Treatment
Indication
Complications
Photocoagulation
Primary treatment, consolidation treatment, and for tumor recurrence
Tumor seeding into vitreous, retinal fibrosis and traction, retinal vascular occlusion
Tumors not more than 3 mm in diameter, with no evidence of seeding, and located posterior to the equator
Thermotherapy
Primary treatment, consolidation treatment, and for tumor recurrence
Iris atrophy, focal cataracts, tumor seeding into vitreous, retinal fibrosis and traction, retinal vascular occlusion
Tumors not more than 3 mm in diameter, with no evidence of seeding, and located posterior to the equator
Thermochemotherapy
Consolidation treatment
Iris atrophy, focal cataracts, tumor seeding into vitreous, transient retinal detachment, diffuse choroidal atrophy
Tumors not more than 12 mm in diameter with no evidence of seeding, and located posterior to the equator
Cryotherapy
Primary treatment, consolidation treatment, and for tumor recurrence
Large area of retinal atrophy, transient retinal detachment, retinal hole, retinal detachment
Tumors not more than 3 mm in diameter with no evidence of seeding, and located anterior to the equator. “Cutting cryo” for posterior tumors
Brachytherapy
Primary treatment, residual tumor following photocoagulation/thermotherapy/thermochemotherap/cryotherapy, and for tumor recurrence
Radiation retinopathy, radiation optic neuropathy
Tumor less than 15 mm in diameter
Presence of diffuse vitreous seeding is contraindication
10.2.2 Focal Primary Treatment
Primary treatment refers to focal treatment employed as the sole therapy for a retinoblastoma lesion, typically for very small tumors (group A).
10.2.3 Chemoreduction
The term “chemoreduction” is used to describe the induction of tumor shrinkage with primary intravenous chemotherapy, followed by subsequent consolidation treatment with focal therapies, and less commonly with EBR.
10.2.4 Consolidation Treatment
In most centers, focal treatment is utilized most frequently following primary intravenous chemotherapy (i.e., chemoreduction) for group B–D tumors. The term “consolidation,” as used in oncology, is a therapy that is used in tandem with primary therapy to “mop up” or eliminate the tumor cells that were resistant to, or were not inactivated by, the primary therapy. In most other childhood tumors, consolidation involves switching treatment modalities entirely or at least changing to different agents and/or doses of the primary modality. In the case of intraocular retinoblastoma, focal consolidation consists of direct laser photocoagulation, thermotherapy, cryotherapy, or brachytherapy.
10.2.5 Photocoagulation
Described by Meyer-Swickerath in 1949, photocoagulation involves heating of the tumor to temperatures above 65 °C [1].
10.2.6 Hyperthermia
Hyperthermia implies raising the tumor temperature to 42–45 °C. Hyperthermia can be induced by laser, microwave, ultrasound, a localized current field, or ferromagnetic thermoseeds.
10.2.7 Thermotherapy
During the thermotherapy, the tumor is heated to a temperature of 45–60 °C. Oosterhuis and coworkers in 1994 introduced thermotherapy for choroidal melanomas using an infrared diode laser through the pupil (transpupillary thermotherapy [TTT]) [2]. Increased depth of tumor necrosis was achieved with TTT as compared with photocoagulation. Unlike hyperthermia, the cytotoxic effects of TTT are irreversible. Transpupillary thermotherapy can be achieved in retinoblastoma tumors using the 810 nm diode laser if the continuous mode is used to treat each spot for 45–60 s.
10.3 Focal Primary Treatment
Group A eyes with small intraretinal lesions away from critical structures are ideal candidates for focal primary therapy such as direct laser photocoagulation or cryotherapy. Larger focal tumors may be candidates for brachytherapy, and the indication for plaque radiotherapy is discussed below. Tumor foci that have not been treated with systemic chemotherapy may be more fragile and sensitive to intense energy density from the laser. For this reason, small spot size, high power, and prolonged burn duration, all of which contribute to increased power density, should be used with caution to avoid sudden mechanical tumor disruption and dissemination.
10.4 Focal Consolidation Treatment
10.4.1 Photocoagulation with Argon Green Laser (532 nm)
10.4.1.1 Background
The argon 532 nm (green) laser is particularly useful for very small retinoblastoma tumors (1.5 mm or less) or for focal consolidation after at least one cycle of systemic chemotherapy. As with other uses of retinal photocoagulation, focal consolidation should not be attempted if the retina containing the lesion is detached. We have found that the argon laser midrange visible (532 nm) wavelength is more readily absorbed in the nonpigmented retinoblastoma tissue than the longer wavelength infrared 810 nm diode laser, which becomes a factor in thick tumors or those occurring over calcified scars. The margins of the treated zone when using the argon laser are also easier to control than with the diode laser. Its main disadvantage when compared to the diode laser is the small spot size. Care must be taken to increase the power density judiciously within the small spot to avoid tumor dissemination or hemorrhages. Tumor disruption may occur in a small spot if the power out of the laser exceeds 700–800 mw for more than 0.3–0.4 s.
10.4.1.2 Technique
The 532 nm green laser is available as a tabletop solid state laser with an indirect laser delivery system that works best for transpupillary laser applications under general anesthesia. The desirable end point for the ophthalmologist is a gentle white spot generated at the boundary between normal retina and tumor edge (Fig. 10.1). The power is initially set between 250 and 350 mw for 0.3–0.5 s. Laser burns are initially placed at the edge of the lesion, half-on and half-off the tumor. The power and/or burn duration is slowly increased until a clear reaction is achieved. Punctate hemorrhage within the treatment spot is a sign that the power density is near the maximum tolerated levels.
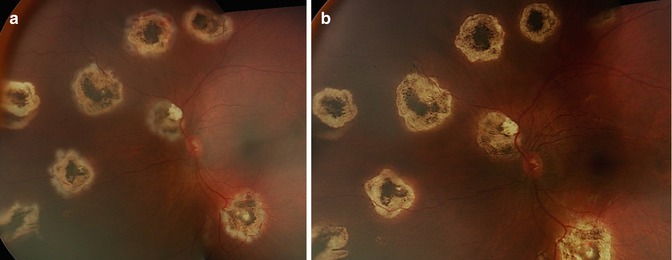
Fig. 10.1
Image taken immediately after the third consolidation laser photocoagulation (a). Each lesion was covered with laser burns. Note the distinct gentle white burn at the lesion edge. There is differential energy uptake. Three weeks later, all lesions are all flat with no clinical evidence of active disease (b)
Once the appropriate power level is set, the edge of the tumor is treated with overlapping burns to establish the perimeter of the lesion. Subsequently the entire lesion should be treated with burns having the same overlap. In the central thicker portions of the tumor, a visible whitening reaction following treatment may not be present. However, neither the power nor the burn duration should be increased once the parameters have been established.
10.4.1.3 Frequency of Treatment
Typically the treatment is repeated every 3–4 weeks, immediately before the next cycle of chemotherapy. A 2–4 week interval can be adopted if the course of intravenous chemotherapy has been completed. Edge tumor recurrence may appear if the laser consolidation process was insufficient, typically within the first 6 months after the last laser session (rarely up to 2 years) (Fig. 10.2).
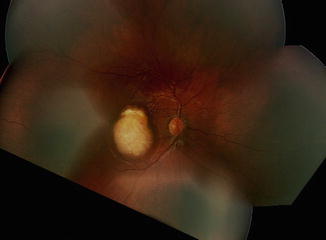
Fig. 10.2
Edge regrowth 8 weeks after the last laser treatment that almost covers the original flat chorioretinal scar. This child missed one follow-up EUA
10.4.1.4 Mechanism of Action
When photocoagulation is used on retinoblastoma lesions and the patient subsequently receives planned systemic chemotherapy (e.g., carboplatin) within 24 h, two tumor-destroying mechanisms may come into play. The first and the most important is direct tumor cell destruction generated by temperatures in excess of 65–70 °C within the treatment spot. The second mechanism occurs in the “donut” or ring of tissue extending for several millimeters outside the laser spot. Heat radiating out from the central spot increases the temperature to the thermotherapy range between 45 and 60 °C. In this region, there is a synergism with the carboplatin, assuming an adequate level of carboplatin is achieved in the tumor. To take advantage of the latter mechanism, we typically perform laser treatment within 24 h of the next cycle of intravenous chemotherapy.
10.4.1.5 Recommendations
In Los Angeles, our treatment protocol requires that each lesion be treated completely with laser on at least three occasions, 2–4 weeks apart. In our experience, even a flat chorioretinal scar achieved after one laser session cannot be considered sterilized. Larger lesions should be lasered at sequential examinations (minimum of three sessions) until the regressed tumor is either flat (type IV scar) or completely calcified (type I). Fleshy type II regression should be lasered until you achieve a type I/IV scar or until you begin to notice retinal contraction. Small areas of type II regression may be left untreated immediately adjacent to the optic nerve or fovea, although the risk for tumor recurrence is always higher with type II vs. type I (or type IV) scars.
10.4.2 Photocoagulation with Diode Laser (810 nm)
10.4.2.1 Background
The 810 nm diode laser is most effective when there is intact RPE beneath the tumor. Through a 28D lens, the indirect ophthalmoscope delivery system offers a spot size of 0.35 mm (small spot) and 1.4 mm (large spot). We typically use the large spot indirect system, which provides improved safety and convenience for treating larger tumors versus the argon laser. Safety comes from the reduced likelihood of concentrated power intensity in a small spot creating tumor dissemination. The larger spot size as compared with argon saves treatment time, thus conferring convenience. It is also our impression that the depth of treatment with the diode laser is greater than the argon laser. However, it is more difficult to control the size of the burn with the diode laser, and care is warranted near the optic nerve and fovea.
10.4.2.2 Technique
The delivery technique is similar to that with argon green laser photocoagulation. The entire tumor is treated with overlap of the spots similar to that described above for the argon 532 nm laser. The initial power settings with the diode laser, especially when the large spot is used, are somewhat higher than for the argon laser. We generally select an initial setting of 300 mw for peripheral and macular lesions undergoing primary therapy and 400–500 mw for large tumors undergoing chemoreduction. If there is little color change induced at the initial power settings for these larger tumors, it is possible to increase the power up to 800 mw, provided that the surgeon is carefully monitoring for complications. The power settings will vary for each patient and for each tumor because of the degree of pigmentation underlying the lesion(s). As with the argon laser, both the power and burn duration can be increased incrementally until the appropriate end point is reached. We typically leave the duration of the treatment on the longest setting (9,000 ms) and set the interval to 50 ms; with these parameters the laser is essentially being used in continuous mode and the surgeon can control the duration of each spot treatment with the foot pedal. Using the diode laser in this manner allows the surgeon to use the diode laser for photocoagulation (1–10 s) or possibly thermotherapy (30–50 s).
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


