Fig. 4.1
Classification of swellings of the jaw according to origin
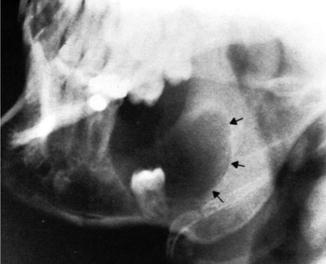
Fig. 4.2
Plain X-ray showing a smooth, well-circumscribed lucent cavity (black arrows) containing the crown of an unerupted tooth, characteristic of dentigerous cyst
Swellings arising from the mucoperiosteum (epulides)
Swellings arising from tissues responsible for development of teeth (odontomas)
Swellings arising from non-odontogenic cell remnants (developmental cysts)
Swellings arising from the bone proper (bony swellings)
4.3 Epulides
Swellings arising from the mucoperiosteum (gums) are known as “epulides” (any solid swelling situated in the gums).
4.3.1 Fibrous Epulides
Fibrous epulides arise from the peridental membrane (mucoperiosteum) surrounding the teeth and present under the gums. It forms a tumor that simulates a “fibroma.” It is the most common form and usually lies between the incisor teeth of the lower jaw. It usually affects middle-aged individuals with a female to male ratio of approximately 3:1.
The swelling is sessile at the beginning and then becomes pedunculated. It is whitish in color due to diminished vascularity, firm in consistency, and covered by intact mucosa. Treatment is by excision.
Other forms:
Fibroangiomatous form: It bleeds easily on touch.
Fibrosarcomatous form: It results from malignant transformation.
Congenital epulides: It occurs since birth, varies from a few millimeters to 9 cm in diameter, and may interfere with feeding or respiration [3].
4.3.2 Myelomatous Epulides (Giant Cell Epulides)
Myelomatous epulides arise from the osteoblastic layer of the periosteum or from the alveolus itself. It contains osteoclasts and is considered an osteoclastoma of the alveolar margin. It is divided by septa into lobules and contains osteoclasts, giant cells, spindle cells, and fibroblasts. It usually affects patients between 30 and 40 years, but can occur at any age.
The swelling is most commonly situated peripherally, in the mandible or maxilla. It presents as a sessile, lobulated, bulky, red mass, fixed to the underlying tissues and covered with intact mucosa, which bleeds on touch owing to its high vascularity. Though painless, it is rapidly growing and liable to necrosis, ulceration, cyst formation, and malignant transformation. A plain X-ray will show eating up of the jaw under the tumor. Treatment is by excision.
4.3.3 Granulomatous Epulides
A granulomatous epulide is a mass of granulation tissue formed around a carious tooth or gingivitis. It presents as a soft, red, lobulated mass that bleeds easily on touch. It is not covered with mucosa. It is treated by removal of the cause of irritation, extraction of the affected tooth, and the use of mouthwash and antibiotics, in addition to scraping away of the granulation tissue. If persistent, painting with 3–5 % silver nitrate or surgical excision may be resorted to.
4.3.4 Carcinomatous Epulides
Carcinomatous epulide is now considered as an “alveolar carcinoma” arising from the mucous membrane covering the gum (squamous epithelium). It is a rapidly growing mass with necrosis and ulceration. Characteristically, it does not give metastases, but gradually eats up the underlying bone. The patient usually presents with a painful, infected, fungating, or ulcerating mass that may invade the bone and spread to cervical lymph nodes (LNs). A biopsy is a must for diagnosis. Treatment usually involves a combination of surgical and radiotherapy (RT) according to full assessment and staging.
4.3.5 Sarcomatous Epulides
A sarcomatous epulide is actually covered by mucous membrane of the gum, but may develop from fibrous tissue. Males, of the middle age, are more affected than females. The patient usually presents with a sessile mass, which may be fixed to the underlying jaw. It may be hard, firm, or soft (denotes degeneration or high-grade malignancy). Ulceration and bleeding occur later. A plain X-ray may show bone infiltration. Treatment is accomplished by a wide excision with a safety margin of the underlying bone or hemimandibulectomy.
4.3.6 Epulides Associated with Pregnancy
It results from increased estrogen level during pregnancy and bad oral hygiene. It usually occurs in relation to the posterior teeth, especially the upper jaw. The patient presents with hypertrophy of the gums and a tendency to bleed. It is usually prevented with good oral hygiene during pregnancy.
4.4 Odontomas
An odontoma is a swelling derived from cellular elements that take part in the development of teeth. It is well-agreed upon that some epithelial cell residues persist throughout life in the gubernacular canals and periodontal membranes. These cells remain as inactive single or cluster cells that could be triggered resulting in the development of well-recognized pathological entities. The origin of epithelial odontogenic neoplasms, hamartomas, or cysts is thought to be related to such cell rests. The evidence is, however, based mainly on morphology and co-localization rather than on solid molecular evidence [2].
4.4.1 Dental (Radicular or Subapical) and Dentigerous (Follicular) Cysts
Both dental and dentigerous cysts show a slowly growing painless swelling, hard in consistency (covered by bone), expanding the bone internally and externally resulting in an “eggshell crackling sensation.” Table 4.1 summarizes the differences between both cysts.
Table 4.1
Differences between dental and dentigerous cysts
Point of difference | Dental (radicular) cyst | Dentigerous (follicular) cyst |
|---|---|---|
Cause | Irritation of the epithelial debris (of Malassez) by a chronically infected tooth usually incisor or canine | Irritation of the same epithelial debris by “unerupted” tooth, usually premolar tooth |
Site | Upper jaw > lower jaw | Lower jaw > upper jaw |
Age | Middle age (30–40 years) | Younger age (7–25 years) |
Pathology | Smaller in size | Larger in size |
Clear fluid inside rich in cholesterol | Viscid fluid inside + missed tooth | |
Overlying tooth is present | Overlying tooth is absent | |
Plain X-ray | Clear cavity with evident outline + cholesterol crystals | No cholesterol crystals |
No tooth inside the cavity | Tooth inside the cavity (Fig. 4.2) | |
Treatment | Extraction of affected tooth and opening the cavity (via intraoral approach) and removal of the epithelial lining, then obliteration of the cavity with soft tissue or bone chips | De-roofing of the cyst and removal of the epithelial lining. If the tooth is upright, it is left to erupt, but if not, it is removed. The cavity is then obliterated |
4.4.2 Ameloblastoma (Adamantinoma)
Ameloblastoma is an epithelial tumor that arises from ameloblasts (epithelial debris of Malassez), or it is a sort of basal cell carcinoma from the basal cells of the dental epithelium. It is reported to constitute about 1–3 % of tumors and cysts of the jaws and is known to be the most common tumor of the lower jaw in Egypt. Ameloblastoma affects the mandible more than the maxilla (5:1) particularly the angle of the mandible, but it can grow forward to the body of the mandible and/or upward to the ascending ramus.
Ameloblastoma occurs most commonly in adults (30–40 years), but may occur at a younger age. The patient presents with a chronic painless jaw swelling, which is characteristically well defined, lobulated, and expanding the jaw externally rather than internally. There may be ulceration of the mucous membrane and loosening of the overlying tooth or teeth. It is usually hard in consistency, but may have an “eggshell” crackling sensation due to degeneration.
Plain X-ray will show fine “soap and bubble” or “honeycomb” appearance (Fig. 4.3). Biopsy is essential for diagnosis. It should be differentiated from osteoclastoma (has fine and coarse soap and bubble appearance on plain radiography). Complications include ulceration, loosening of teeth, pathological fracture, and recurrence after removal.

Fig. 4.3
Ameloblastoma. Note multi-locularity of the lesion (fine soap and bubble or honeycomb appearance), the well-defined margins (large arrows), and resorption of tooth root (small arrows)
Treatment varies from simple enucleation with curettage to wide local resection of the mandible (or maxilla) with reconstruction (Fig. 4.4). A radical approach should be adopted whenever possible as the conservative approach results in a significantly higher rate of recurrence than the radical approaches [4].

Fig. 4.4
A “3D” reconstructed CT image of the resultant defect after resection of a recurrent ameloblastoma requiring bone grafting
4.5 Bony Swellings
Bony swellings affecting the jaw are classified mainly into inflammatory and neoplastic swellings; the latter may be benign or malignant, either primary or metastatic (Table 4.2).
Table 4.2
Classification of bony jaw swellings, according to pathology
Inflammatory | Neoplastic | ||
|---|---|---|---|
Benign tumors (BTs) | Malignant tumors (MTs) | ||
Primary MTs | Secondary MTs | ||
Dental granuloma | Osteoma | Carcinoma: (adenocarcinoma, squamous cell carcinoma, lymphoepithelioma) | From cancer of: Thyroid Breast Suprarenal glands Kidneys Prostate |
Alveolar Abscess | Chondroma | Sarcoma: (Osteogenic sarcoma, chondrosarcoma, fibrosarcoma, Ewing’s sarcoma, etc.) | |
Osteomyelitis (specific, nonspecific) | Paget’s disease | Lymphoma (Burkitt’s) | |
Actinomycosis | Hyperparathyroidism | Osteoclastoma | |
Benign fibro-osseous lesions (fibrous dysplasia – cementoma) | Multiple myeloma | ||
4.5.1 Inflammatory Lesions
4.5.1.1 Dental Granuloma
It may occur in the form of a giant cell granuloma, which represents a failure of an attempt at repair of a hematoma of the jaw. It affects females more than males, usually below the age of 20 years. A plain X-ray (occlusal view) will demonstrate an expansile radiolucency in the anterior portion of the mandible producing even, regular swelling of the buccal cortical plate (arrows) and intrusion of a canine tooth (C) (Fig. 4.5).
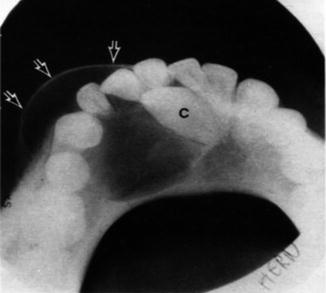
Fig. 4.5
Giant cell granuloma
4.5.1.2 Alveolar (Dental) Abscess
It is an abscess that occurs in the socket of the tooth (alveolus). It can develop ant any age, with the first or second dentition. The patient presents with throbbing pain, painful swelling, and malaise, sweating, and anorexia. Physical examination reveals a hot, tender, reddish (hyperemic) swelling with an ill-defined edge. Large abscesses may fluctuate. The mass is clearly fixed to underlying bone. Upper cervical lymph nodes (LNs) are enlarged and tender.
4.5.1.3 Osteomyelitis
Osteomyelitis may be acute or chronic (specific due to tuberculosis, for example, or nonspecific from acute osteomyelitis, compound fracture of the jaw, blood-borne infection, or tumor infiltrating the jaw).
There may be history of tooth extraction. The patient presents with a painful, warm bony swelling with a nodular surface and a border that gradually merges into normal bone. Expansion may affect one side only or both. Physical examination reveals tenderness, redness, and hotness, with or without edema. Trismus may be present. Draining LNs are enlarged and painful. A sinus and/or abscess may be present. Delayed sequestrum formation and delayed healing may occur due to inadequate rest (continuous motility of the jaw) and recurrent infection from the mouth.
The lesion is usually difficult to heal. Treatment includes mouthwashes and appropriate antibiotics. If a sequestrum develops, sequestrectomy is performed via an incision along the lower border of the mandible. In case of abscess formation, incision and drainage is done.
4.5.1.4 Cervicofacial Actinomycosis
It usually affects adult males, most commonly at the angle of the jaw. The swelling is nodular, tender, warm, and fixed to the skin, with multiple sinuses discharging the diagnostic sulfur granules. Trismus is commonly present. It is sensitive to penicillin.
4.5.2 Neoplastic Lesions
4.5.2.1 Carcinoma of the Maxilla
Carcinoma of the maxilla arises from the “maxillary antrum,” which is pyramidal in shape. Its base is made by the lateral wall of the nose, apex by the zygomatic process of the maxilla, floor by the alveolar part of the maxilla, and roof by the floor of the orbit.
The pathological types include squamous cell carcinoma (SCC), adenocarcinoma, minor salivary gland tumor, and undifferentiated carcinoma. It spreads locally into all direction, by lymphatics to the upper deep cervical, retropharyngeal or submandibular LNs, and hematologically to the lungs, bone, brain.
The disease has a predilection for males with age range 38–89 years [5]. Diagnosis is usually made at a late stage where most of the patients have been long treated for sinusitis or blocked nose. The definitive presentation depends on the site and direction of growth of the tumor, as shown in Table 4.3.
Table 4.3
Clinical presentation of carcinoma of the maxilla
Tumor location | Clinical presentation |
|---|---|
Anterior and lateral wall | Swelling of the face and cheek |
Medial wall | Nasal obstruction, anosmia, epiphora (infiltration of the nasolacrimal duct) |
Posterior wall, nasopharynx | Dyspnea and change of voice |
Roof | Proptosis and diplopia |
Floor | Bulging of the hard palate |
It may present with pain in the region of the maxilla (referred to upper teeth) due to blockage and infection of the antrum and later due to involvement of branches of the trigeminal nerve. The primary tumor may be occult and present with enlarged LNs in the neck.
Plain radiography will show a soft tissue shadow in the antrum and signs of bone destruction. CT scan will delineate the anatomy and bony involvement, and biopsy is essential for definitive diagnosis. The optimum management includes surgery, radiation, and systemic and topical chemotherapy in a variety of combinations and sequences. Survival from carcinoma of the maxilla is poor where the local disease extent and nodal disease at presentation are the only variables independently associated with cause-specific survival [5].
4.5.2.2 Sarcoma of the Maxilla
Contrary to carcinoma, sarcoma of the maxilla affects a younger age group and females more than males. It has a shorter history with more pain, causes a worse general condition, and has a worse prognosis. Pathologically, it may be a spindle cell, osteogenic, or fibrosarcoma.
The patient usually presents with a painful swelling in the face and loosening of teeth. There may be blocking of the nose with epistaxis, fetor oris, and increased salivation. The skin overlying the swelling is usually stretched and glistening and shows dilated veins.
Plain radiography will show clouding of the sinuses and bone destruction, which is better delineated by CT scan. Metastatic workup should be performed due to early spread. For treatment, a combined therapy is usually required (surgery, chemotherapy, and radiotherapy).
4.5.2.3 Burkitt’s Lymphoma
Burkitt’s lymphoma of the head and neck region usually involves the cervical LNs. Primary involvement of the nasal cavity and paranasal sinuses is uncommon. In paranasal Burkitt’s lymphoma, the maxillary sinus is most commonly involved followed by the sphenoethmoidal sinuses [6].
Epstein-Barr (EB) virus is the most likely etiological factor. It occurs more commonly among children of the “Equatorial” regions of Africa between the ages of 2 and 14 years. The most common presentation (50 %) is that of a jaw swelling (osteolytic lesion of the maxilla or mandible). An abdominal tumor is the second most common presentation. Renal involvement is usually bilateral, and the nervous system may also be involved. In girls, involvement of the ovaries is characteristic. A plain X-ray or CT scan will show multiple osteolytic deposits with bone destruction. The tumor is sensitive to chemotherapy.
4.5.2.4 Osteoclastoma (Giant Cell Tumor)
It is a locally destructive tumor, which grows gradually with no metastases, and affects the mandible, but rarely the maxilla could be affected. It is similar to adamantinoma, with some differences highlighted in Table 4.4.
Table 4.4
Differences between ameloblastoma and osteoclastoma
Criteria | Ameloblastoma | Osteoclastoma |
|---|---|---|
Site of origin | Near the angle of the mandible | Near the symphysis menti |
Growth direction | Upward and forward and may cross the symphysis menti | Backward in the body of mandible, but never crosses the S. menti |
Age | Fourth and fifth decades | Adolescents or 20–40 years |
Sex | Females > males (9:1) | Males > females |
Shape of tumor | Lobulations (may be equal) | Variable lobulations (coarse and fine) |
Jaw expansion | External > internal | Equal on both sides |
Color | Pale or pink | Reddish or brownish |
Plain X-ray | Fine soap bubbles | Coarse and fine soap bubbles |
Special character | Radioresistant | Radiosensitive (postoperative RT) |
An osteoclastoma should be differentiated from ameloblastoma (refer to the table above) and other giant cell lesions, mainly:
Giant cell granuloma:
It represents a failure of an attempt at repair of a hematoma of the jaw. It affects females more than males, below the age of 20 years. Perforation of the cortex is very rare.
Brown tumor of hyperparathyroidism (HPT):
The jaw may be affected due to generalized bone affection (von Recklinghausen’s disease). The brown coloration is due to hemorrhage inside the lesion.
Complete surgical resection is required for adequate treatment as incomplete resection leads to recurrence in about 70 % of cases [7].
4.6 Reconstruction of the Mandible
Reconstructive surgery has started as early as 1600 BC. Egyptian surgical papyri have been found describing methods for repairing broken noses and fractured mandibles and providing instruction in suturing to minimize scarring. Written evidence cites reconstructive treatment for facial injuries more than 4,000 years ago, and the physicians in ancient India were utilizing skin grafts for reconstructive work as early as 800 BC. However, reconstructive surgery, like most of other medical specialties, has rapidly progressed in the nineteenth and twentieth centuries. War was the driving force behind most of the developments in reconstructive surgery during the late 1800s and early 1900s. During the First World War, the physicians were confronted with extensive facial and head injuries. Shattered jaws, blown-off noses and lips, and gaping skull wounds caused by modern weapons required innovative restorative procedures. In the 1940s, many plastic surgeons served their countries during the Second World War. They expanded their reconstructive procedures to treat extensively wounded soldiers, sailors, and airmen [8].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


