CHAPTER 36 Rhinoplasty
Preoperative Patient Assessment
Anatomic Evaluation
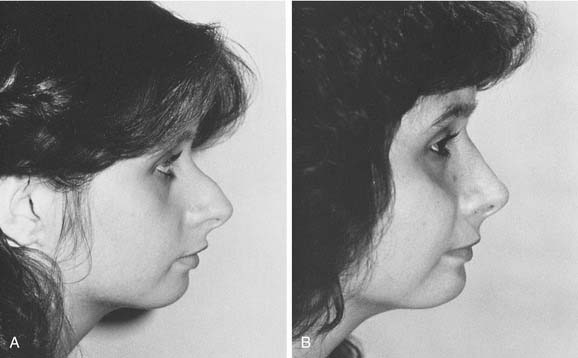
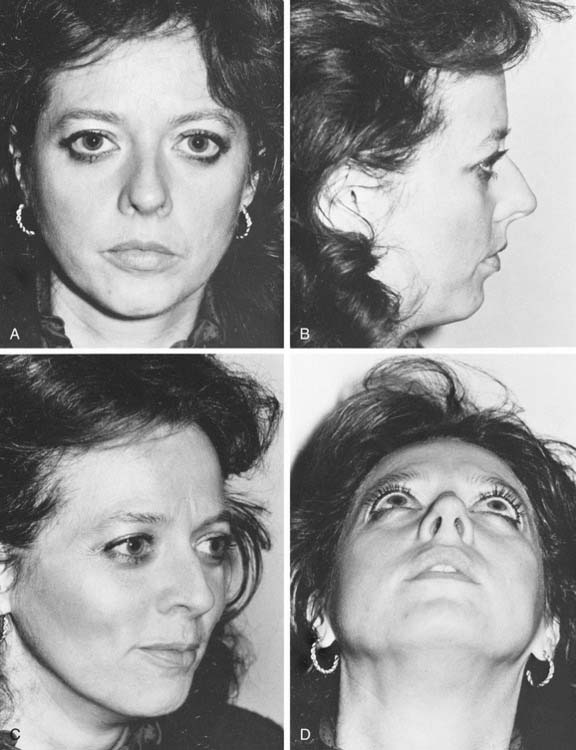
The final result of any rhinoplasty procedure is the consequence of the individual patient’s anatomy (Fig. 36-1) as much as the surgeon’s skill. No two noses are ever quite alike; it follows then that no single, standard procedure suffices to reconstruct every nose pleasingly. The ability to diagnose the possibilities and limitations inherent in each patient is an absolute prerequisite to achieving outstanding results. Sometimes patients with minimal deformities (a small hump; a minimally bulbous tip; a slightly overwide nose) are the best candidates for near-perfect surgical results (Fig. 36-2). Because the initial problem is minimal, however, this group of patients often expects and even demands perfection. More dramatic surgical results are possible in patients who demonstrate significant departures from an aesthetic ideal (a large hump; an elongated, drooping nose; a twisted nose); these patients might tolerate possible minor imperfections that result because the overall improvement is dramatic (Fig. 36-3). It is the fundamental responsibility of the surgeon to balance the wishes and desires of the patient with what is realistically possible given the anatomic limitations (or possibilities) inherent in each individual nose.
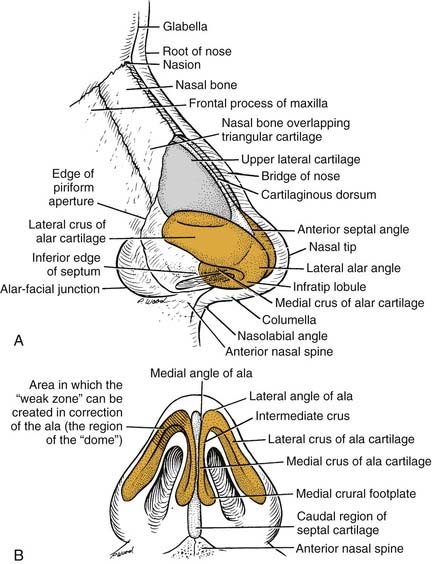
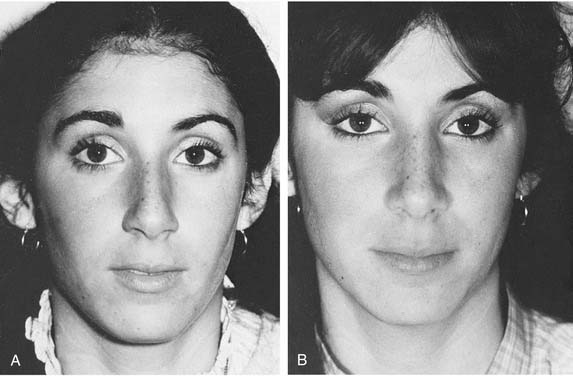
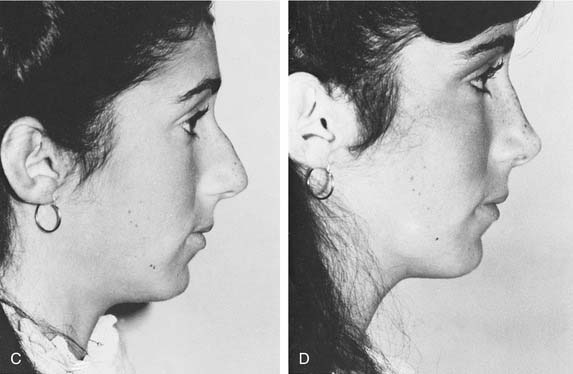
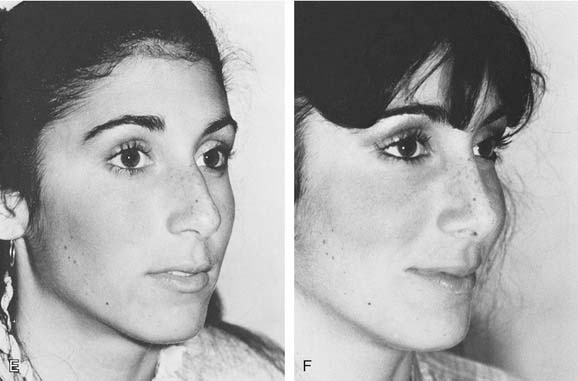
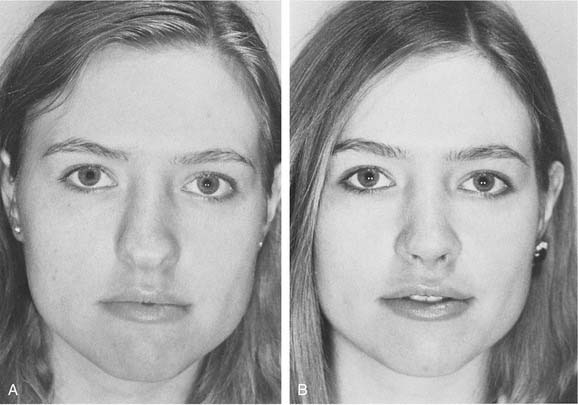
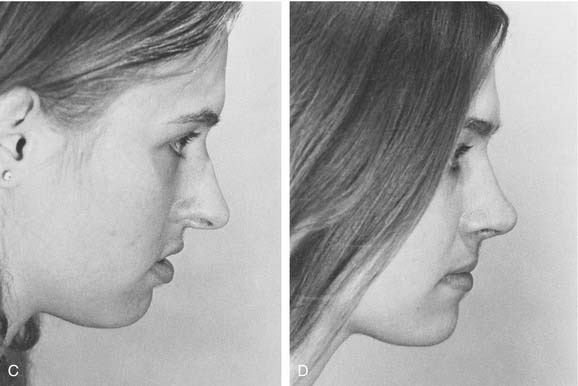
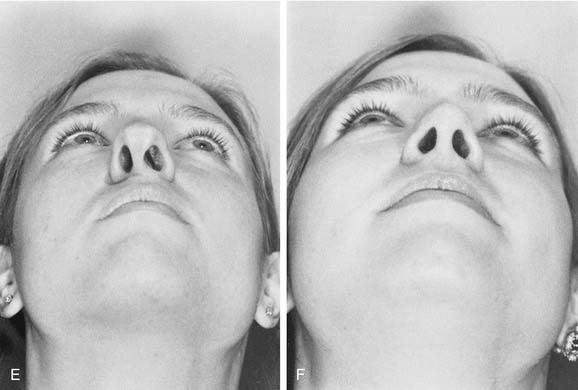
Figure 36-2. Ideal candidate for rhinoplasty surgery. A, C, and E, Preoperative views. B, D, and F, Postoperative views.
The quality of the skin is an essential indicator of the surgical outcome and plays a significant role in preoperative planning. Extremely thick skin, rich in sebaceous glands and subcutaneous tissue, is the least ideal skin type for achieving desirable refinement and definition. Care should be taken not to overreduce the bony-cartilaginous skeleton in thick-skinned patients in a futile attempt to produce a much smaller nose. Failure of thick skin to contract favorably in this situation may lead to excess soft tissue scar, an amorphous nasal appearance, and even the dreaded soft tissue “pollybeak” (Fig. 36-4). When properly supported by the retention or creation of a vigorous supportive skeletal structure, elegant outcomes can be produced in thick-skinned patients with sufficient passage of time.
A critical factor in assessing the candidate for rhinoplasty is the inherent strength and support of the nasal tip, referred to as the tip recoil. Finger depression of the tip toward the upper lid provides a quick and reliable test of the ability of the mobile tip’s structures to spring back into position (Fig. 36-5). The tip that possesses weak, somewhat flail alar cartilages does not tolerate an extensive sacrifice of tissue well and may require the addition of supportive struts to improve its long-term stable support. These weak tips often are accompanied by thin alar side walls and thin skin (see Fig. 36-31C). If the recoil is instantaneous and vigorous, and the tip cartilages resist the deforming influence of the finger, more definitive tip surgery can usually be performed without fear of substantial loss. The size, shape, attitude, and resilience of the alar cartilages can be estimated by palpation or ballottement of the lateral crus between two fingers surrounding its cephalic and caudal margins. During this assessment, the surgeon makes the all-important decision about whether to enhance, reduce, or carefully preserve the tip projection that exists preoperatively. Any asymmetry of the alar cartilages must be carefully noted for later correction.

A gratifying amount of diagnostic information can be gained by palpating the internal vestibules of the nose with the thumb and forefinger surrounding the columella. Otherwise, undetected twists and angulations of the nasal septum, which may significantly influence the final functional and aesthetic appearance, may not be discovered. The width and length of the columella and the medial crura it contains are determined. Short medial crura will probably require supportive cartilaginous struts to support and minimally lengthen the columella and aid in rotation, if desirable; extremely flaring or overlong medial crura invite reduction in width and length as well as retropositioning. Information about the potential of the tip to undergo desirable cephalic rotation is gained by the exploring fingers, which determine whether the tip-lip complex is tethered by muscle and its inadequate length. It is also important to determine whether the central skeletal component of the nose (the quadrangular cartilage) is overlong and might interfere with satisfactory tip rotation (Fig. 36-6). The size and position of the nasal spine and its related caudal septal angle must also be evaluated.
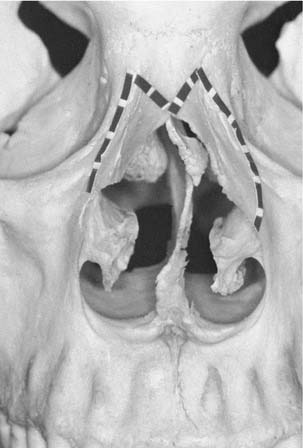
Careful examination of the nasal fossae before and after shrinkage of the mucosa and turbinates is an essential component of the initial examination. Supplemental anterior and posterior rhinoscopy with the fiberoptic rhinoscope expands diagnostic information beyond that furnished by the nasal speculum alone. An overt, symptomatic deviation of the nasal septum is easily diagnosed; the deflected ethmoid plate, which may appear innocent but can be responsible for airway blockade after infraction of the bony side walls during an osteotomy (Fig. 36-7), may be easily overlooked by casual inspection. Internal examination confirms the condition of the internal nasal valves and their associated upper lateral cartilages and discovers whether the turbinates require repair or relocation to improve overall nasal function. If a septal perforation exists, its size and location may significantly influence the planned extent of the surgical procedure, particularly if substantial hump removal is planned.
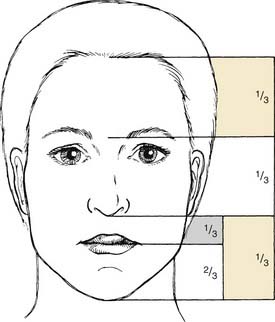
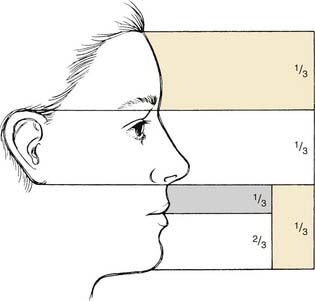
Finally, the position and inclination of the nasofrontal and nasolabial angles, the shape and size of the alae, the overall width of the middle and upper thirds of the nose, and the relationship of the nose to the remainder of the facial features and landmarks are evaluated (Fig. 36-8). In particular, facial asymmetries (which are present more often than not) and the relationship of the chin projection to the nose should be documented (Fig. 36-9), particularly for patients who are unaware of the existence of such abnormalities. The routine use of a three-way mirror, facial photographs, and even computer imaging catalyze this vitally important communication process between the expectant patient and the cautious surgeon. This is the time, reinforced by later discussions, to make the patient aware of any and all limitations that the existent variant anatomy imposes on the desired surgical outcome. Realistic expectations and thoroughly informed consent are the keystones on which the most important surgical outcome—a happy patient—is achieved.
Photography and Imaging
Standard and uniform color photography of a rhinoplasty patient, recorded before and serially after the surgical event, are as important to the rhinoplasty surgeon as radiographs are to bone specialists and electrocardiograms are to cardiologists. They are important guides to operative planning and execution, definitive records for evaluation by the surgeon and patient, invaluable teaching tools, and vital medicolegal records. Reliable methods of making standardized, consistently uniform photographs are described in Fig. 36-10. A rhinoplasty surgeon should either become expert in personally securing uniform and standard photographs or should arrange uncompromisingly for their provision by a medical photographer or knowledgeable assistant. Modern digital photography has multiple advantages including ease of storage and retrieval.
Anesthesia and Analgesia
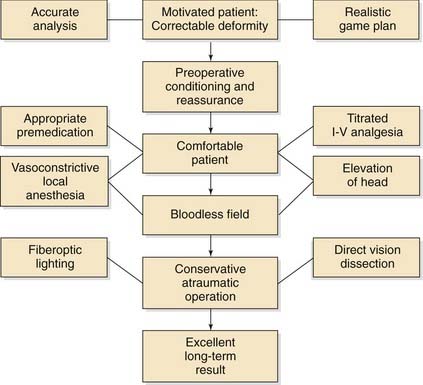
Each surgical step in the correction of the nose is interrelated and interdependent with the other steps; the success of each step depends in no small measure on the preceding ones. Because the administration of infiltrations anesthesia is the initial surgical step in rhinoplasty, a well-planned and well-executed technique that avoids tissue distortion is necessary for a successfully controlled procedure (Fig. 36-11).
Surgical Planes
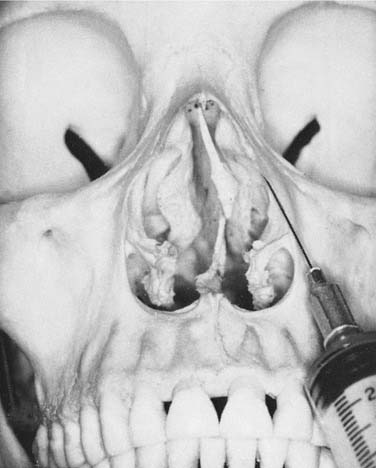
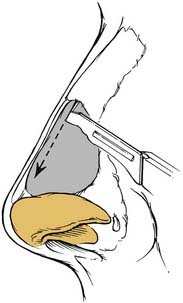
Within the nose, four distinct dissection planes can be identified. An extraperiosteal plane exists lateral and medial to the ascending process of the maxilla along the intended course of the lateral osteotomies. Infiltration of the local anesthetic on both sides of the ascending process aids remarkably in eliminating or reducing bleeding after a lateral osteotomy (Fig. 36-12). A second plane exists in the submucoperichondrial and submucoperiosteal spaces flanking the nasal septum. Infiltration of the local anesthetic into this plane results in a hydraulic dissection of the septal flap, facilitating elevation and preservation of flap integrity (Fig. 36-13). Of greatest importance is the surgical plane occupying the immediate supraperichondrial and supraperiosteal regions over the lower and upper cartilages and nasal bones that exist just below the subcutaneous tissue layer (Fig. 36-14). It is entered in all rhinoplasty operations. Infiltrating and operating in this plane produces a virtually bloodless field for delicate precision surgery. The fourth relatively avascular and favorable dissection plane exists in the submucoperichondrial space flanking the septal cartilage on either side.
Infiltration Anesthesia
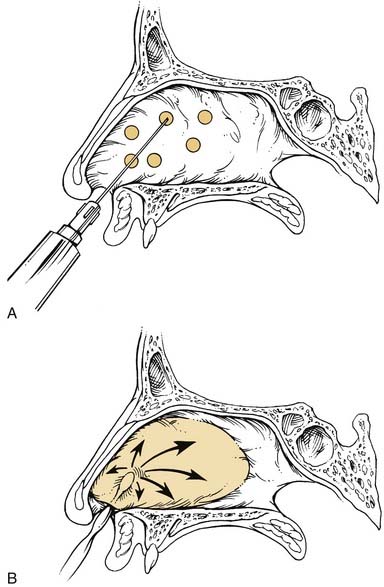
The infiltration of the local anesthetic is initiated by retracting the ala cephalically with the thumb and forefinger, exposing the caudal edge of the upper lateral cartilage (specula or retractors are unnecessary and redundant at this point). A long 27-gauge needle is placed parallel to the long axis of the exposed upper lateral cartilage, and with a quick stabbing motion the needle penetrates the epithelium, usually with minimal sensation to the patient (Fig. 36-15A).
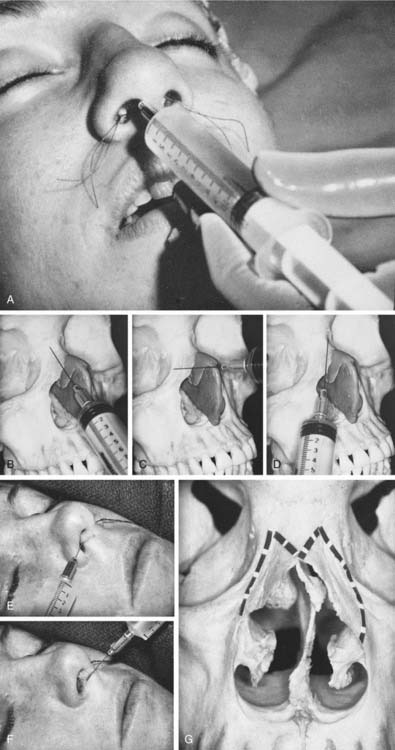
A minimal quantity of anesthetic solution, usually less than 0.5 mL, is deposited into this plane as the needle is withdrawn to but not beyond the point of initial penetration (see Fig. 36-15B). If the nose becomes distorted during this maneuver, the needle is not in the proper plane, and the infiltration stops until the plane is located. With alternate slight rotation of the needle laterally and medially over the dorsum (see Fig. 36-15C and D), the procedure is repeated until the anesthetic is deposited in the proper plane over the area to be dissected. The procedure is repeated on the opposite side. With this method, only two injection penetrations are sufficient to anesthetize the nasal dorsum.
Anesthesia of the base of the nose and columella is accomplished next. The needle penetrates the skin at the junction of the floor of the right nostril and columella and is advanced to a point just beyond the left alar facial junction (see Fig. 36-15E). Infiltration occurs as the needle is withdrawn to the columella. Without removal, the needle is rotated and advanced into the columella. Again, a small amount of anesthetic is deposited as the needle is withdrawn. Sparing the patient an additional needle prick, the needle is rotated into the right nasal base, which is anesthetized in a similar fashion (see Fig. 36-15F).
The anesthetic can then be deposited along the course of the lateral osteotomies (see Fig. 36-15A and B) or, if desired, this can be deferred until later in the operation. This delay adds a safety measure to the procedure by allowing the patient to metabolize the initial lidocaine and epinephrine before adding any additional solution. The margin of the piriform aperture just above the leading anterior edge of the inferior turbinate is brought into sharp relief by surrounding it with the blades of a small nasal speculum. The needle is inserted at this site, and a small amount of medication is injected. The needle is advanced lateral to and then medial to the ascending process of the maxilla along the intended path of the lateral osteotomies (see Fig. 36-15G
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


