Incidence may be higher
Advanced intraocular disease at presentation
Extraocular disease at presentation
Delayed diagnosis
Existence of several barriers to optimal delivery of care
Poor survival rate
International collaborative efforts are necessary to improve the survival
5.2 Incidence
In a previous chapter, Bunin and Orjuela introduced evidence that the incidence of nonheritable retinoblastoma may be higher in some developing countries, especially among the poorer populations. Increased incidence of retinoblastoma has been reported in tropical Brazil, south Mexico, indigenous populations in Alaska, and some African countries [2–4]. As reliable data on cancer incidence in many developing countries are usually lacking, these findings should be confirmed in larger, properly designed, population-based studies.
There is no sound explanation for this reported increased incidence. These authors suggest that variation in the incidence may be due to environmental factors. Studies trying to link the human papillomavirus (HPV) to the pathogenesis of retinoblastoma led to controversial results [5–7]. In Mexico, low intake of fruit and vegetables during pregnancy also correlates with a higher risk of having a child with sporadic nonheritable retinoblastoma [6].
5.3 Clinical Features
5.3.1 Presenting Signs of Retinoblastoma in Developing Countries
Presenting signs of retinoblastoma vary depending where in the world the affected child lives (Fig. 5.1). Strabismus, a presenting sign in 20 % of children in the United States, is not recognized as a presenting sign in Central Africa [8]. Proptosis due to orbital extension of retinoblastoma, which is rarely a presenting sign of retinoblastoma in the United States [9], is one of the commonest presenting signs in lower-income countries [10, 11].
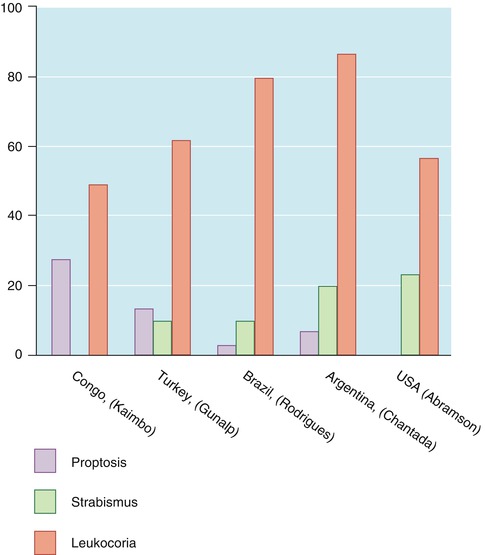
Fig. 5.1
Comparison of presenting signs of patients with retinoblastoma in different countries
5.3.2 Extraocular Retinoblastoma at Presentation
There is evidence that retinoblastoma presents more frequently with massive extraocular dissemination in developing countries (Fig. 5.2). It is important to recognize that these children usually present with severe malnutrition leading to cachexia and severe orbital pain in extreme cases, so treatment should include prompt supportive care. Delayed diagnosis is implicated as a major factor leading to extraocular dissemination and subsequent metastasis.
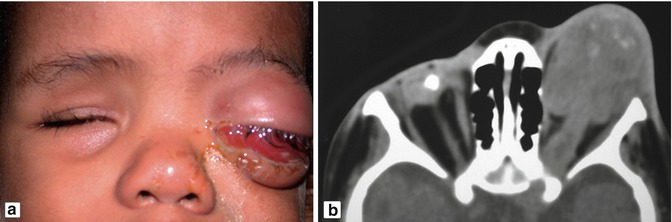
Fig. 5.2
Patient with bilateral retinoblastoma and overt extraocular extension OS (a) which is confirmed by computed tomography (b)
5.4 Delayed Diagnosis
Delayed diagnosis is a complex phenomenon in which patient and physician-related factors and socioeconomic factors play a role.
5.4.1 Patient-Related Factors
Patient-related factors include symptoms of retinoblastoma in young children who are unable to express visual disturbances together with the lack of awareness of the general population that ocular abnormalities such as strabismus and leukocoria may be signs of cancer.
5.4.2 Physician-Related Factors
Invariably, parents or other family members are the first to notice the visual abnormality. Pediatricians are frequently the first physicians to evaluate the affected child. It is rare for the pediatrician to detect leukocoria because of limited ophthalmic examination with undilated pupil in routine examinations. Therefore, they rarely recognize the significance of the parents’ complaints. As a result, many patients are not diagnosed or referred to an ophthalmologist on the first visit to the pediatrician. In a large cohort from Mexico, the majority of first contact physicians lacked basic information about retinoblastoma [14] (Fig. 5.3). All these factors add critical weeks or months to the delay in diagnosis of retinoblastoma (Fig. 5.4).
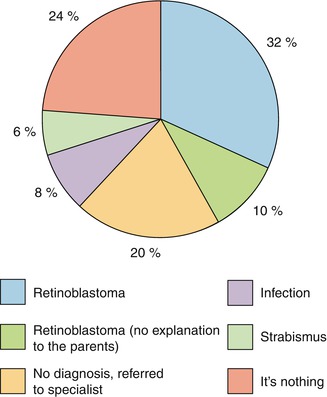
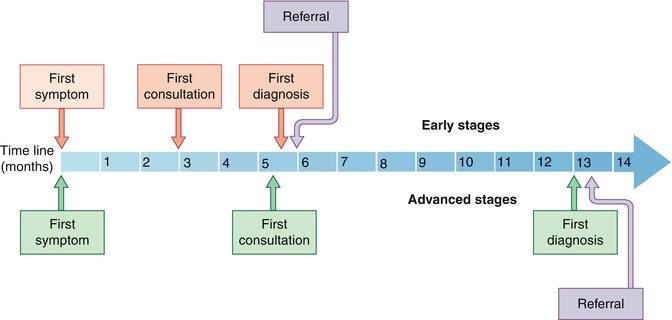
Fig. 5.3
Action taken by the pediatrician or ophthalmologist after the first consultation of a patient with retinoblastoma in Mexico
Fig. 5.4
Schematic representation of the diagnostic pathway of children with retinoblastoma in Mexico according to the disease extension
In Africa, most children present to the clinics and the nurses are the first to examine the child. If there is suspicion of abnormal examination or nonresponse to initial treatment, the child is referred then to the general doctor.
Physician’s delay in the recognition of the symptoms was found to be the main reason in failing to recognize retinoblastoma, which had the longest delay to diagnosis – 5 months in a study in South Africa [15].
5.4.3 Socioeconomic Factors
Socioeconomic factors such as parental education, lack of health insurance, living in villages remote from large cities and human development indexes are significant risk factors for systemic dissemination of disease and ultimately survival [1]. Patient-related factors are not always associated with the low level of education of the parents or the socioeconomic conditions [15].
5.5 Survival
5.5.1 Survival with Retinoblastoma Is Lower in the Developing Countries
Survival rates lower than 50 % have been reported in lower-income countries [1]. Since more than 80 % of the world’s children live in developing countries, globally, there may be more children dying of retinoblastoma than surviving. In middle-income countries, significant advances have been made in the past decades, and survival rates greater than 80 % are obtained in many countries.
5.5.2 Steps to Improve Survival
An improvement in the survival of patients with retinoblastoma in developing countries should not depend only on better treatment for extraocular disease. Rather, early detection and diagnosis with consequent reduction in systemic dissemination is expected to improve overall survival rate. A coordinated multistep approach involving public awareness, professional education, screening, but ultimately socioeconomic development is necessary. To be effective, resources must also aim to decrease the probability of treatment refusal.
5.5.2.1 Public Awareness Programs
In order to address this public health problem, some developing countries have embarked on public awareness programs about the signs and symptoms associated with retinoblastoma. One of the earliest and most important programs of this kind was developed in Brazil. To increase awareness of leukocoria as a presenting sign, the program targeted the general population through TV advertising and billboards. Other groups in Central America distributed pamphlets with information at vaccination centers and pediatricians’ offices [16]. The impact of these programs in the outcome of retinoblastoma is difficult to estimate. Awareness campaigns should target populations where the problem is mortality because of metastatic retinoblastoma at presentation. Their role for the detection of early intraocular disease is unknown.
5.5.2.2 Professional Education Programs
An educational program to increase awareness of retinoblastoma among primary care physicians, especially those working in rural areas, has been established in some countries. In addition more detailed information about retinoblastoma has been inserted into the medical school curriculum.
5.5.2.3 Screening for Retinoblastoma
Retinoblastoma may be an ideal candidate for screening (Box 5.2). Since children with a family history for retinoblastoma have been screened for many years by dilated examination under anesthesia, the natural history of the intraocular disease is well known; however, in middle-income countries, most children with a family history of retinoblastoma are not screened [17]. Additionally, retinoblastoma presents in a narrow age range, constituting a well-defined target population to be screened. Because retinoblastoma occurs at an age when routine visits to the pediatrician are more common, these practitioners should probably be involved in the screening. However, the perfect test for screening and a proper program are still to be developed.
Box 5.2. Screening for Retinoblastoma
Retinoblastoma may be an ideal candidate for screening |
Natural history of the intraocular disease is well known |
Presentation in a narrow age range, constituting a well-defined target population |
Retinoblastoma occurs at an age when routine visits to the pediatrician are more common |
Programs that involve pediatricians in the screening should be developed |
Relationship between early diagnosis and enhanced prognosis for eye salvage and patient survival |
5.5.2.4 Minimizing Treatment Refusal
Families refuse or withdraw treatment in as many as 30 % of children diagnosed with intraocular retinoblastoma in many parts of the developing world [18]. Refusal of enucleation as the major cause of treatment withdrawal attests to many cultural and religious barriers to effective treatment of retinoblastoma that exist among indigenous populations in the developing world. Socioeconomic factors also play a large role, especially in health systems where medical care is not free of charge for the families [19]. Because families frequently must travel long distances to receive medical care for retinoblastoma, many choose, following diagnosis and treatment recommendations, to return home where the child dies. The lack of financial resources to support the family during a stay in the referral center as would be required for an extended course of chemoreduction is a common cause of treatment refusal. Also, there are other family members at home who must be cared for. Therefore, treatment programs must take all of these factors into consideration.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


