CHAPTER 28 Rhytidectomy
Historical Perspective
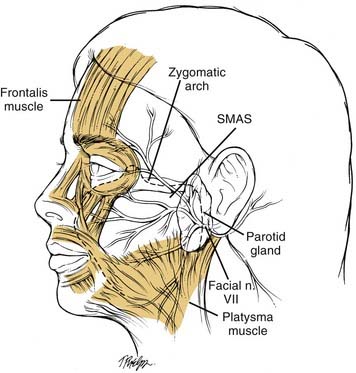
In 1907, Miller1 published the first medical book on the subject of cosmetic surgery. Thus was born the surgical field of aesthetic surgery. Around this same time, perhaps as early as 1901, the first rhytidectomy was performed and took the primitive form of excising skin and repairing the wound without undermining the facial skin. Early facelift techniques were probably developed by German surgeons, but by 1906, American surgeons were beginning to adopt and improve the techniques of facelifting. By 1926, surgeons were using coronal incisions for forehead lifting and were developing methods of dealing with the double chin. By the 1930s, facelift surgery had attained a level of sophistication that inspired no major innovations until after World War II, when the development of antibiotics and improved anesthesia provided safer elective surgery. Before World War II, aesthetic surgery was looked on by organized medicine with disfavor, believing that it was not warranted because of associated risks. By 1960, this attitude had changed somewhat. The greater affluence of the middle class and changing attitudes helped spawn a renewed interest in rhytidectomy. However, it was not until the 1970s that significant innovations in facelifting were introduced. This was initiated by the work of Skoog,2 who reported dissecting beneath the superficial fascia of the face. Before 1974, rhytidectomy had consisted of a simple subcutaneous dissection of facial and cervical skin with or without suture suspension of the underlying superficial fascia. Skoog demonstrated that an advancement flap dissected beneath the superficial fascia, later to be named the superficial musculoaponeurotic system (SMAS), while leaving the overlying skin attached, could improve the jaw line better than a subcutaneous dissection of the skin. Skoog’s discovery that enhanced results were possible from dissecting deeper than the conventional subcutaneous tissue plane ushered in a renaissance for rhytidectomy, and today surgeons are in the midst of this renaissance. Skoog’s report created considerable interest in the superficial facial fascia and led to the 1976 report by Mitz and Peyronie.3 This and subsequent studies showed that the SMAS is a fibromuscular fascial extension of the platysmal muscle that arises superiorly from the fascia over the zygomatic arch and is continuous in the inferior cheek with the platysma. Throughout this chapter, when the term SMAS is referred to, the reader should understand that this structure consists of a fibrous layer of connective tissue in the mid-face but has more consistency in the inferior cheek, where it consists of the platysmal muscle. This is particularly true over the tail of the parotid gland and anterior to the gland. The distribution of the facial nerve is deep to the SMAS (Fig. 28-1).3 Presumably, the function of the SMAS is to transmit to the facial skin the activity of the facial mimetic musculature.
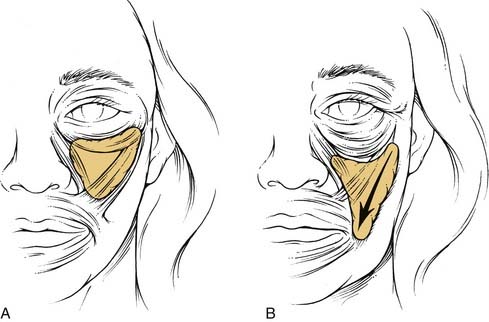
Yousif and others investigated the anatomy of the melolabial fold and found that the fold resulted from descent of the anterior cheek fat and overlying attached skin.4 With aging, the cheek fat of the mid-face descends inferomedially (Fig. 28-2). This tissue migration has the effect of enhancing the melolabial fold and deepening the melolabial crease. At the same time, the orbicularis muscle of the lower eyelid stretches and descends inferolaterally. This movement causes the margin of the lower eyelid to move below the inferior limbus, which, in turn, produces scleral show. The junction between the cheek and lower eyelid descends below the orbital rim, causing skeletonization of the inferior bony orbital rim and, in some patients, the development of a nasojugal groove. On the basis of the anatomic changes of the lower eyelid and mid-face that occur from aging, it eventually became evident that rejuvenation of the mid-face required elevation and fixation of the mid-facial soft tissues and correction of the redundant orbicularis muscle of the lower eyelid by excision or repositioning of the muscle superomedially.
The SMAS is essentially a fascial extension of the platysmal muscle beneath the cheek fat of the mid-face.4–7 Traction placed on the SMAS is not transmitted to the melolabial fold and as a consequence does not ameliorate the fold. This is because the SMAS is effectively anchored by the bony origins of the mimetic muscles it envelops, especially the zygomatic major muscle in the region of the body of the zygoma. This point of fixation prevents the upward lateral displacement of a sub-SMAS rhytidectomy flap and the flattening of the melolabial fold. This finding led to the realization that a sub-SMAS dissection must release the investments of the SMAS to the zygomatic musculature to move the SMAS and the overlying cheek fat upward, thereby improving the melolabial fold and the appearance of the mid-face.8 The deep-plane rhytidectomy perfected by Hamra extended a sub-SMAS dissection of the inferior cheek superiorly, cutting through the SMAS peripherally, and releasing it from its investment of the zygomatic muscles, so that the SMAS and the overlying skin and subcutaneous tissues could be advanced upward.9 This release was accomplished by transitioning from a sub-SMAS plane in the inferior cheek to a supra-SMAS plane in the superior medial cheek (Fig. 28-3). The dissection extended medially beyond the melolabial fold, totally releasing all SMAS attachments to the dermis of the upper lip and creating a thick musculocutaneous flap composed of skin, subcutaneous fat of the cheek, and the platysma. Hamra subsequently modified the deep plane rhytidectomy by including the orbicularis oculi in the rhytidectomy flap and termed it a composite rhytidectomy.10 Owsley11 showed that by dissecting medially from the malar eminence to the lateral upper lip just superficial to the SMAS in the plane immediately above the orbicularis oculi, zygomaticus, and levator muscles, the cheek fat could be suspended superiorly, restoring a youthful appearance to the mid-face and effacing the melolabial fold. He showed that a sub-SMAS dissection was not at all necessary to improve the mid-face. Owsley’s approach is often referred to as an extended supra-SMAS rhytidectomy.
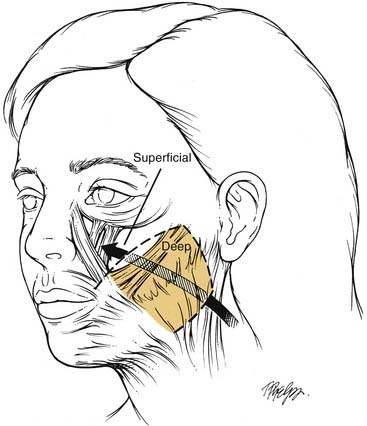
Figure 28-3. The deep-plane rhytidectomy described by Hamra19 extended a sub-superficial musculoaponeurotic system (sub-SMAS) dissection of the inferior cheek superiorly, cutting through the SMAS peripherally, thus releasing the SMAS from investments to the zygomatic muscles, so that the SMAS and overlying skin and cheek fat could be mobilized upward. This release was accompanied by transitioning from a deep (sub-SMAS) plane in the inferior cheek to a superficial (supra-SMAS) plane in the superior medial cheek.
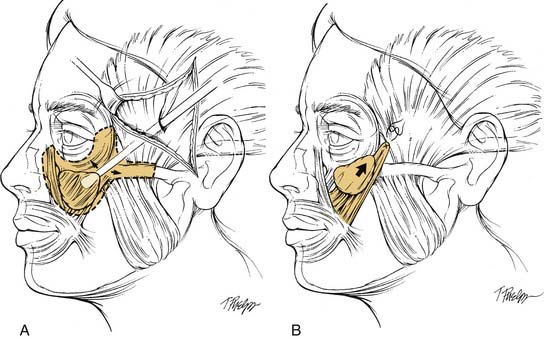
The knowledge gained from the clinical and anatomic studies performed in the mid and late 1970s enabled continued refinement of sub-SMAS and extended supra-SMAS dissection techniques, culminating in the early 1990s. Emerging in parallel with these surgical approaches was the development of a different concept for rejuvenating the mid-face accomplished by a subperiosteal dissection. In 1980, Tessier12 demonstrated that undermining the periosteum of the superior and lateral orbital rim allowed elevation of the soft tissues of the forehead and eyebrows, with improved results compared with previous techniques for forehead lifting. In 1988, Psillakis and others13 reported on a subperiosteal rhytidectomy technique that involved detachment of all periosteum from the bony orbital rims, upper maxilla, zygoma, and nose. After this detachment, the soft tissues of the forehead, lateral canthus, mid-face including the melolabial folds, and to some degree the jowls were lifted to reestablish a more youthful relationship with the underlying facial skeleton. Because of troubling temporary forehead paralysis from trauma to the temporal branch of the facial nerve (6.7%), the authors advocated restricting subperiosteal dissection of the zygomatic arch to the anterior third to reduce the risk of injury. Ramirez and others14 modified the subperiosteal facelift described by Psillakis, permitting significant improvement in the safety and clinical results. They released the periosteum from the entire zygomatic arch by dissecting deep to the temporalis fascia. The temporalis fascia was then used as a lifting and anchoring element of the entire cheek and perioral soft tissues (Fig. 28-4). The surgical approach by Ramirez and others showed improved mid-face suspension by. complete subperiosteal undermining of the mid-facial bones. The suspension seemed to have the same influence on the melolabial fold as the deep-plane facelift, that is, elevation of the ptotic cheek fat to a more youthful position with effacement of the fold.
The subperiosteal facelift described by Ramirez and others14 is technically difficult, because it requires a temporal approach, which is considerably removed from the body of the zygoma and the anterior maxilla where the mid-face soft tissues are attached. As with the deep-plane rhytidectomy, visibility anterior to the convexity of the zygoma is limited, and it may be necessary to perform some dissection blindly. Because the temporal approach by itself presents difficulties with detachment of the periosteum from the maxilla, surgeons turned to other approaches. The most popular of these was transorbital access to the mid-face achieved by performing a lower lid blepharoplasty incision. The periosteum was released from the maxilla and zygoma, and the soft tissues of the mid-face were suspended either to a periosteal cuff at the inferior bony orbital rim or to the temporalis fascia in the anteroinferior aspect of the temporal fossa.15–18 A major drawback of the transorbital route was not infrequent problems of lower lid retraction or even ectropion. This complication occurs from trauma to the orbicularis oculi and subsequent scar contracture. Some surgeons recommended concomitant lateral canthoplasty or at the very least canthopexy to reduce this risk. Other surgeons avoided this risk altogether by combining a transtemporal and transoral approach and not performing any dissection of the mid-face through the lower eyelid. The transtemporal approach was used to elevate the periosteum from the zygomatic arch and the superior aspect of the zygoma. The transoral approach was used to free the periosteum from the maxilla and inferior aspects of the zygoma. This combined approach had the advantage of allowing the surgeon direct access for performing a subperiosteal dissection of the entire mid-face under direct vision without the need of an endoscope. It also avoided the risk of lower eyelid retraction or ectropion.
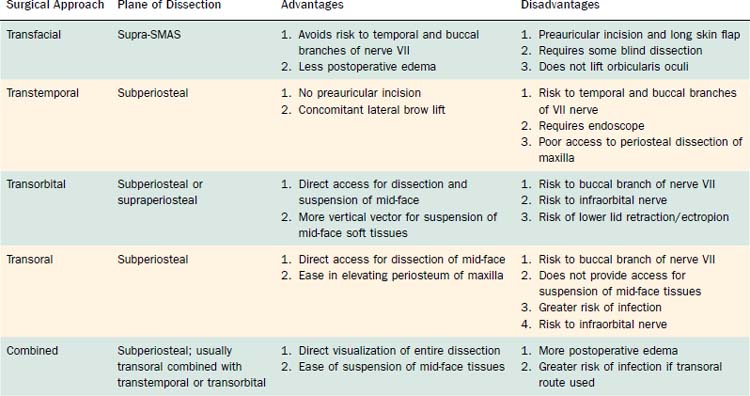
Proponents of the subperiosteal approach point to the safety of keeping all of the soft tissue, including the facial nerve, above the plane of dissection. There is less risk of injury to the zygomatic and buccal branches of the facial nerve with the subperiosteal approach compared with the deep-plane or extended supra-SMAS facelift. There is no disruption of the blood supply to the skin of the mid-face, because the plane of dissection is beneath all of the major blood supply to the face. There is no need for a lengthy skin flap lifted from the preauricular area or for a blind dissection of soft tissues of the mid-face. Although not part of the discussion in this chapter, it has become apparent that the aging changes in the lower periocular area are maximally rejuvenated when mid-facelifting is performed in conjunction with orbicularis oculi repositioning to a more superior and medial position.10 Repositioning of the ptotic orbicularis muscle is most easily accomplished by performing a subperiosteal mid-facelift. Transfacial supra-SMAS mid-facelifts do not reposition this muscle. Table 28-1 summarizes the advantages and disadvantages of the various approaches to lifting the mid-face.
Table 28-1 Dissection Planes of Mid-Facelifting
| Advantages | Disadvantages | |
|---|---|---|
| Subperiosteal | ||
| Supra-SMAS |
Surgical Approaches
Although there are a multitude of variations in performing a rhytidectomy of the lower face and upper neck, they may be divided into four categories according to the tissue planes used for dissection. These include subcutaneous, sub-SMAS, supra-SMAS, and subperiosteal (Table 28-2).
Subcutaneous Rhytidectomy
All approaches except the endoscopic facelift without preauricular or postauricular incisions call for some subcutaneous tissue dissection of the facial skin. The postauricular skin flap is always elevated in the subcutaneous tissue plane. Likewise, the preauricular skin must be dissected in a similar plane for variable distances before incisions can be made through the SMAS. Typically, the skin of the upper neck is also elevated in the subcutaneous tissue plane or immediately superficial to the platysmal muscle (preplatysmal). Dissection may continue forward in the neck to the midline. The extent of anterior dissection in the subcutaneous tissue plane of the face depends on the surgeon’s preference and may be influenced by the degree of facial skin laxity. In the past, there have been controversies concerning the benefits of long-flap versus short-flap rhytidectomies. A benefit of dissecting to the lateral bony orbital rim in the temple is that it releases the skin from the underlying orbicularis oculi. This helps to improve the crow’s feet and also assists with redistribution of the vertically advanced preauricular skin flap. Once a skin flap has been elevated, the exposed SMAS can be plicated by folding it on itself using sutures to suspend it to the periparotid fascia. The subcutaneous facelift with plication of the SMAS is still the most common surgical approach used by plastic surgeons, composing 23% of facelift procedures performed.19 It is probably the safest approach from the standpoint of risk of facial nerve injury but has the disadvantages compared with other techniques of shorter long-term improvement of the jowl and no correction of the mid-face.
SMAS Rhytidectomy
The sub-SMAS dissection of the lower face is another common surgical approach performed by approximately 20% of facelift surgeons.19 This may take the form of elevating an SMAS flap limited to the area over the parotid gland (25% of surgeons) or extending the SMAS flap anterior to the parotid gland. The SMAS flap is then suspended posterosuperiorly. Neither approach lifts the mid-face, but both markedly improve the jowl. When an SMAS flap is dissected from the parotid fascia, it is frequently referred to as an SMAS rhytidectomy. Dissecting beneath the SMAS anterior to the parotid gland and then transitioning to a supra-SMAS plane and dissecting all of the cheek fat with attached overlying skin away from the zygomatic musculature as described by Hamra is known as a deep-plane rhytidectomy (see Fig. 28-3).19 Later, Hamra added to this dissection a supraperiosteal dissection of the superior aspect of the mid-face through a lower eyelid incision. This biplane dissection was termed a composite rhytidectomy by Hamra.10 Nine percent of facelift surgeons perform a deep plane or composite rhytidectomy.19
A variation of the sub-SMAS dissection is a strip SMAS-ectomy described by Baker.20 This technique consists of excising a strip of SMAS along a line that extends from the angle of the mandible to the lateral malar eminence. Usually, a 2- to 4-cm wide strip of SMAS is excised, depending on laxity. Much of this excision is anterior to the parotid gland. No anterior dissection beneath the SMAS is performed. The SMAS is reapproximated, advancing the mobile SMAS and platysma posterosuperiorly to the junction of the SMAS fixed to the periparotid fascia. Approximately 20% of facelift surgeons use the technique of SMAS-ectomy.19 It has the advantage of simplicity but does not address the mid-face.
Supra-SMAS Rhytidectomy
The main disadvantage of the extended supra-SMAS rhytidectomy is the long preauricular skin flap resulting from a lengthy anterior dissection. This creates a potentially large dead space where hematomas can collect. A dissection beyond the convexity of the zygoma may require some blind dissection or at least impair the exposure available to the surgeon. In addition, remaining above the SMAS throughout the dissection does not provide as much improvement of the jowl compared with developing a SMAS flap of the inferior cheek. Approximately 20% of facelift surgeons perform the extended supra-SMAS rhytidectomy.19 The advantage of the deep-plane facelift compared with the supra-SMAS lift is that the inferior cheek is dissected in a sub-SMAS plane, creating an advancement flap, whereas the mid-face is dissected in a supra-SMAS plane. The sub-SMAS dissection in the lower face provides long-term correction of the jowl.21
Subperiosteal Rhytidectomy
Subperiosteal rhytidectomy refers to the lifting of the cheek tissues by dissecting in the subperiosteal plane over the maxilla and zygoma. The procedure usually includes an endoscopic subperiosteal forehead lift as well. All of the soft tissues of the mid-face are lifted, including the elevators of the lip, the zygomatic major and minor, and often the orbicularis oculi. The fundamental difference between the subperiosteal mid-facelift and the transfacial supra-SMAS facelift is the superior displacement of these muscles (see Fig. 28-4
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


