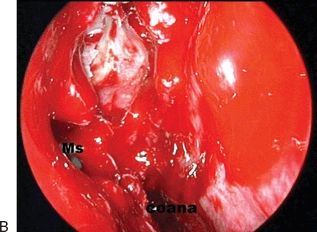
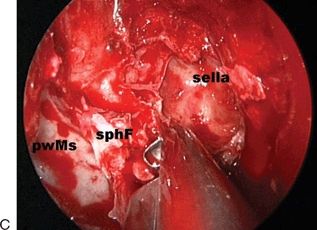

FIGURE 26.1 Approach phase (right side). A. The middle turbinate is resected through the ipsilateral nasal fossa. B. A complete sphenoethmoidotomy with a wide meatomy is performed. C. The posterior margin of the medial wall of the maxillary sinus (Ms) is resected to expose the posterior wall of the maxillary sinus (pwMs) and the vertical process of the palatine bone. D. After ligation of the sphenopalatine artery, the medial pterygoid process (pp) is drilled out. sphF, sphenopalatine foramen; OCr, optic–carotid recess.
This stage is performed holding the endoscope freehand. A 0-degree endoscope is normally sufficient; a 30-degree endoscope is seldom required. The middle turbinate is resected through the ipsilateral nasal fossa (Fig. 26.1A), increasing the peripheral view, improving the maneuverability of the surgical instruments and preserving the integrity of the mucoperiostium of the turbinate for harvesting of a mucosal graft. An ethmoidal route is used, and a complete sphenoethmoidotomy with a wide meatomy is performed (Fig. 26.1B). The posterior margin of the medial wall of the maxillary sinus is resected to expose the posterior wall of the maxillary antrum and the vertical process of the palatine bone (Fig. 26.1C). After ligation of the sphenopalatine artery, the medial pterygoid process is drilled out (Fig. 26.1D). The resection of the medial pterygoid process permits exposure of the inferolateral portion of the CS. As in the MTea, contralateral access to the surgical field is gained by removing a portion of the posterior aspect of the nasal septum along its attachment to the sphenoid rostrum.
At the end of this phase, a frontal view of the posterior wall of the sphenoid sinus is obtained, allowing the recognition of many bone landmarks in a pneumatized sinus (Figs. 26.2 and 26.3): the optic protuberance, the optic recess, the parasellar carotid protuberance, the planum, the tuberculum sellae, the sella, the paraclival carotid protuberance, and the clival indentation. In the poorly pneumatized sphenoid sinus, it is especially important to identify the course of the vidian nerve on the floor of the sinus; it has a mediolateral direction from anterior to posterior, indicating the genu between the petrous carotid artery and the paraclival carotid artery (Figs. 26.4 and 26.5).
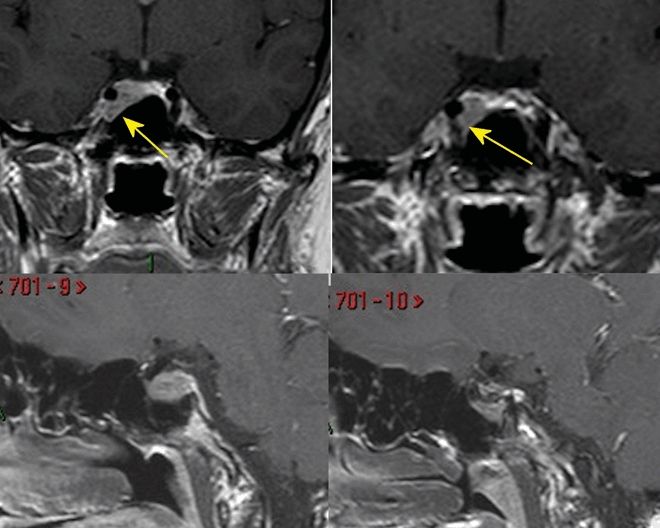
FIGURE 26.2 T1-weighted, contrast-enhanced coronal and sagittal MRI showing a pituitary adenoma growing in the medial and anteroinferior compartment of the right CS (arrows).
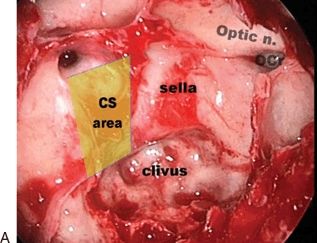
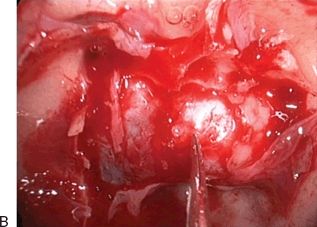
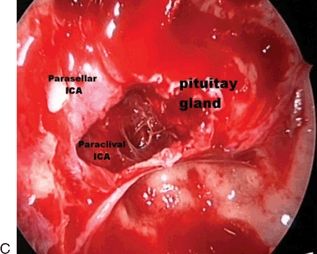
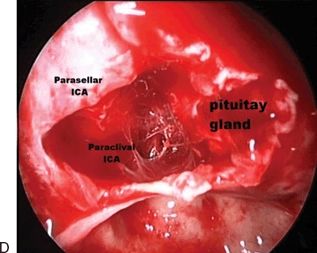
FIGURE 26.3 Intraoperative view of the patient in Figure 26.2. Image (A) shows a sphenoidal sellar variant with all main landmarks clearly visible: optic carotid recess (OCr), expanded sella, clivus, and parasellar and paraclival internal carotid artery (ICA) protuberance. With imaginary lines joining the landmarks, it is possible to highlight the projection onto the sphenoid wall of the cavernous sinus (CS). The following images show the dural opening (B), the intracavernous view after removal of the tumor in the medial compartment (C) and anteroinferior compartment (D) in the right CS. The preserved pituitary gland is clearly visible.
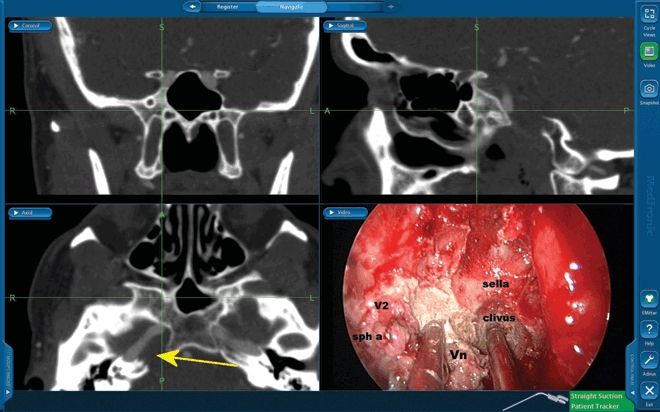
FIGURE 26.4 This image shows intraoperative CT angiography navigation in a poorly pneumatized sphenoid sinus (patient in Fig. 26.1). A chordoma is growing in the right petroclival area (arrow) just behind the petrous portion of the ICA. The medial suction tube (not navigated) points toward the clivus in the midline; the navigated suction tube is located between the vidian nerve (Vn) and the second division of the trigeminal nerve (V2) in the same plane and points toward the junction of the horizontal, petrosal part of the ICA with the ascending paraclival segment of the ICA (anterior genu). (sph a, sphenopalatine artery.)
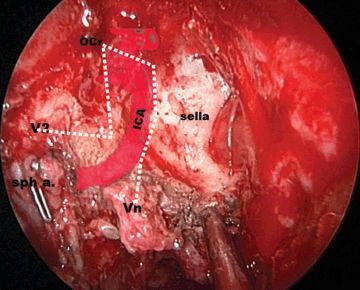
FIGURE 26.5 Intraoperative view of the patient in Figures 26.1 and 26.4. Colored angiography of the internal carotid artery (ICA) is superimposed on the endoscopic intraoperative image in order to better understand its relationship with the landmarks. With imaginary lines joining the landmarks, it is possible to highlight the projection onto the sphenoid wall of the CS and ICA. (Vn, vidian nerve; sph a, sphenopalatine artery; V2, second division of the trigeminal nerve; OCr, optic carotid recess.)
We emphasize the importance of the transpterygoid phase which is crucial to increase the maneuverability of the surgical instruments in a caudocranial direction and to expose the lateral wall of the sphenoid sinus and the inferior (lacerous) part of the CS. The amount of pterygoid process resection depends on the pneumatization of the sphenoid sinus: a more pneumatized sinus requires a more extensive resection of the pterygoid process in order to expose the lateral wall of the sphenoid sinus. Many bony landmarks may be visible on the lateral sphenoidal sinus wall and, in a caudocranial and anteroposterior direction, they consist of: the pterygoid foramen and the pterygoid protuberance posteriorly showing the lacerous portion of the paraclival carotid artery, the foramen rotundum about 1 cm above and lateral to the pterygoid foramen, the protuberance of the maxillary nerve, the orbital apex, and the optic protuberance (Figs. 26.3 to 26.5).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


