Fig. 13.1
Schematic view of the natural history of intraocular retinoblastoma growth with respect to the invasion of five clinically recognizable anatomic sites: (a) retina, (b) retrohyaloid space, (c) subretinal space, (d) vitreous cavity, (e) posterior and anterior chambers
While solid vascularized retinal tumors are easily accessible to various treatment modalities, the tumoral avascular counterpart involving the other ocular sites is either poorly controlled by conventional therapies or beyond any conservative treatment as in the case of anterior segment invasion (absolute indication for enucleation). The high drug resistance of these avascular tumors may be explained by the inability of the present routes of administration to achieve tumoricidal concentrations in the corresponding eye compartments. In addition, these tumors are virtually inaccessible to focal treatments and are highly radioresistant due to their hypoxic nature.
13.4 Clinical Features
The tumor appearance and growth patterns will differ according to the physical nature of the invaded compartments. Solid tumors will adopt either a hemispherical endophytic or exophytic shape or a diffuse planar infiltration within the retinal tissue (diffuse infiltrative variant). Tumor spread into the viscous vitreous gel initially resembles dusty (loose cellular spread) or cloudy (dense cumulus-like spread) infiltrates, resulting from localized versus massive ILM/hyaloid disruptions, respectively (Fig. 13.2a–f). With time a subset of individual tumor cells will begin selective growth to form floating spheres with or without a whitish center. Under the effect of gravity, these vitreous tumors slowly migrate and tend to accumulate inferiorly at the ora serrata. Finally, tumor spread into the aqueous retrohyaloid or subretinal compartments is also associated with the formation of spheres, which differs from the vitreous ones by their ability to rapidly migrate according to gravitational stimuli and their tendency to accumulate inferiorly posterior to the vitreous base or under the ora serrata, respectively. In contrast to vitreous floating seeds, prehyaloid ones (Fig. 13.2i, j) are all located at the same level and tend to coalesce, similarly to ILM-anchored retrohyaloid seeds. Free cobblestone-like (pavimentous) seeds may form in the meniscus of liquid created by partial posterior hyaloid detachment (Fig. 13.2g, h). Finally, a large hyaloid disruption at the tumor base can be followed by a massive transfer of tumor material into the retrohyaloid space creating a position-dependent circular level (Fig. 13.2k–n). When the tumor invades the aqueous fluid of the anterior segment, the semiologic features can be divided into free-floating spheres or tumor cells possibly forming a pseudo-hypopyon or tumor attached to the iris (spheres) and corneal endothelium (pavimentous growth).
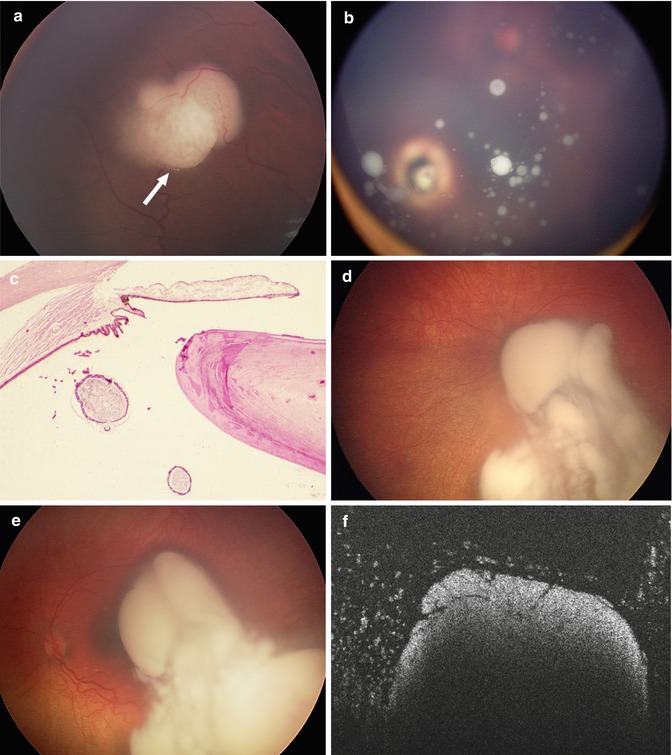
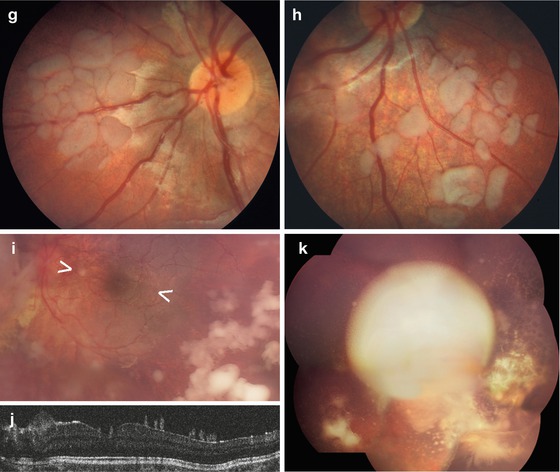
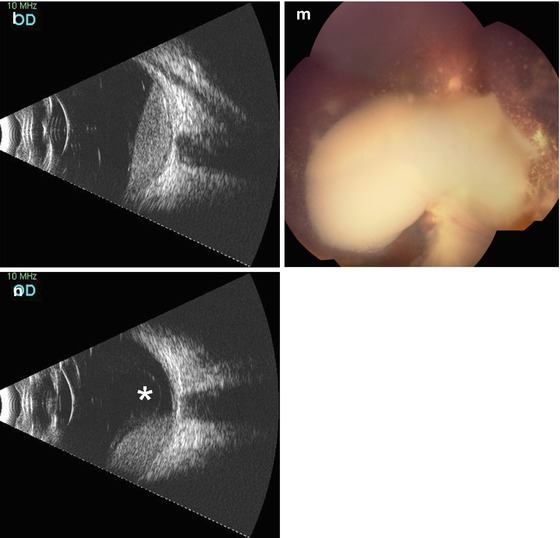
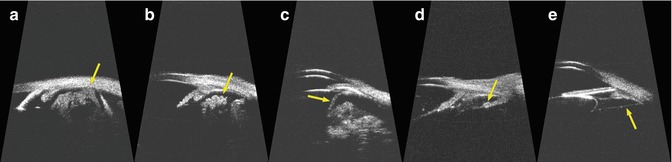
Fig. 13.2
Semiology of endophytic seeding into the vitreous cavity (a–f) and into the retrohyaloid space (g–n). Fine dust visible around the retinal tumor foci (a); multiple spheres with a whitish center (b); H-E staining of spherical seeds showing the active superficial layer and necrotic center (c); fundus RetCam photo (d, e) and OCT (f) of a mobile vitreous cloud; Retrohyaloid seeding forming free pavimentous clones (g, h). Pre-hyaloid seeding forming ovoid partially coalescent clones anchored to the internal face of the hyaloid (i, j). Massive retrohyaloid seeding (retrohyaloid cloud equivalent) with typical position-dependent ophthalmoscopic contours (k, m) and spirit level on ultrasonography (l, n; asterisk: detachment of the posterior hyaloid)
Fig. 13.3
Ultrasonographic biomicroscopy-based ineligibility criteria: (a) tumor, (b) vitreous seeds, and (c) retinal or (e) anterior hyaloid detachment at the entry site; (d) tumor cells in the posterior chamber
13.5 Diagnostic Evaluation, Determination of IViC Eligibility, and Follow-Up
13.5.1 Initial Evaluation: Criteria of Eligibility
The indication for IViC is based on an examination under anesthesia aimed at establishing the eligibility criteria (Box 13.1). A safe pars plana entry site must be determined. Finally, it is imperative to eradicate the retinal source of the seeding.
Box 13.1. Eligibility Criteria for Intravitreal Chemotherapy
The tumoral nature of the seeding is unequivocal and must be differentiated from other mimicking conditions, such as old vitreous hemorrhage or vitritis.
The tumoral viability of the seeding is obvious, which can sometimes require an observation period to document the vitreous growth.
There is a safe pars plana entry site as assessed by ultrasonic biomicroscopy, specifically to exclude: tumor, vitreous seeds, retinal or anterior hyaloid detachment at the entry site, as well as invasion of the anterior and posterior chamber.
The retinal source of the seeding is amenable to treatment.
13.5.2 Follow-Up Evaluation of IViC: Response Monitoring
At each visit the residual vitreous tumor burden is reassessed and IViC carried out every 7–10 days, up to eight injections if a response can be documented, until complete seed fragmentation is observed or complete response is achieved (Fig. 13.4). Complete response is established if the seeds (1) completely disappear (vitreous seeding regression type 0) or convert into (2) refringent and/or calcified residues (vitreous seeding regression type I), (3) amorphous often nonspherical inactive residues (vitreous seeding regression type II), or (4) a combination of the latter two (vitreous seeding regression type III). An injection of consolidation is usually given once a complete response is observed. IViC can be repeated if vitreous recurrence occurs from another source. The timing to complete regression is a matter of weeks to months in case of dust, small localized vitreous spheres, or retrohyaloid seeding, but can reach 1 year in case of big diffuse vitreous spheres or clouds.
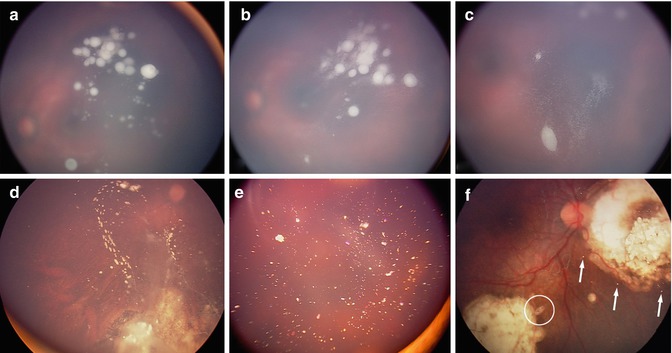
Fig. 13.4
Regression patterns of vitreous seeding: (a) vitreous seeds prior to IViC, (b) partial response following first IViC characterized by a fragmentation of the spheres, (c) further fragmentation after additional injections before complete extinction. Complete response can be classified into complete disappearance (type 0), conversion into either (d) calcified seeds (type Ia), (e) crystalline refringent dust (type Ib), (f) amorphous nonspherical (see asterisk) seeds (type II), or (f) a combination of regression type I and II (type III)
13.5.3 IViC: Treatment and Prognosis
13.5.3.1 Technique
An anterior chamber paracentesis is performed before melphalan injection. A volume of 0.1–0.1–0.15 ml (according to the calculated volume to be injected) of aqueous fluid is aspirated and sent for cytopathologic analysis. A 32-G needle mounted on a tuberculin syringe is then introduced perpendicularly 2.5–3.5 mm from the limbus at the desired meridian opposite to the seeds through the conjunctiva and sclera under microscope viewing until the needle tip reaches the center of the vitreous cavity. The injected dose is 20 μg (0.1 ml) in most cases but can be cumulatively increased by 2–4 μg up to 30 μg (0.15 ml) for each of the following situations: (1) age over 2 years, (2) diffuse nature and/or high density of the seeding, (3) previous intra-arterial exposure to melphalan, and (4) relapse after previous IViC. Upon removal of the needle, three cycles of freeze-thaw cryo-applications are applied at the injection site. The eye is then carefully shaken with forceps in all directions to enable even distribution of the drug. The ocular status at presentation and follow-up is objectively monitored under anesthesia with fundus photography using RetCam (Clarity, Pleasanton, California, USA) and B-scan ultrasonography (OTI Scan 2000 Ophthalmic Technologies). At each visit the residual vitreous tumor burden is reassessed and IViC carried out every 7–10 days up to eight injections through the same meridian, if a response can be documented, until complete seed fragmentation is observed or a complete response achieved (see supra follow-up evaluation).
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


