Complications of Contact Lenses
Erich B. Groos Jr.
Bernard H. Chang
Contact lenses are visual prostheses worn for the purpose of correcting refractive error. Most contact lenses are worn for cosmetic and functional reasons by those who prefer them to spectacle correction. Patients approach the wear and care of contact lenses with varying degrees of discipline. Complications suffered by contact lens wearers can commonly be attributed to poor lens hygiene or overwear, poor lens fit, or underlying ocular pathology. Management of the latter two risk factors is to some extent under the control of the physician who fits lenses, but day-to-day maintenance remains the responsibility of the patient. Educating and monitoring each patient for appropriate lens wear and care requires substantial time and effort, but unfortunately, directions for appropriate lens management are frequently ignored.1,2,3,4,5 Patients with higher levels of ametropia tend to be more dependent on contact lens correction and are thus more likely to push the limits of safe contact lens wear.5 More often than not, experienced contact lens wearers become less fastidious over time and gradually abandon basic principles of lens cleaning and disinfection.1
As contact lens use has become more prevalent in the ametropic population, the prevalence of complications as a proportion of emergency eye care visits has increased; yet the overall prevalence of contact lens–related visits remains less than 5%.6,7,8 An eye care specialist who encounters a contact lens wearer with contact lens intolerance must recognize the signs of contact lens–related ocular disease and identify the appropriate cause. Bruce and Brennan9 present a thorough and thoughtful analysis of corneal pathophysiology as it relates to contact lens wear. They separate the forces that cause corneal disease in contact lens wear into four major categories:
Hypoxia and hypercapnia
Allergy and toxicity
Mechanical effects
Osmotic effects
Of these four, the first two account for most complications encountered in practice.
This chapter contains a review of the complications of contact lens wear in the order in which one might encounter them in the course of an organized examination of a patient. Defective contact lenses may affect vision unrelated to any complication. The eyelids are rarely the site of complications and may show meibomian gland dysfunction, blepharoptosis, or upper eyelid masses. The conjunctival surface is the frequent victim of contact lenses and the solutions necessary for their care. Inflammation secondary to toxicity or allergy occurs in the form of follicular conjunctivitis, giant papillary conjunctivitis, superior limbic keratoconjunctivitis, and other rarer conditions. Chronic inflammation may cause concretions or dry eye. The cornea, on which the contact lens floats, is the ocular structure most commonly affected adversely by contact lenses. Epithelial alterations include physical damage, vascularization, edema, cysts, and hypoesthesia. Corneal stroma may show edema, infiltrates, vascularization, opacities, infectious keratitis, or ectasia. Endothelial cells may be affected by long-term contact lens wear by forming blebs or exhibiting polymegathism. Finally, there are a few rare intraocular complications associated with contact lens wear that may not owe their cause to lens wear alone.
CONTACT LENS FORCES
Hypoxia and Hypercapnia
Because it is avascular, the cornea relies on gas exchange at the tear–air interface for successful aerobic metabolism. The threshold among individual eyes to suffer hypoxic complications varies widely.10,11 Eye closure and contact lens wear decrease the exchange of oxygen and carbon dioxide at the corneal surface. Oxygen transmissibility (Dk/L), which is lens material permeability (Dk) divided by lens thickness (L), is the most important variable when determining relative oxygen delivery to the corneal surface through a contact lens.12,13 The exchange of tears under the contact lens also influences corneal oxygen tension. Small-diameter rigid lenses of the same or lower oxygen transmissibility may result in less corneal edema than larger-diameter soft lenses because of superior tear exchange.13,14 Hypoxia and hypercapnia are less severe in the deep stroma and endothelium, which may obtain oxygen from and discharge carbon dioxide into the aqueous humor.15,16 It is estimated that a Dk of 300 would be required to prevent acidosis from anaerobic metabolism of the corneal epithelium but a Dk of only 18 would be required to do the same for the aqueous.16
In the absence of adequate oxygenation, the corneal epithelial mitotic rate decreases, causing decreased thickness, microcysts, and increased fragility.9 The compromise in junctional integrity of epithelial cells that ensues leads to punctate epithelial keratopathy, epithelial abrasions, and increased risk of microbial keratitis. Stromal lactate accumulation from anaerobic metabolism causes increased stromal thickness and disruption of the regular pattern of collagen lamellae leading to striae, posterior stromal folds, and increased light backscattering. Acidosis also increases corneal oxygen requirements, thereby exacerbating corneal hypoxia.17 Long-term stromal hypoxia and hypercapnia create stromal acidosis, which, in the short term, will elicit endothelial edema and blebs and, over many years, endothelial cell polymegathism. Further effects of hypoxia are corneal hypoesthesia and neovascularization of both the epithelium and stroma. Stromal vascularization may evolve to interstitial keratitis, deep opacities, or rarely intrastromal hemorrhage. In some cases of long-term wear, the cornea becomes accustomed to the new oxygen tension, and stromal edema is replaced by stromal thinning.
Allergy and Toxicity
A spectrum of ocular disorders that are allergic in etiology predispose to contact lens intolerance in certain individuals. Allergic rhinitis and conjunctivitis are risk factors for poor contact lens tolerance.18 The contact lens wearer faces various potential allergens. Contact lenses also encourage adhesion of debris, which remains in contact with ocular tissues and prolongs the exposure to allergens. Contact lens solutions and, in particular, the preservatives within them induce allergic responses in susceptible individuals.19 Thimerosal hypersensitivity may cause conjunctivitis, corneal epithelial infiltrates, and superior limbic keratoconjunctivitis.9 Reaction to protein deposits on contact lenses may produce giant papillary conjunctivitis resembling that with exposed sutures.19 The toxicity induced by an immobile contact lens is related to the rapid accumulation of metabolic by-products in the anterior corneal layers, which may result in limbal hyperemia, peripheral corneal infiltrates, and keratitic precipitates.9 Further surface damage may be the result of solution toxicity causing various patterns of punctate epithelial keratopathy. A combination of chronic chemical and mechanical forces may rarely lead to persistent epitheliopathy that mimics partial limbal stem cell deficiency or dysplasia.
Mechanical Effects
Mechanical effects inducing complications in contact lens wearers may include injuries sustained by improper placement or removal of a lens or those related to contact lens fitting and wear. Steep-fitting rigid lenses may induce corneal distortion or leave a surface imprint. In severe cases the corneal surface becomes warped. Tight-fitting soft lenses may induce surface wrinkling. Epithelial damage may occur because of debris trapped below the lens. This complication is particularly important considering the preponderance of female cosmetic contact lens wearers.7
Osmotic Effects
Contact lenses increase tear evaporation and decrease reflex tearing, thereby promoting the development of punctate epithelial keratopathy. Surface desiccation impairs ocular lubrication by the tear film, putting the epithelium at risk for mechanical injuries such as abrasions and erosions.
COMPLICATIONS BY LENS TYPE
Choosing the appropriate contact lens type for a particular patient requires careful consideration of refractive error, corneal shape, pre-existing ocular disease, and patient preference. The relative risks for complications of soft and rigid lenses using both extended and daily wear routines are important in the decision process. Rigid lenses, with the exception of hybrid and scleral lenses, are associated with fewer overall complications than soft lenses.6,20 Because rigid lenses have a significant adjustment period, failures within the first 6 months are approximately equal for both rigid and soft lenses.21 Risk for complications is directly proportional to the length of uninterrupted wearing time for any type lens.6,21,22,23,24,25,26,27,28,29 Extended wear lenses are associated with the highest relative risk for all complications except corneal abrasion, which occurs more frequently in the rigid lens population.6,30 Newer silicone polymers with high Dk seem to have reduced, but not eliminated, the complications of extended contact lens wear.21,22,23,24,25,26 Daily disposable soft lens wear appears to provide the greatest safety.30,31,32,33,34
Contact Lens Defects
Rigid contact lenses may break or chip to produce punctate epithelial keratopathy, corneal erosions, or corneal abrasions. A warped lens may cause corneal warpage or keratoconus.35 Lens deposits may accumulate, inducing focal inflammation and rarely giant papillary conjunctivitis.36 Despite tearing with relative ease, soft contact lenses wreak much less epithelial damage than nicked or broken rigid lenses.30 Hydrogel lenses attract much more protein deposition, making them more antigenically potent. A comprehensive review of soft lens defects is beyond the scope of this chapter but can be found elsewhere.37
Rigid Lenses
Rigid contact lenses of both the gas-permeable and polymethylmethacrylate (PMMA) type are effective lenses for the correction of astigmatic ametropia. These lenses deliver better image clarity than soft hydrogel lenses, but their use is limited by the high early dropout rate secondary to discomfort.21 Rigid lenses accumulate less protein and are thus less prone to induce allergic complications. Rigid lenses as a group are associated with fewer severe complications overall than soft lenses.6,7,20 The difference in the rate of infectious keratitis is even greater.20 The exceptions to this difference are scleral lenses and hybrid soft/hard lenses designed for use in high-risk eyes. Extended wear of rigid contact lenses, though encouraging because of their favorable oxygen transmissibility, has been limited by the significant prevalence of lens adherence to the cornea with overnight wear.38,39 Recent developments in rigid lens materials with high Dks and advanced designs have fueled the resurgence of orthokeratology. The short-term safety of this method for corneal flattening has been established, but the continued risk for corneal warpage, infectious keratitis, lens binding, central island formation, and erosion remains to be defined.
Daily Wear Soft Lenses
Wearing soft contact lenses on a daily basis is a popular method for correction of refractive errors. These lenses present a small relative risk of nonulcerative complications compared to rigid lenses and a lower risk than extended wear lenses.6 Compared to disposable daily wear lenses, conventional daily wear lenses have a higher rate of complications, excluding ulcerative keratitis, the rate for which is the same for both groups.40 The prevalence of ulcerative keratitis for daily soft lens wear is lower than that for any type of soft extended wear lens and higher than that for daily wear rigid lenses.20,41 Daily disposable soft lenses afford the lowest complication rate of any lens type.30,31,32,33,34 Planned replacement lenses (daily, weekly, and monthly) have largely supplanted yearly disposable daily soft lenses.
Extended Wear Soft Lenses
Continuous-wear soft contact lenses are ideal for patients with high refractive errors who wish to see at all times. These individuals are significantly handicapped without their spectacles, making even contact lens insertion difficult. This wearing regimen has become more popular for the general population of lens wearers because of the convenience afforded by minimal lens care requirements, particularly with disposable lenses.
Despite favorable early reviews, extended wear soft lenses have not become the panacea that was expected because of a higher incidence of ulcerative and nonulcerative complications compared to soft and rigid daily wear lenses.6,20,42 The safety of disposable extended wear lenses is better overall than for conventional extended wear, but the risk for infectious keratitis is the same.41 Sterile infiltrates occur more frequently with the disposable extended wear lenses.41 This higher risk for sterile keratitis may skew the results of some trials comparing rates of infectious keratitis for disposable versus conventional lenses. Because of chronic hypoxia related to extended lens wear, many extended wear lens failures are secondary to progressive superficial vascularization.43 Initial fitting with extended wear lenses that move well and have higher Dk/L values helps to decrease the number of potential failures.44 The availability of high Dk silicone polymer hydrogels has dramatically reduced but not eliminated the complications associated with extended lens wear.22,23,24,25
Aphakic Lenses
Contact lens correction of aphakia in both the geriatric and pediatric population may be limited by the difficulties of handling the lenses.45,46 Many elderly patients and parents of children lack the manual dexterity necessary to remove lenses on a daily basis. Extended wear soft lenses for aphakic correction, even with enhanced oxygen permeability, have limited transmissibility because of increased center thickness. Major complications observed include neovascularization, apical ulceration secondary to overwear, and infectious keratitis.45,46,47 Rigid daily wear lenses have a 10-fold reduced risk of infectious keratitis compared to soft extended wear in this population, but their use is curtailed by problems with handling, discomfort, and care.46 Coupled with the hypoxic stress on an already surgically compromised endothelium, these risks for many may make secondary intraocular lens implantation a more reasonable option. Improvements in lens implant design and safety of surgery have dramatically reduced the number of aphakic eyes over the last 20 years.
Therapeutic Lenses
Hydrogel contact lenses are useful in the treatment of various ocular surface disorders from dry eye to corneal perforation.48,49 The complications one encounters with these lenses are much the same as those with cosmetic extended wear lenses but occur with greater frequency because of an underlying disease process. One contact lens–related complication that may mimic more severe disease-related problems is the immobile lens syndrome.9 Though this syndrome may occur rarely in cosmetic extended soft lens wearers, it most often complicates therapeutic lens wear. As the name implies, the lens becomes immobile and traps debris against the cornea for an extended period of time. The resulting intense inflammatory reaction causes varying degrees of limbal hyperemia, peripheral corneal infiltration, and intraocular inflammation, including keratic precipitates and rarely hypopyon. This complication may be avoided by fitting lenses that move well and have high Dk values. If one uses a lens with high water content, assessment of lens movement within 24 hours is important because these lenses tend to shrink. Scleral lenses and hybrid lenses are newer products and designs that have become useful for advanced keratoconus and severe ocular surface disease. Complications with these lenses typically are the result of the underlying ocular pathology. It is important to consider therapeutic lens wearers separately when compiling data concerning contact lens complications because they may skew the results.
EYELID COMPLICATIONS
Meibomian Gland Dysfunction
Eyelid structures lie in direct apposition with contact lenses and exhibit varying degrees of inflammation, both clinical and subclinical. The meibomian glands are situated a fraction of a millimeter from the tarsal conjunctival surface and can be affected by chronic, low-grade mechanical and chemical irritation. Contact lens wearers show significantly more meibomian gland dysfunction than matched controls.50 Although this study was not masked, it supports some authorities’ theory that tear lipid abnormalities are an underrecognized cause of contact lens intolerance, particularly in veteran wearers. Meibomian gland dysfunction in a symptomatic contact lens patient with decreased tear breakup time should be treated with moist heat and, in severe cases, with topical azithromycin. Short-term use of mild topical corticosteroids is helpful in severe cases. In refractory cases, discontinuation of contact lens wear is necessary to break the cycle perpetuated by inflammation. Careful examination for and treatment of causes of periocular inflammation and changes in contact lens care may be required to prevent further exacerbation of the condition. The rapid accumulation of protein deposits in these patients may require a temporary shift to daily disposable lenses. Although meibomian gland dysfunction related to contact lens wear rarely progresses to visual loss, severe cases left untreated show progressive decrease in surface lubrication, leading to an increased risk of infectious keratitis and scarring.
Blepharoptosis
Long-term wear of rigid contact lenses has been reported to cause blepharoptosis in a wide age range of patients. In a two-pronged study, van den Bosch and Lemij51 describe seventeen patients with rigid contact lens–related ptosis. Two of these patients had unilateral ptosis that occurred on the side of rigid lens wear. One of the two wore a soft lens in the fellow, nonptotic eye. The second part of the study compares the margin reflex distance (MRD) of a group of long-term rigid lens wearers to that of an age-matched control group. The former group had a smaller MRD and more clinical diagnoses of ptosis than the control group. An earlier study describes the pathophysiology of contact lens–related ptosis as levator aponeurosis disinsertion.52
Upper Lid Mass
In rare cases rigid contact lenses that were thought to be lost migrate through the conjunctiva at the superior tarsal border of the upper eyelid to present many years later as an upper eyelid mass.53,54,55,56,57,58 A ring-shaped protrusion with a hole in the center located on the conjunctival side of a lid mass suggests the diagnosis.53 Histologic examination reveals a cystic cavity lined with epithelium, scar tissue, and chronic inflammation.54,55,56 The clinical presentation is that of an eyelid tumor or chalazion. In at least one case the contact lens presented spontaneously from the mass.55 Computed tomography scanning will not reveal the lens if present; therefore, one must inquire regarding a previously lost contact lens in these cases.57 The lens may also migrate into the orbit to cause an orbital mass.58 In one case the retained lens was the cause of a severe peripheral ulcerative keratitis.56 Of all reported cases, 21 lenses were found in the upper lid, 2 migrated into the orbit, and 2 extruded from the lid.58
CONJUNCTIVAL COMPLICATIONS
Conjunctival injection in a contact lens wearer often seems to be the norm rather than the exception. With all forces both mechanical and chemical conspiring to induce inflammation, it is surprising that the prevalence of severe conjunctival inflammation is not greater. In 1980, before the widespread use of hydrogel or gas-permeable contact lens materials, Korb et al.59 found a significantly higher prevalence of elevated papillae in long-term PMMA wearers than in a large control group. Considering that a soft contact lens behaves like a small sponge, it is not surprising that a soft contact lens wearer is five times more likely than a rigid lens wearer to present with a hypersensitivity or toxicity-related disorder.6 Hypersensitivity and toxicity accounted for 387 out of 1,104 (35%) emergency admissions to a tertiary eye hospital with contact lens–related problems.6 Of that number approximately two-thirds were conjunctivitis.
Mucus Formation
Continuous friction and chemical forces of contact lenses on the conjunctival surface promote the formation of mucus in quantities higher than in those who do not wear lenses. On a microscopic level the number of goblet cells is increased over that of normal controls.60 The number of nongoblet cells lining the epithelium that contain mucous vesicles is increased in contact lens wearers relative to normal controls.60 Only in rare cases does overproduction of mucus result in loss of the ability to wear contact lenses.
Dry Eye
As discussed previously, contact lenses have been associated with an increased risk of meibomian gland dysfunction and the attendant decrease in tear surface integrity. In addition to a loss of surface lubrication, the loss of lipid layer integrity allows increased aqueous evaporation; a process further accelerated by contact lenses, particularly those with high water content. The hydration required by these lenses absorbs water from the surrounding tear lake. Hydrogel lenses and, to a greater extent, rigid lenses cause corneal hypoesthesia, which decreases basal and reflex tear secretion.61 The combination of lipid, aqueous, and mucin abnormalities caused by contact lens wear puts the wearer at higher risk for dry eye.62 Treatment should be directed toward symptomatic patients with regard to specific abnormalities identified on careful examination. In most cases, dry eye is multifactorial and may not respond to artificial tear therapy alone. Contact lens cessation will often allow more rapid resolution of dry eye symptoms. Once discontinued, lenses may then be worn with protective measures prescribed to decrease recurrences.
Concretions
Chronic contact lens wear in the presence of significant daily exposure to particulate matter promotes the phagocytosis of particles by cells of the conjunctival epithelium, primarily in the inferior fornix. Contact lens wearers in industrial situations, where there is significant dust exposure, and those who wear makeup that spills into the tear lake daily are at risk of developing concretions. In most instances concretions are benign, but the engulfed material may erode through to irritate the ocular surface. Concretions that stain with fluorescein after 5 minutes in a symptomatic patient may be removed under topical anesthesia.
Toxic Conjunctivitis
Toxicity of various contact lens–related chemicals to the ocular surface causes bulbar conjunctival injection and papillary conjunctivitis in the fornices, usually more pronounced inferiorly. Also known as contact irritation, this reaction is dose dependent and is exacerbated by the fact that contact lenses slow clearance of the inciting agent.19 Most commonly, this reaction occurs when a contact lens wearer breaches protocol by not rinsing hydrogel lenses sufficiently after disinfection or enzyme treatment. The patient may also neglect hand washing after exposure to any number of household chemicals before handling the lenses. These reactions will respond quickly to discontinuing lens wear and avoiding the inciting agent. Cool compresses and preservative-free artificial tears will provide symptomatic relief during recovery. Severe cases may require a short course of corticosteroid drops, though some authorities observe that treatment fails to hasten resolution of the inflammation. If the wearer has “sensitive” eyes, conjunctivitis may occur because of preservatives in contact lens solutions. Changing to hypoallergenic care solutions and preservative-free saline for storage will often eliminate this reaction. The use of daily disposable soft lenses will limit exposure to the chemicals of routine lens care as well. In these situations it is often prudent to recommend the use of heat disinfection because it is superior to the hypoallergenic chemical disinfectants, particularly against Acanthamoeba. Reinforcing the basic elements of proper contact lens care is always important.
Allergic Conjunctivitis
Generally, allergic conjunctivitis secondary to contact lens wear may be distinguished from contact irritation by the presence of severe itching and swelling. In both situations, the ocular findings of diffuse papillary conjunctivitis are indistinguishable. True contact allergy may be proven by skin-testing potential allergens for characteristic delayed erythema and induration associated with cell-mediated immunity. An inciting hapten may be environmental, in which case the contact lens presents the hapten in concentrated form to an already inflamed conjunctiva. Certain contact lens solution components, particularly preservatives such as thimerosal, have been implicated as allergens. Patients with ocular irritation in the presence of thimerosal-preserved solutions have a high rate of positive skin patch tests to thimerosal.63 One may minimize the prevalence of allergic contact lens disorders by carefully screening patients for nonocular allergic symptoms and conditions.18
Allergic conjunctivitis must be distinguished from hay fever conjunctivitis, perennial allergic conjunctivitis, atopic keratoconjunctivitis, vernal conjunctivitis, and giant papillary conjunctivitis by careful history and ocular examination.19 Once the diagnosis has been made, identifying the inciting hapten allows effective counseling for avoidance. Changing to less allergenic solutions may be necessary in the absence of an identifiable allergen. Symptomatic treatment is the same as that for toxic conjunctivitis. Control of itching may be accomplished by using topical vasoconstrictors and antihistamines during the acute phase. Topical ketorolac (Acular) has been effective for the symptomatic relief of itching but does not improve local tissue engorgement as well as topical vasoconstrictors. Oral antihistamines and rarely topical corticosteroids may be needed for severe cases. Topical cromolyn sodium (4%) may be used for chronic recurrent cases but has largely been supplanted by Pataday, Bepreve, and Elestat.
Giant Papillary Conjunctivitis
Giant papillary conjunctivitis (GPC) takes its name from the large papillae that form on the upper tarsal conjunctiva in response to contact lens wear or the chronic presence of other ocular foreign bodies.64,65 No contact lens type has escaped association with this complication.41,60,66 The classic triad of pruritus, excess mucus, and contact lens intolerance coupled with giant papillae of the upper tarsal conjunctiva make the diagnosis (Fig. 27-1).59 As the disease process progresses, the conjunctiva coalesces and the papillae become flattened. Ptosis may also develop. The condition must be differentiated from vernal keratoconjunctivitis because both have similar clinical features.19 Vernal keratoconjunctivitis occurs in warm weather, in adolescent males, and in the absence of contact lens wear.19 Those with seasonal allergies are more likely to develop GPC with contact lens wear.65,67
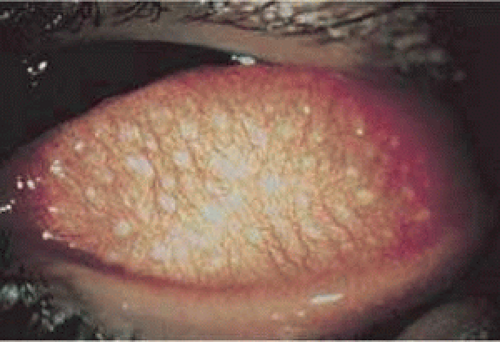 Figure 27-1. Giant papillary conjunctivitis. |
The pathophysiology of GPC is believed to involve conjunctival reaction to protein deposits on the lens surface, but mechanical trauma may also contribute.64 The immunologic reaction in GPC is similar to that found in vernal keratoconjunctivitis, but tear histamine levels are significantly greater for vernal.68 Tear IgE levels are also elevated in GPC patients relative to disease-free contact lens–wearing controls.69
Rigid lens wearers are less likely than hydrogel lens wearers to develop GPC because they accumulate less protein and are more completely cleaned.36,65,66 Most PMMA lenses do not require enzyme cleaning, but gas-permeable lenses should be enzyme cleaned at least once per month if not more often. The enzyme that seems to create the least inflammation in these patients is papain.64 Heat disinfection is associated with an increased prevalence of protein deposition and should be replaced by cold disinfection, preferably a hydrogen peroxide system.37,64
Treatment consists of discontinuing lens wear and initiating pharmacologic therapy with topical cromolyn sodium (4%) four times per day.64,70,71 Because the commercial preparation has shown stability problems and is no longer available, the solution must be made fresh for each patient every month. Promising data on symptomatic improvement with topical nonsteroidal anti-inflammatory agents leave hope for a new commercial preparation for this condition.72 Newer mast cell stabilizers such as Pataday, Bepreve, and Elestat show promise for treating GPC but have not been widely tested.65 Topical corticosteroids are of little benefit in this disorder. Topical antihistamines and vasoconstrictors are valuable during the acute phase, which lasts 3 to 5 days in the absence of contact lenses. After resolution of itching, hyperemia, and mucus production, contact lenses may be refit and mast cell stabilizers used with them in place.64,65 Rigid gas-permeable lenses have often been recommended to replace hydrogel lenses because of their tendency to bind less protein.64,65 Others recommend new, clean soft lens use with reinforcement of appropriate lens care and frequent replacement or the daily use of a disposable soft lens.73,74 Chronic recurrent GPC requires permanent cessation of lens wear but is becoming rarer with frequent lens replacement strategies.
Contact Lens–Related Superior Limbic Keratoconjunctivitis
Contact lens–related superior limbic keratoconjunctivitis (CL-SLK) is a condition characterized by superior bulbar conjunctival inflammation, redundancy, and thickening associated with irregular superior corneal epithelium and an underlying V-shaped, faint, subepithelial, corneal opacity extending toward the center of the cornea. The condition is usually bilateral and symmetric. In non–contact lens wearers with SLK, hydrogel contact lens wear may be therapeutic. CL-SLK may be distinguished from its de novo counterpart by the pattern of punctate epithelial keratopathy (PEK) associated with each. A contact lens wearer develops PEK superiorly and extending down the peripheral cornea to the inferior one third, whereas the other form of SLK has PEK limited to the superior pole of the corneal epithelium. Contact lens wearers who develop this condition are often rigid lens wearers who switched to soft lenses or soft lens wearers who switched from heat disinfection to chemical.75 In each case preservative exposure is the presumptive cause, and a significant percentage show hypersensitivity to thimerosal.75,76 Most patients improve to baseline without lens wear over periods ranging from 1 week to 1 year. Corticosteroids and other traditional pharmacologic agents used to treat immunologic ocular diseases are largely ineffective in this condition. Topical cyclosporine (Restasis) is a good alternative for the treatment of these patients. Some patients may return to lens wear using preservative-free solutions and heat disinfection.75
Pyogenic Granuloma
Pyogenic granuloma is rarely associated with contact lens wear. Two cases have been reported in which daily and extended lens wear is associated with formation of a pyogenic granuloma.77,78 Both patients underwent excision of the mass with pathologic diagnosis. One lesion showed numerous foreign bodies embedded in the center.78 Follow-up information was available on one person only, who was able to return to lens wear by switching to rigid gas-permeable lenses.77
CORNEAL COMPLICATIONS BY LAYER PRIMARILY AFFECTED
Epithelium
The corneal epithelium bears the brunt of mechanical trauma and chemical alterations meted out during contact lens wear. Hypoxia is emerging as a major force in corneal epithelial damage not explainable by direct trauma related to lens defects or handling. Decreasing Dk in rigid lenses in an animal model increased the observed degree of corneal epithelial cell swelling and desquamation.79 Extended soft contact lens wear has been implicated in specular microscopic observations of enlarged surface epithelial cells, suggesting a slower turnover of cells under these conditions.80 Even scant concentrations of common contact lens disinfectants, which come into intimate contact with the epithelial surface on a daily basis in hydrogel lens wear, cause epithelial cell retraction and decreased mitotic activity.81 The spectrum of corneal epithelial injury secondary to contact lens wear extends from mild punctate epithelial keratopathy in specific patterns to severe ocular surface disorders with indolent ulceration, anterior stromal scarring, superficial vascularization, and decreased vision requiring surgical intervention.82 There has even been a report of intraepithelial neoplasia associated with contact lens wear in the setting of extensive acute ultraviolet radiation exposure.83 Because isolated trauma to the epithelium may lead to serious corneal scarring, persistent contact lens abuse may lead to visual loss requiring penetrating keratoplasty.84,85 With enough foresight most contact lens wearers may avoid this devastating result.
Punctate Epithelial Keratopathy
Punctate epithelial keratopathy (PEK)—often incorrectly referred to as superficial punctate keratitis (SPK)—may result secondary to trauma, hypoxia, drying, chemical toxicity, or any permutation of the previous list.9,86 Discontinuing lens wear, eliminating potentially toxic topical medications, and treating tear surface abnormalities are the mainstays of therapy for these findings. Specific changes in contact lens material, fit, care, or wearing time may be required to prevent recurrence.
Contact lens overwear produces a coarse central pattern of staining that is often associated with excessive rigid and soft contact lens wear as well as with flat-fitting rigid lenses.9 The severity of staining is proportional to the duration of contact lens abuse and will determine recovery time following discontinuing lens wear. Discontinuing extended wear, decreasing daily wear time, and refitting with steeper rigid lenses are all possible approaches to prevent recurrence.27 The presence of an arcuate patch of PEK near the superior limbus is suggestive of hypoxia secondary to a tight upper lid.9 This may be addressed by refitting with higher-Dk lenses or decreasing the duration of continuous lens wear. In rare cases the epitheliopathy may require months without lenses to effect resolution.
Contact lens–related superior limbic keratoconjunctivitis presents with additional signs and symptoms to accompany the irregular superior PEK that develops in non–contact lens–related SLK.9,75,76 The diagnosis and treatment of this condition have been discussed previously under conjunctival complications.
Corneal PEK secondary to solution toxicity commonly presents as a diffuse pattern of superficial punctate fluorescein staining involving the entire corneal surface, often including the limbal conjunctival surface as well.9 Patients complain that the lenses sting immediately on insertion. Review of lens care protocol, particularly when using hydrogen peroxide disinfection systems, is critical to eradicate this complication. Hand washing should be doubly stressed. Severe PEK may evolve to a vortex pattern suggesting more profound epithelial toxicity and rarely limbal stem cell deficiency or neurotrophic keratitis. In its most severe form the PEK may become dendriform.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


