surgeries that may induce sympathetic ophthalmia include iridectomy,11,21,22 iridencleisis,11,23 evisceration,24 retinal detachment repair,25,26,27,28,29 keratectomy,1,11,23 laser photocoagulation,19,30 laser cyclotherapy,31,32,33,34 local irradiation,35,36,37 and following vitrectomy for endophthalmitis after intravitreal bevacizumab.38 Kilmartin et al39 reported a minimum estimated incidence of 0.03/100,000 in the United Kingdom and Republic of Ireland. The main current risk is surgery, particularly retinal surgery.39 In a retrospective case series, sympathetic ophthalmia was diagnosed in 10 (1.08%) of 924 patients seen in the Singapore National Eye Center from 1993 to 2003.40 In this series, ocular surgery, especially vitreoretinal surgery, had overtaken nonsurgical trauma as the major cause of the disease.
Males have a higher prevalence of trauma-induced sympathetic ophthalmia than females, probably because males have higher overall injury rates.11,41 In postsurgical cases, however, the rates are equal between the sexes.41,42 Trauma-induced disease is more common among children, whereas postsurgical disease is more prevalent among older patients because of their increasing need for ophthalmic surgery.41,43,44
CLINICAL MANIFESTATIONS
The interval between ocular injury and the onset of sympathetic ophthalmia is important. It has been reported to be as short as 5 days11,45 or as long as 66 years.46,47 In general, 65% of sympathetic ophthalmia cases occur 2 weeks to 2 months after injury, and 90% occur before 1 year.1,11,48
The onset of the disease is insidious. The injured eye becomes painful and photophobic, and visual acuity is diminished. The noninjured (sympathetic) eye then follows a similar course. On ocular examination, the injured eye shows persistent low-grade uveitis despite the healing wound. Characteristic bilateral panuveitis is recognized by “mutton-fat” keratic precipitates, ciliary flush, aqueous cell and flare, posterior synechiae, vitreous cells and haze, choroidal thickening and infiltration, and optic nerve head edema. The presence of small, yellowish-white inflammatory infiltrates, 60 to 700 μm in diameter, at the level of the retinal pigment epithelium (Dalen-Fuchs nodules) but more commonly located at the midperiphery, is pathognomonic of sympathetic ophthalmia (Fig. 51-1). In severe cases, rubeosis iridis, cataracts, pupillary membrane formation, and exudative retinal detachment can occur. Chorioretinal scarring may eventually form, and the eyes may become phthisic.1,49,50,51
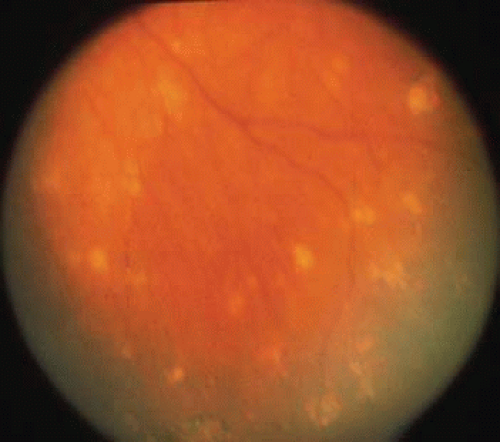 Figure 51-1. Multiple subretinal and choroidal infiltrates seen in the midperiphery of a patient with sympathetic ophthalmia. |
In some cases of sympathetic ophthalmia, the bilateral uveitis may be so mild or transient that the diagnosis is missed.1,49,52 Recently Gupta et al53 observed that 36 eyes with early stage of sympathetic ophthalmia presented posterior uveitis without anterior involvement in Northern India. Sympathetic ophthalmia can present as a mild, nongranulomatous uveitis that is easily misdiagnosed as idiopathic uveitis. This atypical clinical presentation may be due to early enucleation of the injured eye before the classic histopathology of sympathetic ophthalmia has appeared. Alternatively, the pathology may be modified by immunosuppressive treatment.52,54 In addition, progressive subretinal fibrosis with multifocal granulomatous chorioretinitis55 can occur in sympathetic ophthalmia.56 This rare entity is characterized by rapid vision loss with progressive subretinal fibrosis involving the macula.55 This form of the disease progresses rapidly and is often unresponsive to systemic immunosuppressive therapy.
Fluorescein angiography of patients with sympathetic ophthalmia often shows multiple areas of hyperfluorescence and leakage at the level of the retinal pigment epithelium (Dalen-Fuchs nodules) and the choroid (choroidal granuloma).48,49,50,57,58 If there is a serous retinal detachment, pooling of dye in the late frames of the angiogram can be observed.14,49,58,59,60 Although early hypofluorescence followed by late hyperfluorescence has been reported, this may indicate obliteration of the choriocapillaris and the presence of numerous Dalen-Fuchs nodules, as well as choroidal granulomas to obscure choroidal fluorescence in the early phase.14,50,60,61 Indocyanine green (ICG) angiography can reveal hypofluorescent patterns that persist throughout angiography or fade in the late phase that represent active or cicatricial lesions in the choroids.33,62,63,64,65
There may be a genetic component to disease susceptibility. With racially matched controls, HLA-DR4 and HLA-DRw53 were found to be highly associated with sympathetic ophthalmia in Japanese patients,66 whereas the occurrence of HLA-DR4 and DQw3 was reported significantly elevated in American patients with sympathetic ophthalmia.67 Using HLA serologic and polymerase chain reaction amplification (PCR)-based DNA typing in 16 Japanese patients and 50 controls, Shindo et al68 reported HLA-DRB1*04, DQA1*03, and DQB1 04 were significantly associated with sympathetic ophthalmia. Kilmartin et al69 also confirmed this genotype association (HLA-DRB1*04 and DQA1*03) in Caucasian patients with sympathetic ophthalmia. Recently cytokine gene polymorphisms, particularly interleukin-10 (IL-10)-1082A polymorphism, were found to be associated with severity of sympathetic ophthalmia.70,71
The differential diagnosis of sympathetic ophthalmia includes Vogt-Koyanagi-Harada syndrome, phacoanaphylactic uveitis, sarcoidosis, chronic idiopathic uveitis, and other granulomatous uveitis induced by mycobacteria or fungi.1,50,51 A history of ocular injury and a lack of systemic involvement or proven ocular infection, however, are helpful indicators in diagnosing sympathetic ophthalmia. Vitiligo, poliosis, alopecia, dysacusis, and meningeal irritation, findings more commonly reported in Vogt-Koyanagi-Harada syndrome, may be noted rarely in sympathetic ophthalmia.1,49,72 Blodi73 and Lubin et al11 reported sympathetic ophthalmia in 23% of 170 and in 46% of 105 cases of lens-induced endophthalmitis, respectively; in the latter study, of 31 cases of lens-induced endophthalmitis occurring after 1950, there was only one case of sympathetic ophthalmia. In reviewing 100 cases of sympathetic ophthalmia from the Armed Force Institute of Pathology (AFIP) file, Croxatto et al74 found 14 cases (22% of the 46 eyes enucleated before 1950, in contrast to 7% of the 54 eyes enucleated after 1950) associated with phacoanaphylactic endophthalmitis; the occurrence of sympathetic ophthalmia was unrelated to the severity of the choroidal inflammation.
The more severe the inflammation, the worse the prognosis of sympathetic ophthalmia. The sooner the diagnosis and more intensive the therapy, the better the outlook.23,42,75,76 In their study of 105 cases, Lubin et al11 found that 93.3% of the patients with mild inflammation had 20/70 (6/21) vision or better (the metric equivalent is given in parentheses after the Snellen notation); 100% of patients with severely inflamed eyes had 20/70 vision or worse. In a study with long-term follow-up data (mean follow-up of 23 years), Makley and Azar75 demonstrated ocular complication in 70% of patients. In this study, only 65% of the 17 patients treated with corticosteroids attained a visual acuity of 20/60 (6/18) or better. In a study at Moorfield Hospital, a visual acuity of between 20/20 and 20/60 was achieved in 14 of 18 patients (77%).76 In a study of 85 patients with sympathetic ophthalmia in three academic tertiary uveitis clinics from 1976 to 2006, Galor et al77 reported the ocular complications most often associated with decreased vision were cataracts and optic nerve abnormality. Exudative retinal detachment and active intraocular inflammation were significantly associated with poorer visual acuity in the sympathizing eye. Chan et al42 reported on 32 sympathetic ophthalmia patients from 1982 to 1992: 16 patients had a final visual acuity of 20/40 or better, and 10 had a visual acuity worse than 20/200. The remaining 6 patients had visual acuity ranging from 20/40 to 20/200. In this series and other subsequent studies, prompt and aggressive application of anti-inflammatory therapy was the key to achieving better visual outcome.40,42,78
HISTOPATHOLOGY
The classic histopathologic features of sympathetic ophthalmia were first described by Fuchs in 1905,3 confirmed by Easom and Zimmerman,79 and summarized by Green.80 Both the injured and the sympathetic eyes show similar histopathologic features. The main feature of sympathetic ophthalmia is a diffuse, nonnecrotizing, granulomatous inflammation in the uvea. The choroid is markedly thickened and infiltrated by lymphocytes and nests of macrophages, epithelioid cells, and giant cells. Other classic histopathologic findings include a relative lack of retinal involvement, sparing of the choriocapillaris, and the formation of Dalen-Fuchs nodules, consisting mainly of epithelioid cells located between the Bruch membrane and the retinal pigment epithelium (Fig. 51-2). Fuchs3 found that approximately 25% of his classic cases of sympathetic ophthalmia had Dalen-Fuchs nodules.
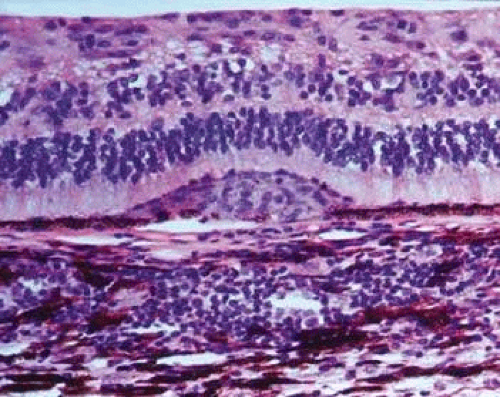 Figure 51-2. Microphotograph of Dalen-Fuchs nodule composed of mainly epithelioid histiocytes (macrophages) and a few degenerative pigment epithelial cells between the retinal pigment epithelial cell layer and Bruch membrane. |
Lubin et al11 reported that more than one nodule was present in 33 of 93 cases (35.5%). Kuo et al81 observed Dalen-Fuchs nodules in all 50 Chinese patients with severe sympathetic ophthalmia. Nine of 29 patients (31%) had Dalen-Fuchs nodules in an AFIP series.82 Breaks in the Bruch membrane at the site of Dalen-Fuchs nodules also have been identified.60,83
Many other histopathologic features of sympathetic ophthalmia have been reported in the literature. Retinal involvement (e.g., retinal perivasculitis, retinitis, retinal gliosis) has been documented in 30% of cases of sympathetic ophthalmia by Winter,23 in 42.2% by Lubin et al,11 and in 55% by Croxatto et al.74 Other features include choriocapillaris obliteration, reported in 40% of cases by Croxatto et al74 and in 52% by Kuo et al;81 chorioretinal scarring was reported in 7% of cases by Croxatto et al74 and in 25% by Makley and Azar.75 Lubin et al11 found optic atrophy in 54.4% of sympathetic ophthalmia cases. Nongranulomatous inflammation and focal inflammation can also be observed in sympathetic ophthalmia. In the 29 AFIP cases of sympathetic ophthalmia, 11 did not have granulomatous inflammation and 13 presented with only focal choroidal inflammation.82 Eosinophils and plasma cells were more commonly seen in the non–corticosteroid-treated and more severely inflamed cases.
Marak et al84 observed histologic variations related to race in sympathetic ophthalmia (SO). They found thickened choroid, an increase in the number and size of choroidal granulomas, and eosinophilia more commonly among African American patients than among white American patients. Kuo et al81 did not find any significant histopathologic differences between Chinese patients and white American patients. The finding of Marak et al84 may reflect the fact that the cases in the African American group were more severe at the time of diagnosis.
As stated previously, there is a rare form of SO characterized by a progressive subretinal fibrosis with multifocal granulomatous chorioretinitis leading to rapid vision loss.55 Histopathologic findings include multifocal granulomatous inflammation involving the outer retina and choroid with giant cells distributed along the Bruch membrane.56 In this variant, serum antibodies against photoreceptor and retinal pigment epithelium can be detected.
Immunohistopathologic studies of sympathetic ophthalmia show that choroidal infiltrates are composed predominantly of T lymphocytes.19,83,85,86,87,88 We have demonstrated a greater number of CD4+ T cells (T helper/inducer cells) in the early stages of the disease and CD8+ T cells (T suppressor/cytotoxic cells) in the late stages of the disease.83 In contrast, B-cells are found in less than 5%19,85,86,88 to 15%19,83 of choroidal infiltrates; however, higher percentages of B cells were found in 4 of the 29 AFIP eyes at the end stage of the disease.82 Formation of a pseudogerminal center with an aggregate of B cells surrounded by T cells is found in the variant of sympathetic ophthalmia with progressive subretinal fibrosis and blindness associated with multifocal granulomatous chorioretinitis.89
The main cellular components of both choroidal granuloma and Dalen-Fuchs nodules are bone marrow–derived monocytic (histocytic) cells. The granulomas of sympathetic ophthalmia have immunohistochemical staining profiles that are similar to the granulomas of sarcoidosis.90 In the late stage of sympathetic ophthalmia, however, degenerated retinal pigment epithelium can be an important component of Dalen-Fuchs nodules.91 Despite the accumulation of T lymphocytes in eyes with sympathetic ophthalmia, there is no reported difference in the lymphocytic subpopulations in the peripheral blood of patients with sympathetic ophthalmia, with the exception of one atypical case reported by Kaplan et al.88
Expressions of cell adhesion molecules and major histocompatibility (MHC) class II antigens on the ocular resident cells have been observed in eyes with sympathetic ophthalmia and may be important in the pathogenesis of the disease.19,92,93 Expression of various inflammatory mediators such as inducible nitric oxide, cytokines (e.g., tumor necrosis factor-alpha and interleukine-1), and chemokines are also illustrated in the eyes of sympathetic ophthalmia.94,95,96
PATHOGENESIS
The etiology of sympathetic ophthalmia is still an enigma. Two hypotheses dominate the older literature: autoimmunity against uveal melanin, uveal melanocytes, retinal pigment epithelium, or retinal antigens; or a viral or bacterial infection.1 Later studies have emphasized immune system involvement in patients with ocular inflammation.50 In 1971, investigators reported that lymphocytes from patients with sympathetic ophthalmia might respond to heterogeneous or homogeneous retinal and uveal tissues.97,98,99 Using lymphocyte transformation and a leukocyte migration inhibition assay, Rahi et al52 reported that cells from 5 of 6 patients with sympathetic ophthalmia showed positive reactions to uveoretinal tissues, whereas 7 of 10 cases of posttraumatic nongranulomatous uveitis showed negative responses to uveoretinal antigen. These observations suggested that cell-mediated hypersensitivity could be an important pathogenic mechanism. The immunohistopathologic finding of the predominantly T-lymphocytic infiltration in ocular tissue supports a cell-mediated immunologic response (delayed hypersensitivity) to ocular antigens in both typical and atypical cases of sympathetic ophthalmia.19,86,87,88,100,101
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


